Arthrogryposis Multiplex Congenita: Comprehensive Surgical Management

Key Takeaway
Arthrogryposis multiplex congenita (AMC) represents a complex syndrome of multiple congenital joint contractures driven by fetal akinesia. Orthopaedic management prioritizes achieving independent ambulation and functional upper extremities for activities of daily living. Treatment involves early serial casting followed by targeted surgical interventions, including radical soft-tissue releases, osteotomies, and tendon transfers, meticulously timed to optimize biomechanical alignment and prevent recurrence during skeletal growth.
Introduction and Pathophysiology
Arthrogryposis multiplex congenita (AMC), more accurately termed multiple congenital contractures, encompasses a heterogeneous group of over 150 unrelated disorders sharing a common phenotypic endpoint: nonprogressive, multiple rigid joint contractures present at birth. Rather than a discrete clinical entity, AMC is a symptom complex resulting from fetal akinesia (limited intrauterine movement).
The underlying etiology of decreased fetal movement can be broadly categorized into neurogenic, myogenic, skeletal, or environmental factors. Regardless of the primary insult, the lack of normal joint excursion during embryogenesis leads to severe periarticular fibrosis and capsular contracture. Histological analysis of the affected extremities reveals profound myopathic and neuropathic features, characterized by a markedly diminished muscle mass that is extensively replaced by dense fibrotic tissue and fat.
The incidence of AMC is approximately 1 in 3,000 live births. Because of the vast array of associated syndromes—ranging from classic Amyoplasia (sporadic) to Distal Arthrogryposis (autosomal dominant) and Diastrophic Dysplasia (autosomal recessive)—a comprehensive genetic evaluation is mandatory for all affected patients.
Clinical Presentation and Diagnostic Evaluation
Patients with classic arthrogryposis (amyoplasia) typically present with quadrimelic involvement. The extremities appear cylindrical, fusiform, or cone-shaped, lacking normal skin creases and subcutaneous tissue. Sensation and intellect remain entirely normal, which is a critical factor in their excellent potential for rehabilitation and functional adaptation.
Fig. 31-52 Newborn with arthrogryposis multiplex congenita. Note the classic orthopaedic presentation: congenital dislocation of the knees, teratological clubfeet, internal rotation contractures of the shoulder, extension contractures of the elbow, and severe flexion contractures of the wrist.
Diagnostic Modalities
- Clinical Examination: The gold standard for establishing the phenotypic diagnosis and mapping the extent of rigid fibrous ankylosis.
- Neurological and Neuromuscular Assessment: Electromyography (EMG), nerve conduction studies, serum muscle enzyme tests, and muscle biopsy are utilized to differentiate between neurogenic and myogenic etiologies.
- Radiographic Evaluation: Essential for assessing skeletal integrity, identifying teratological dislocations of the hips or knees, and screening for scoliosis (present in 10% to 30% of patients).
Principles of Orthopaedic Management
The overarching prognosis for children with AMC is relatively good, provided that treatment is aggressively focused on maximizing functional independence. While the disease itself is nonprogressive, certain contractures may appear to worsen between 12 and 18 months of age due to differential growth between the skeleton and the fibrotic soft tissues.
According to Tachdjian, the orthopaedic management of AMC is anchored by two primary goals:
1. Independent Ambulation: Requires the creation of a plantigrade, braceable foot and the correction of lower extremity alignment.
2. Independent Upper Extremity Function: Focused on enabling activities of daily living (ADLs), particularly hand-to-mouth function and perineal care.
Clinical Pearl: Early intervention is paramount. An immediate postnatal program of passive stretching exercises and serial splinting with custom thermoplastic orthoses is recommended. While physical therapy rarely provides permanent correction, it stretches the soft tissues, reduces the magnitude of subsequent surgical releases, and prevents secondary contractures.
Surgical Timing
- Knees and Hips: Surgical intervention should ideally be performed between 6 to 9 months of age.
- Feet: Surgery should be timed closely to when the child normally begins to pull to a stand (10 to 12 months) to utilize weight-bearing as a dynamic force against recurrence.
- Upper Extremities: Delayed until ambulation is securely achieved (typically 3 to 4 years of age). Early upper extremity surgery can disrupt the child's use of their arms for crawling and balance.
Spinal Deformity in Arthrogryposis
Scoliosis occurs in up to 30% of patients with AMC. The curves are often rigid, neuromuscular in nature, and highly resistant to orthotic management. Progressive curves require surgical stabilization to maintain truncal balance and sitting posture. Severe, rigid deformities may necessitate combined anterior and posterior approaches to achieve adequate correction and fusion.

Fig. 31-51A Correction of severe arthrogrypotic scoliosis utilizing anterior fusion with Dwyer instrumentation.

Fig. 31-51B Subsequent posterior fusion utilizing Luque rods to provide rigid segmental stabilization.
Lower Extremity Management
The Arthrogrypotic Foot
The most common foot deformities in AMC are rigid teratological clubfoot (talipes equinovarus) and congenital vertical talus. The surgical goal is strictly functional: converting a rigid, deformed foot into a rigid, plantigrade foot that can accommodate standard orthoses. A biomechanically "normal" foot is an unrealistic expectation.
Surgical Progression:
1. Soft-Tissue Release: Following a plateau in serial casting, an extensive posteromedial and posterolateral release is indicated. This must be far more radical than a standard idiopathic clubfoot release, often requiring complete capsulotomies of the subtalar, talonavicular, and calcaneocuboid joints.
2. Talectomy (Astragalectomy): Indicated for severe, rigid deformities that cannot be corrected by soft-tissue release alone, or for recurrent clubfeet in young children. Fusing the calcaneocuboid joint concurrently with talectomy helps prevent progressive midfoot adduction.
3. Cancellectomy of the Talus and Cuboid (Verebelyi-Ogston/Gross Technique): A joint-sparing alternative to talectomy for severe midfoot/hindfoot rigidity.
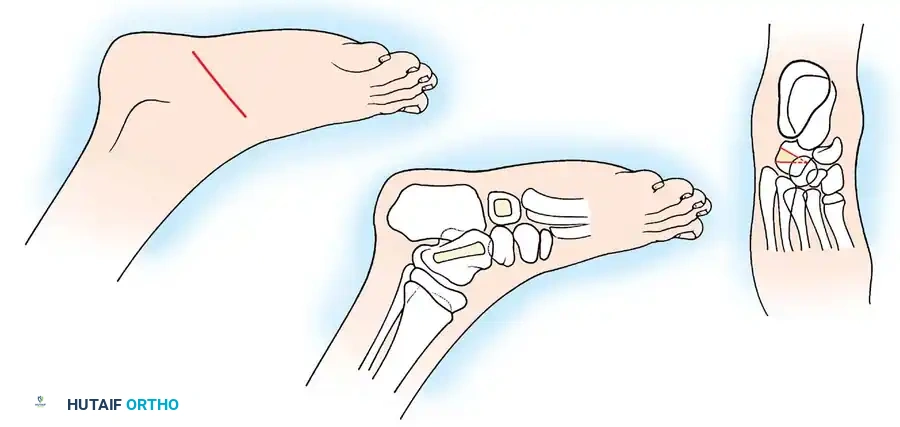
Fig. 31-53 Cancellectomy of the talus and cuboid. (A) Incision approach. (B) Creation of cortical windows in the talus and cuboid to expose and curette the cancellous bone. (C) Closing wedge osteotomy effect achieved by manual manipulation, collapsing the decancellated bones to correct the deformity.
Cancellectomy Technique:
* A window is created in the dorsal cortex of the cuboid and the lateral cortex of the neck and body of the talus.
* All cancellous bone is meticulously curetted out, leaving only an empty cortical shell.
* The deformity is then acutely corrected by manual manipulation, crushing the cortical shells into the newly created void, effectively acting as a closing wedge osteotomy without sacrificing the articular cartilage.
For adolescents near skeletal maturity with recurrent rigid deformities, a Triple Arthrodesis remains the definitive salvage procedure. Gradual correction using circular-frame external fixators (e.g., Ilizarov) is an option but is technically demanding due to the poor skin envelope and osteopenic bone.
The Arthrogrypotic Knee
Knee deformities present as either severe flexion or extension contractures.
Flexion Contractures:
Ambulation is generally possible with a residual knee flexion contracture of 15 to 20 degrees. If serial casting fails to achieve this by 6 to 12 months of age, surgical release is required.
* Soft-Tissue Release: Involves posterior medial and lateral hamstring lengthenings combined with extensive posterior knee capsulotomies.
* Approach: Use vertical medial and lateral posterior incisions, or an extensile posterolateral Henry incision.
Surgical Warning: Never use S-shaped incisions in the popliteal fossa for arthrogrypotic patients. The acute extension of the knee following correction places excessive tension on the skin flaps, inevitably leading to severe wound necrosis and breakdown.
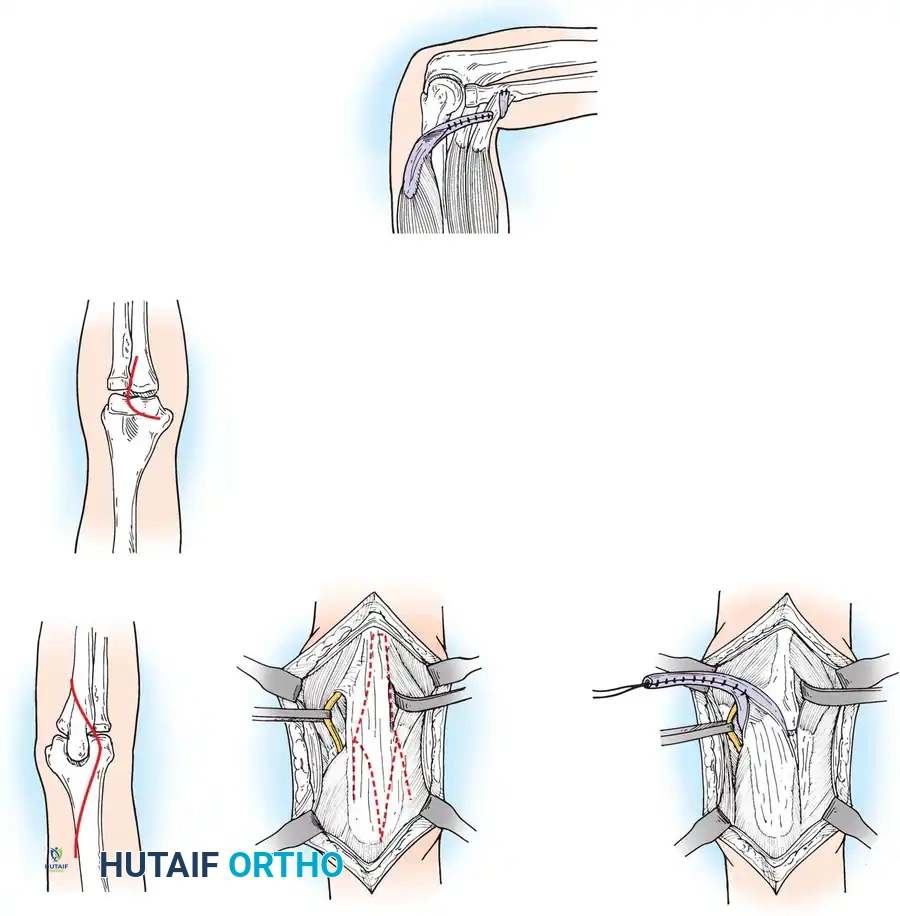
Diagram illustrating the extensive posterior capsular release and hamstring lengthening required for severe knee flexion contractures.
- Bony Correction: Supracondylar extension osteotomy of the distal femur is reserved for older children. If performed before skeletal maturity, DelBello and Watts demonstrated a recurrence rate of 1 degree per month due to anterior physeal tethering. Femoral shortening may be required simultaneously to prevent traction injury to the sciatic nerve and popliteal vessels.
Extension Contractures:
Hyperextension deformities are driven by a fibrotic, contracted quadriceps mechanism. If unresponsive to casting, a formal Quadricepsplasty (V-Y lengthening of the quadriceps tendon and release of the vastus intermedius) is indicated to allow passive flexion for sitting.
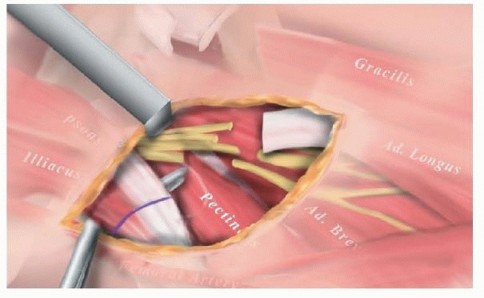
The Arthrogrypotic Hip
The hip is involved in approximately 80% of AMC patients. Mild flexion contractures are common and usually accommodated by a compensatory increase in lumbar lordosis. However, fixed flexion contractures exceeding 45 degrees require surgical release (e.g., psoas and rectus femoris tenotomies) to allow upright posture.
Hip Dislocation:
Occurring in 15% to 30% of patients, teratological hip dislocation management is highly nuanced.
* Unilateral Dislocation: Must always be reduced surgically to prevent severe pelvic obliquity and secondary structural scoliosis.
* Bilateral Dislocation: Historically left unreduced due to high stiffness rates. However, modern literature (Szöke et al.) advocates for early open reduction (3 to 6 months of age) utilizing a medial approach.
* Late Presentation (12-36 months): Requires a comprehensive one-stage open reduction via an anterior approach, combined with primary femoral shortening (to decompress the joint) and a pelvic osteotomy (e.g., Dega or Pemberton) to provide adequate acetabular coverage. Postoperative spica cast immobilization should be strictly limited to 6 to 8 weeks to prevent irreversible joint stiffness.
Upper Extremity Management
The primary goal of upper extremity surgery is to facilitate bimanual function and independent ADLs. Surgery is delayed until 3 to 4 years of age, ensuring the child has mastered ambulation. However, interventions should not be delayed beyond 8 years of age, as established compensatory motor patterns become too deeply ingrained to adapt to the new biomechanical alignment.
The Shoulder
The classic arthrogrypotic shoulder is rigidly adducted and internally rotated. While weakness and stiffness at the glenohumeral joint rarely require intervention, the fixed internal rotation is a profound functional block, preventing the hand from reaching the mouth or perineum.
Surgical Management:
A Proximal Humeral Derotation Osteotomy is the procedure of choice. The humerus is osteotomized proximal to the deltoid insertion and externally rotated to place the hand in a functional sagittal plane.
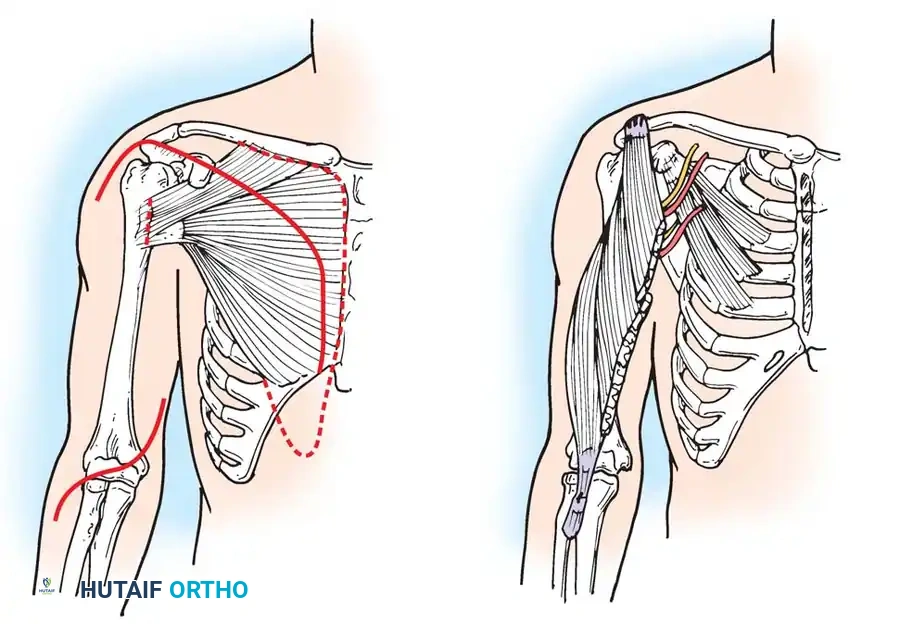
Diagrammatic representation of muscle transfers and releases around the shoulder girdle, often utilized in conjunction with rotational osteotomies to optimize upper extremity positioning.
The Elbow
Elbow deformities dictate the functional capacity of the entire upper limb.
* Flexion Contractures: A stiff, flexed elbow is highly functional for feeding and facial hygiene. Surgery is rarely indicated.
* Extension Contractures: A fixed extended elbow, particularly if bilateral, is a devastating impairment. The patient cannot feed themselves or perform basic hygiene.
Surgical Options for the Extended Elbow:
The goal is to achieve a functional range of passive motion and, if possible, active elbow flexion.
1. Posterior Release and Tricepsplasty: The fibrotic triceps tendon is lengthened (often via a V-Y advancement) and the posterior capsule is released to allow passive flexion.
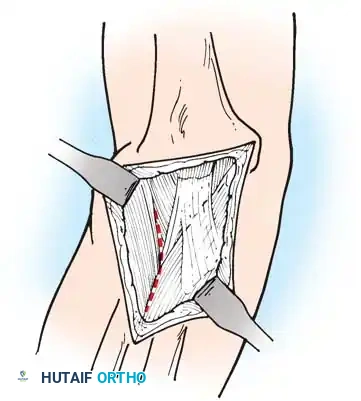
Surgical approach for posterior elbow release and tricepsplasty, demonstrating the exposure of the fibrotic triceps mechanism.
- Tendon Transfers for Active Flexion: Once passive motion is achieved, active flexion can be restored if suitable donor muscles are available.
- Triceps Transfer: If the triceps has residual active power, it can be routed anteriorly to substitute for the absent biceps/brachialis.
- Pectoralis Major Transfer (Clark's Procedure): The sternocostal head of the pectoralis major is mobilized and transferred to the biceps tendon or proximal ulna.
- Steindler Flexorplasty: Proximal advancement of the flexor-pronator mass from the medial epicondyle to the anterior humerus, utilizing the wrist flexors to drive elbow flexion.
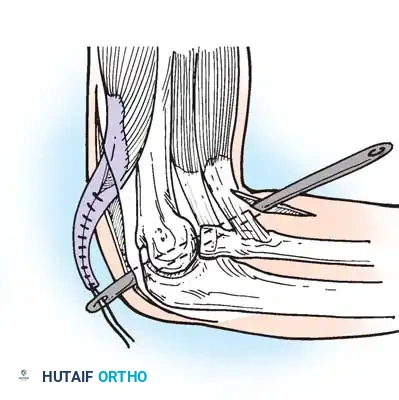
Illustration of tendon transfer techniques around the elbow to restore active flexion following the release of a rigid extension contracture.
The Wrist and Hand
The arthrogrypotic wrist is typically fixed in severe palmar flexion and ulnar deviation, with rigidly flexed fingers and an adducted, clasped thumb.
Management Strategy:
* Wrist: Proximal row carpectomy or wedge osteotomies of the carpus can place the wrist in a neutral or slightly extended position, significantly improving the mechanical advantage of the extrinsic finger flexors. In older adolescents, a formal radiocarpal arthrodesis provides a stable, permanent platform.
* Thumb: A clasped thumb severely limits grasp. Release of the adductor pollicis, combined with a Z-plasty of the first web space, is often required to open the first commissure and allow for lateral pinch.
Clinical Pearl: When planning bilateral upper extremity surgery, the dominant limb is typically optimized for hand-to-mouth activities (requiring elbow flexion and neutral/supinated forearm), while the non-dominant limb is optimized for perineal care and pushing up from a chair (requiring elbow extension and pronation).
Postoperative Rehabilitation
The success of any surgical intervention in AMC is inextricably linked to the postoperative rehabilitation protocol. Due to the dense fibrofatty nature of the tissues, the propensity for recurrence is exceptionally high. Continuous nighttime splinting is often required until skeletal maturity. Physical therapy must focus on active-assisted range of motion, as aggressive passive stretching of a surgically released joint can lead to microtrauma, heterotopic ossification, and paradoxical increased stiffness.
📚 Medical References
- Akazawa H, Oda K, Mitani S, et al: Surgical management of hip dislocation in children with arthrogryposis multiplex congenita, J Bone Joint Surg 80B:636, 1998.
- Atkins RM, Bell MJ, Sharrard WJ: Arthrogryposis: pectoralis major transfer for paralysis of elbow fl exion in children, J Bone Joint Surg 67B:640, 1985.
- Axt MW, Niethard FU, Döderlein L, et al: Principles of treatment of the upper extremity in arthrogryposis multiplex congenita type I, J Pediatr Orthop 6:179, 1997.
- Banker BQ: Neuropathologic aspects of arthrogryposis multiplex congenita, Clin Orthop Relat Res 194:30, 1985.
- Bayne LG: Hand assessment and management in arthrogryposis multiplex congenita, Clin Orthop Relat Res 194:68, 1985.
- Beals RK: The distal arthrogryposes: a new classifi cation of peripheral contractures, Clin Orthop Relat Res 435:203, 2005.
- Bernstein RM: Arthrogryposis and amyoplasia, J Am Acad Orthop Surg 10:417, 2002.
- Brown LM, Robson MJ, Sharrard WJW: The pathophysiology of arthrogryposis multiplex congenita neurologica, J Bone Joint Surg 62B:291, 1980.
- Carlson WO, Speck GJ, Vicari V, et al: Arthrogryposis multiplex congenita: a long-term follow-up study, Clin Orthop Relat Res 194:115, 1985.
- Cassis N, Capdevila R: Talectomy for clubfoot in arthrogryposis, J Pediatr Orthop 20:652, 2000.
- Choi IH, Yang MS, Chung CY, et al: The treatment of recurrent arthrogrypotic clubfoot in children by the Ilizarov method: a preliminary report, J Bone Joint Surg 83B:731, 2001.
- DelBello DA, Watts HG: Distal femoral
You Might Also Like