Complications of Hand Fractures: Reconstructive Hierarchy, Malunion, and Mallet Fracture Fixation

Key Takeaway
Hand fracture complications, including malunion and tendon adhesion, require a strict reconstructive hierarchy prioritizing soft tissue coverage and sensation before osseous repair. Malunion disrupts intrinsic muscle balance, necessitating precise surgical correction. For intra-articular mallet fractures, open reduction and internal fixation utilizing a transarticular Kirschner wire and pull-out suture technique restores joint congruity and extensor mechanism biomechanics, ensuring optimal functional recovery.
COMPLICATIONS OF HAND FRACTURES: AN OVERVIEW
The human hand is an exquisitely balanced kinematic chain, relying on the precise interplay of osseous architecture, capsuloligamentous constraints, and a complex musculotendinous network. Consequently, fractures of the hand are highly susceptible to complications that can severely compromise both form and function. The most frequently encountered complications of hand fractures include malunion, nonunion, adhesion of tendons to the fracture site, deep space infection, and profound limitation of joint motion.
When managing the traumatized hand, particularly in the setting of crush injuries or high-energy trauma, the orthopedic surgeon is often faced with composite tissue loss. In these complex scenarios, a strict reconstructive hierarchy must be observed to optimize outcomes and prevent catastrophic failure of the surgical intervention.
The Reconstructive Hierarchy: Soft Tissue First
If multiple tissues must be reconstructed, the repair of bones and joints is strictly third in the order of priority. The foundational prerequisites for any successful osseous reconstruction are a robust soft tissue envelope and adequate neurovascular status.
Surgical Pearl: If good skin coverage is absent, osseous repair will inevitably fail due to desiccation, infection, or hardware exposure. Furthermore, if the hand is profoundly insensitive, structural repair is functionally futile, as the patient will bypass the insensate appendage and remain at high risk for recurrent, unrecognized microtrauma.
Bone and joint reconstruction procedures are indicated only after the following criteria are met:
1. Stable Soft Tissue Envelope: Good skin coverage has been obtained, either via primary closure, skin grafting, or local/free flap reconstruction.
2. Sensory Integrity: At least protective sensation is present, or nerve reconstruction has been performed and sensory return is forthcoming.
3. Vascular Patency: Adequate perfusion is confirmed to support fracture healing and combat potential infection.
PATHOPHYSIOLOGY AND BIOMECHANICS OF MALUNION
Malunion is one of the most functionally debilitating complications of hand fractures. If fractures of one or more bones of the hand unite in a poor anatomical position, the resulting deformity is rarely just a cosmetic issue; it fundamentally alters the biomechanics of the digit.
Disturbance of Muscle Balance
The hand relies on a delicate balance between the extrinsic flexors/extensors and the intrinsic musculature (lumbricals and interossei). Malunion disrupts this balance through several mechanisms:
* Rotational Deformity: Even a minor rotational malunion at the metacarpal or proximal phalanx level can lead to significant digital overlap (scissoring) during active flexion, severely impairing grip strength and dexterity.
* Angular Deformity: Volar angulation (apex dorsal) is common in metacarpal neck fractures. Excessive angulation alters the moment arm of the extensor mechanism, leading to a secondary extensor lag or compensatory hyperextension at adjacent joints (e.g., pseudoclawing).
* Shortening: Osseous shortening decreases the resting tension of the intrinsic and extrinsic tendons. A shortening of just 2 to 3 millimeters can result in a clinically noticeable extensor lag and a reduction in grip power due to the altered length-tension relationship of the muscle fibers.
Corrective osteotomy is often required to restore the anatomical axis, re-tension the musculotendinous units, and restore the normal cascade of the fingers.
THE BONY MALLET FINGER: INDICATIONS AND BIOMECHANICS
A classic example of a fracture requiring precise anatomical restoration to prevent debilitating malunion and joint dysfunction is the intra-articular mallet fracture. A mallet fracture occurs when an axial load is applied to an actively extended distal interphalangeal (DIP) joint, resulting in an avulsion of the terminal extensor tendon insertion along with a variable portion of the dorsal articular base of the distal phalanx.
Indications for Operative Intervention
While many soft-tissue mallet injuries and small avulsion fractures can be managed conservatively with strict extension splinting for 6 to 8 weeks, operative intervention is mandated in specific clinical scenarios to prevent secondary osteoarthritis, chronic extensor lag, and swan neck deformity.
Indications for Open Reduction and Internal Fixation (ORIF) include:
* Volar Subluxation: Any degree of volar subluxation of the distal phalanx relative to the middle phalanx indicates gross instability of the DIP joint.
* Articular Involvement: Fractures involving greater than 30% to 33% of the articular surface of the distal phalanx.
* Displacement: A fracture gap greater than 2 to 3 millimeters that cannot be reduced closed.
* Failure of Conservative Management: Inability to maintain reduction in a splint.
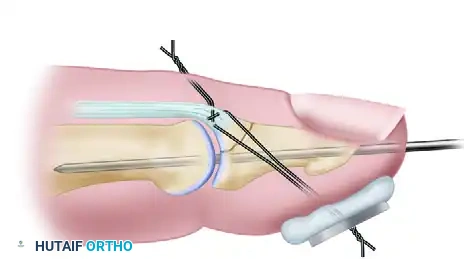
SURGICAL TECHNIQUE: REDUCTION AND FIXATION OF MALLET FRACTURES
The goal of surgical intervention is to anatomically reduce the articular surface, restore the continuity of the terminal extensor tendon, and stabilize the DIP joint to allow for early, protected healing. The following technique utilizes a transarticular Kirschner wire (K-wire) combined with a pull-out suture for fragment stabilization.
Step 1: Patient Positioning and Surgical Approach
The patient is positioned supine with the affected arm extended on a radiolucent hand table. A regional block (e.g., axillary or wrist block) or general anesthesia is administered. A well-padded forearm or arm tourniquet is applied to ensure a bloodless surgical field. Loupe magnification is highly recommended for precise handling of the delicate extensor mechanism and articular fragments.
The DIP joint is exposed through a dorsal zigzag incision or an H-shaped incision centered over the joint.
Surgical Warning: Extreme care must be taken during the dorsal approach to avoid injury to the germinal matrix of the nail bed, which lies immediately distal to the extensor insertion. The skin flaps should be elevated as full-thickness flaps to preserve the fragile dorsal vascularity and prevent marginal skin necrosis.
Step 2: Joint Preparation and Distal Phalanx Drilling
Once the joint is exposed, the fracture hematoma is meticulously irrigated and cleared. The dorsal avulsion fragment, which remains attached to the terminal extensor tendon, is gently retracted dorsally to inspect the articular surface of the middle and distal phalanges.
Before reducing the fracture, a smooth Kirschner wire (typically 0.035 or 0.045 inches) is prepared. The K-wire is drilled longitudinally through the distal phalanx, starting from the center of the articular surface of the distal phalanx and exiting through the distal tip of the finger (hyponychium).

- Technical Tip: Ensure the K-wire exits slightly volar to the nail plate to avoid iatrogenic nail deformity. The wire is driven distally until its proximal tip is flush with the articular surface of the distal phalanx, ensuring it does not impede the subsequent reduction of the joint.
Step 3: Anatomic Reduction and Transarticular Fixation
With the distal K-wire in place, the surgeon focuses on restoring the joint congruity.
* Reduce the joint: The distal phalanx is manipulated to correct any volar subluxation, aligning it perfectly with the condyles of the middle phalanx.
* Manipulate the fracture fragment: The dorsal avulsion fragment is gently hinged back into its anatomical bed on the distal phalanx.
* Pass the Kirschner wire across the joint: While holding the DIP joint in full, strict extension (0 degrees), the previously placed K-wire is driven proximally across the DIP joint into the middle phalanx. This transarticular wire neutralizes the deforming forces and holds the joint rigidly in extension.
Step 4: Fragment Fixation via Pull-Out Suture
In many cases, the dorsal fragment is too small or comminuted to accept direct screw or pin fixation without shattering. If the fracture fragment cannot be maintained in close, stable apposition to the major fragment by the transarticular wire alone, a pull-out suture technique is employed.
- A non-absorbable monofilament suture (e.g., 3-0 or 4-0 Prolene) is passed through the terminal extensor tendon just proximal to the bony fragment, utilizing a locking Krackow or Kessler-type stitch.
- The two ends of the suture are then passed through the fracture bed of the distal phalanx, exiting the volar aspect of the digital pulp. Straight Keith needles are highly effective for this trans-osseous passage.
- The fracture fragment is reduced anatomically into its bed.
- The suture ends are tied tightly over a padded button on the volar pulp of the finger.
Clinical Pitfall: The button must be adequately padded (often with a small piece of Xeroform or sterile felt) to prevent pressure necrosis of the volar skin. The tension on the suture should be sufficient to hold the fragment securely, but over-tensioning can cause ischemia of the pulp or fragmentation of the dorsal bone flake.
Step 5: Radiographic Verification and Closure
Before concluding the procedure, it is mandatory to obtain intraoperative fluoroscopic radiographs in at least two orthogonal planes (strict AP and true lateral).
* Verify the anatomical reduction of the articular surface.
* Confirm the correction of any volar subluxation.
* Ensure the transarticular K-wire is centrally placed within the medullary canal of the middle phalanx and does not penetrate the proximal interphalangeal (PIP) joint.
Once reduction and hardware placement are confirmed, the tourniquet is deflated, and meticulous hemostasis is achieved. The dorsal skin incision is closed with fine non-absorbable sutures (e.g., 5-0 or 6-0 nylon) using interrupted stitches to avoid strangulating the skin edges.
After closure, a sterile dressing is applied, and a custom thermoplastic or aluminum splint is fabricated to protect the transarticular Kirschner wire and the surgical repair.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
The success of mallet fracture fixation relies as much on disciplined postoperative care as it does on meticulous surgical technique. The rehabilitation protocol must balance the need for rigid immobilization to allow osseous union with the necessity of preventing profound joint stiffness.
Phase I: Immobilization (Weeks 0 to 6)
- Splinting: The DIP joint is maintained in continuous extension via the transarticular K-wire and the external splint. The PIP joint and metacarpophalangeal (MCP) joints are left free to prevent secondary stiffness of the digit.
- Wound Care: Sutures are typically removed at 10 to 14 days postoperatively. Pin site care is initiated to prevent superficial tract infections. The patient is instructed to keep the pin site clean and dry.
- Monitoring: The volar button (if a pull-out suture was used) must be inspected regularly to ensure there is no skin breakdown or necrosis.
Phase II: Hardware Removal and Early Motion (Week 6)
- Hardware Removal: At exactly 6 weeks postoperatively, clinical and radiographic assessments are performed. If radiographic union is evident, the transarticular Kirschner wire, the pull-out suture, and the volar button are removed in the clinic.
- Range-of-Motion Exercises: Active range-of-motion (AROM) exercises for the DIP joint are initiated immediately following pin removal.
- Night Splinting: A mallet splint is often continued at night for an additional 2 to 4 weeks to prevent stretching of the newly healed extensor mechanism and to combat any residual extensor lag.
Phase III: Strengthening and Return to Function (Weeks 8 to 12)
- Gentle passive range of motion (PROM) and progressive strengthening exercises are introduced.
- Patients are counseled that maximal medical improvement may take up to 6 months, and a mild residual extensor lag (5 to 10 degrees) or slight prominence of the dorsal joint is common but rarely limits functional capacity.
MANAGEMENT OF SURGICAL COMPLICATIONS
Despite meticulous technique, complications can arise during the management of mallet fractures.
- Pin Tract Infection: Superficial infections are common and usually resolve with oral antibiotics and local pin care. Deep infections may necessitate premature removal of the K-wire, which risks loss of reduction.
- Nail Deformity: Iatrogenic injury to the germinal matrix during the dorsal approach or improper K-wire placement can result in ridging or splitting of the nail plate. Prevention through careful anatomical dissection is paramount.
- Loss of Reduction: If the pull-out suture fails or the K-wire backs out prematurely, the fracture may displace. If recognized early, revision fixation may be required. If recognized late, it may result in a malunion requiring salvage procedures such as DIP joint arthrodesis.
- Skin Necrosis: Excessive tension on the volar button or aggressive retraction of the dorsal skin flaps can lead to full-thickness skin loss. This reinforces the principle of the reconstructive hierarchy: respecting the soft tissue envelope is the ultimate determinant of surgical success.
You Might Also Like
