Mastering Open Reduction and Internal Fixation of Phalangeal Fractures and PIP Joint Dislocations

Key Takeaway
Open reduction and internal fixation (ORIF) of phalangeal fractures is indicated for unstable, rotated, or intra-articular patterns. Techniques range from the Pratt method of retrograde pinning to the Belsky-Eaton intramedullary technique. For complex proximal interphalangeal (PIP) joint fracture-dislocations with significant volar lip comminution, advanced reconstructions such as the hemi-hamate osteoarticular autograft restore joint congruity and stability, permitting early active motion and preventing chronic dorsal subluxation.
BIOMECHANICS AND INDICATIONS FOR OPEN REDUCTION
Phalangeal fractures are among the most common injuries evaluated by orthopedic surgeons, yet their management requires a profound understanding of hand biomechanics. The delicate interplay between the intrinsic muscles (interossei and lumbricals) and the extrinsic tendons (flexor digitorum superficialis/profundus and extensor digitorum communis) creates predictable deforming forces. Proximal phalanx fractures typically apex volar due to the proximal pull of the interossei on the base and the distal pull of the central slip on the middle phalanx.
While many phalangeal fractures can be managed non-operatively with buddy taping or functional splinting, surgical intervention via Open Reduction and Internal Fixation (ORIF) or closed reduction with percutaneous pinning (CRPP) is strictly indicated for:
* Fractures with unacceptable angular or rotational deformity (scissoring of digits).
* Unstable oblique or spiral fractures that shorten under the compressive forces of the flexor tendons.
* Intra-articular fractures with step-offs greater than 1-2 mm.
* Fractures with significant segmental comminution or bone loss.
* Complex proximal interphalangeal (PIP) joint fracture-dislocations.
Surgical Warning: Rotational malalignment is the least tolerated deformity in phalangeal fractures. Even 5 degrees of malrotation at the proximal phalanx can lead to 1.5 cm of digital overlap at the fingertips during composite flexion. Always assess rotation clinically with the metacarpophalangeal (MCP) and PIP joints flexed prior to final fixation.
SURGICAL APPROACHES TO PHALANGEAL FRACTURES
The Pratt Technique: Open Reduction and Retrograde Pinning
For transverse or short oblique fractures of the proximal or middle phalanx that cannot be reduced closed, the Pratt technique offers a reliable method of direct visualization and stabilization.
Surgical Steps:
1. Exposure: Utilize a dorsal longitudinal or slightly curved incision over the fractured phalanx. Expose the extensor tendon mechanism.
2. Tendon Incision: Incise the extensor tendon longitudinally precisely in its center. Carefully retract the split tendon to each side to expose the underlying fracture site.
3. Retrograde Drilling: Under direct vision, drill a Kirschner wire (K-wire) into the distal fragment.
4. Reduction and Fixation: Anatomically reduce the fracture. Once reduced, drive the K-wire retrograde across the fracture site into the proximal fragment.
5. Deformity Correction: Ensure absolute correction of any rotational deformity. While minor shortening may be biomechanically acceptable, rotational malalignment is not.
6. Closure: Meticulously repair the extensor tendon with a fine non-absorbable or slowly absorbable suture (e.g., 4-0 or 5-0).
Figure 67-45A: Crush injury to the small finger resulting in a middle phalangeal fracture.

Figure 67-45B: AP radiograph demonstrating the inherently unstable nature of the fracture.

Figure 67-45C: Lateral radiograph confirming displacement requiring stabilization.

Figure 67-45D: Postoperative AP radiograph showing the Pratt technique of crossed Kirschner wire fixation providing excellent alignment.

Figure 67-45E: Postoperative lateral radiograph confirming concentric reduction and stability.
Postoperative Protocol:
Support the finger in the intrinsic-plus position (position of function: MCP joints flexed 70-90 degrees, PIP/DIP joints fully extended) and the wrist in 20-30 degrees of extension. The finger is splinted for 2 to 3 weeks, allowing protected early range of motion. The K-wires are typically removed in 3 to 4 weeks once clinical callus is evident.
Closed Reduction and Percutaneous Pinning (CRPP)
Sometimes an unstable oblique fracture of a middle or proximal phalanx can be treated by closed reduction and percutaneous pinning with a K-wire inserted across the fracture.
Clinical Pearl: The K-wire should be inserted midlaterally. This trajectory is critical to avoid tethering the extensor hood dorsally or injuring the flexor tendon apparatus volarly, which would severely compromise postoperative digital excursion.
The Belsky-Eaton Intramedullary Pinning Technique
Belsky and Eaton described a highly effective, minimally invasive technique for pinning multiple proximal phalangeal fractures, particularly transverse or short oblique patterns.
Surgical Steps:
1. Positioning: The fractured phalanx is held anatomically reduced with the MCP joint flexed to 90 degrees. Flexing the MCP joint tightens the collateral ligaments, utilizing ligamentotaxis to aid in reduction, and pulls the extensor mechanism distally, moving it out of the trajectory of the pin.
2. Pin Insertion: A single K-wire (typically 0.045 or 0.062 inch) is drilled from the dorsal aspect of the metacarpal head, passing across the flexed MCP joint.
3. Intramedullary Passage: The wire is advanced along the medullary canal of the proximal phalanx to cross the fracture site.
4. Joint Protection: The wire must not cross the PIP joint. It should be left exposed proximally (bent and cut outside the skin) to facilitate easy removal in the clinic at 3 to 4 weeks.

Figure 67-46A: Markedly unstable proximal phalangeal fracture.

Figure 67-46B: Belsky-Eaton pinning technique. The fracture is treated by percutaneous pinning across the MCP joint. Note the MCP joint is flexed at least 60 to 70 degrees, and the PIP joint is intentionally not crossed.
INTRA-ARTICULAR PHALANGEAL BASE FRACTURES
Intra-articular fractures of the proximal phalangeal base present a unique challenge. The articular surface must be restored to prevent post-traumatic osteoarthritis and stiffness.
When restoration of near-anatomical joint surface articulation is necessary and early motion is desirable, open reduction and internal fixation utilizing minifragment screws (1.0 mm to 1.5 mm) is preferable. Lag screw technique provides absolute stability, allowing for immediate postoperative mobilization.

Figure 67-47A: Comminuted intra-articular fracture in the middle finger proximal phalanx base of an avid tennis player.

Figure 67-47B: Successful treatment achieved via precise lag screw fixation, restoring the articular congruity.
Surgical Pitfall: Open or severely comminuted phalangeal fractures, especially of the proximal phalanx, may be unsuitable for internal fixation using traditional methods due to the risk of devascularizing small fragments. In such cases, external fixation using a mini external fixator is highly appropriate to maintain length and alignment via ligamentotaxis.
PROXIMAL INTERPHALANGEAL (PIP) JOINT FRACTURE-DISLOCATIONS
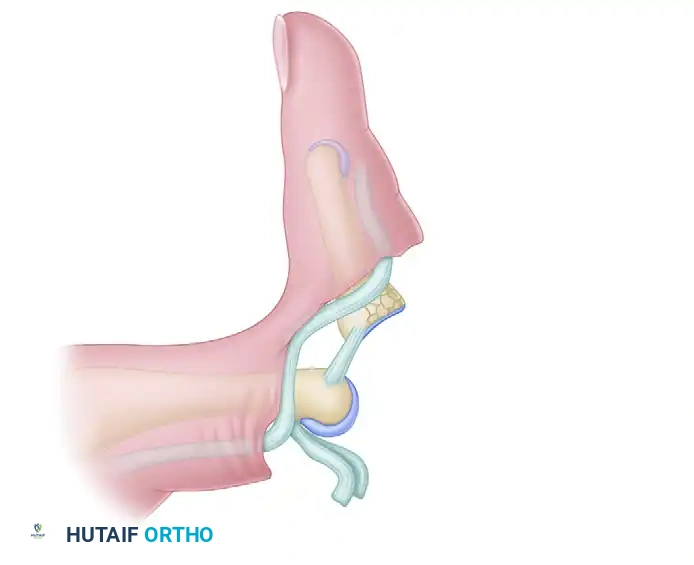
A PIP joint fracture-dislocation is a devastating injury that, as a rule, results in an unstable dorsal displacement of the middle phalanx. This pathoanatomy is caused by the disruption of the attachment of the volar fibrocartilaginous plate, often taking a fragment of the volar lip of the middle phalanx with it.
Treatment Algorithm Based on Articular Involvement
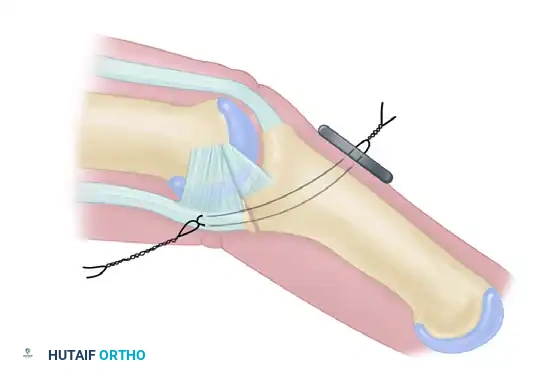
- Large Single Fragment (>50% Articular Surface): If a large, single volar fragment involving more than 50% of the joint surface is present, ORIF is indicated. Fixation can be achieved with one or more K-wires, minifragment screws, or a wire loop pullout technique.
- Small Fragments (<50% Articular Surface): If the fragment or fragments include less than 50% of the articular surface, the technique described by McElfresh, Dobyns, and O’Brien is preferred. This utilizes an extension block splint, allowing active flexion of the PIP joint while preventing the terminal extension that leads to dorsal subluxation. This gives satisfactory results, especially in cases without gross displacement.
- Chronic/Persistent Subluxation (≤40% Articular Surface): For persistent dorsal fracture-dislocations with preserved condyles of the proximal phalanx and a volar defect of 40% or less, the volar plate arthroplasty method of Eaton and Malerich may be used. They reported successful use of this technique in old, healed, displaced fractures even 2 years after injury.
Advanced Reconstruction: The Hemi-Hamate Osteoarticular Autograft
An alternative, highly advanced treatment involves the reconstruction of the middle phalanx volar lip using an autogenous osteoarticular graft.
Indications:
* Persistent dorsal subluxation of the PIP joint with 30 degrees of PIP joint flexion.
* Delayed presentations of PIP joint dorsal fracture subluxations.
* Middle phalanx volar lip fractures exceeding 50% of the articular surface with severe comminution.
* Failed volar plate arthroplasty.
* Failed dynamic traction or extension block splinting.
Biomechanical Rationale:
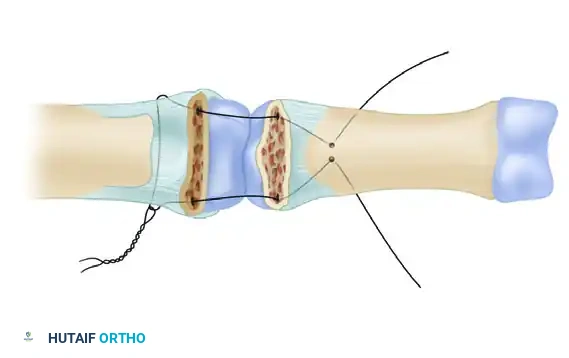
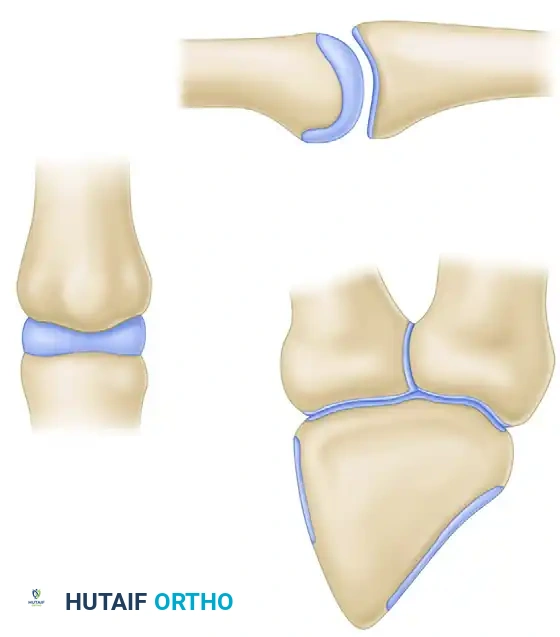
A size-matched segment of the distal hamate articular surface is carefully shaped to match the comminuted contour of the middle phalanx. The distal hamate (articulating with the base of the 4th and 5th metacarpals) possesses a central ridge that perfectly mimics the median ridge of the middle phalangeal base, providing exceptional coronal plane stability.

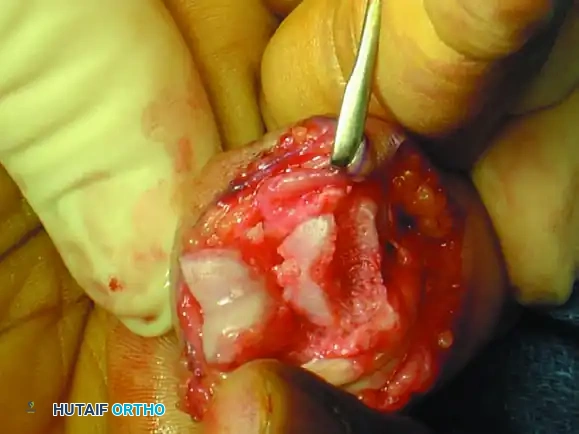
Figure 67-49A: Persistent dorsal PIP joint subluxation with a nonreconstructible middle phalangeal volar lip fracture.

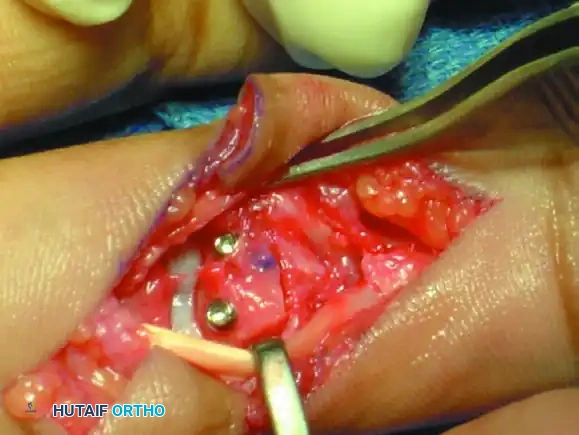
Figure 67-49B: Volar exposure of the middle phalangeal base and geometrical preparation of the defect to receive the graft.

Figure 67-49C: Intraoperative fluoroscopic view of the distal hamate donor site.

Figure 67-49D: Fixation of the hemi-hamate graft with two minifragment screws to replicate the middle phalangeal base concavity.

Figure 67-49E: Radiograph demonstrating a concentric joint without collapse or dorsal subluxation at 2 years after surgery.
Step-by-Step Hemi-Hamate Surgical Technique
- Volar Approach: A volar Bruner or midlateral incision is made to approach the PIP joint. The flexor tendon sheath is opened, and the A3 pulley is released. The flexor tendons are retracted laterally.
- Joint Exposure ("Shotgunning"): The volar plate is released distally. The collateral ligaments are sharply released from their proximal attachments to allow the joint to be hyperextended or "shotgunned." This provides unparalleled visualization of the articular defect on the middle phalanx.
- **
Associated Surgical & Radiographic Imaging










You Might Also Like


