Complications of Hand Fractures: Advanced Surgical Management
Key Takeaway
Complications of hand fractures, including malunion, nonunion, and joint contractures, require meticulous surgical management. Treatment prioritizes soft tissue coverage and sensation before bone reconstruction. Surgical interventions range from corrective osteotomies and corticocancellous grafting to precise capsulotomies. This guide details evidence-based indications, biomechanics, and step-by-step operative techniques to restore hand function, grip strength, and kinesthetic balance in complex cases.
COMPLICATIONS OF HAND FRACTURES
The management of hand fractures is fraught with potential pitfalls. Complications include malunion, nonunion, adhesion of tendons to the fracture site, deep space infection, and severe limitation of joint motion. When addressing a severely traumatized hand where multiple tissue types require reconstruction, the orthopaedic surgeon must adhere to a strict hierarchy of repair. The reconstruction of bones and joints is strictly third in the order of priority.
Surgical Pearl: The Hierarchy of Hand Reconstruction
If good, vascularized skin coverage is absent, underlying osseous repair will inevitably fail. Furthermore, if the hand is entirely insensitive, structural repair is functionally futile. Bone and joint reconstruction procedures are indicated only after stable soft-tissue coverage has been obtained and when at least protective sensation is present or definitively forthcoming via nerve repair.
MALUNION OF HAND FRACTURES
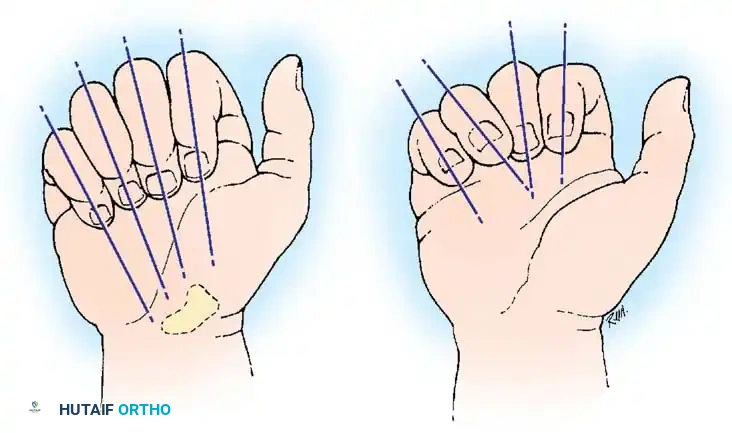
If fractures of one or more bones of the hand unite in an anatomically poor position, the resulting disturbance of the intrinsic and extrinsic muscle balance causes profound weakness of grasp and pinch. This is especially debilitating if the metacarpals and proximal phalanges are involved. The kinesthetic sense of the hand also becomes highly disturbed, leading to clumsy motor patterns.
Rotational malalignment and volar/dorsal angulation can cause notable hand deformity, which is usually accentuated when the patient attempts to make a composite fist. However, the fundamental rule of hand surgery applies: not every malunited fracture requires surgical intervention. The dynamic function of the fingers and the hand—not the static radiographic appearance—dictates the necessity of treatment. Ill-advised surgical intervention usually fails to improve function and frequently exacerbates stiffness.
Biomechanics and Tolerance of Angulation
Minor malunion deformities should generally be accepted when the motion of the surrounding joints is satisfactory. Treatment by corrective osteotomy can lead to nonunion, tendon adhesions, and severe difficulty in reestablishing satisfactory joint motion, particularly in patients beyond middle age.
Most malunited fractures of the metacarpal neck should be managed conservatively, particularly those involving the fifth metacarpal. Flexion deformities of 40 degrees or more in the fifth metacarpal neck can easily be accepted with excellent functional outcomes. When the fifth metacarpal head is displaced volarward, the highly mobile fifth carpometacarpal (CMC) joint allows dorsal displacement of the distal end of the bone, allowing the palm to yield dynamically when a hard object is grasped. This compensatory mechanism is also true, albeit to a lesser extent, for the ring finger.
Conversely, the second and third metacarpals have little to no motion at their respective CMC joints. When the metacarpal head of the index or long finger is displaced volarward, the rigid base forces the head into the palm, frequently causing pain with firm grasp.
When a metacarpal head is markedly displaced, secondary hyperextension of the metacarpophalangeal (MCP) joint and subsequent contracture of the collateral ligaments often occur. In these scenarios, a combined capsulotomy and corrective osteotomy may be necessary.
Management of Articular and Condylar Malunions
Certain malunions involving the articular surface require meticulous intra-articular osteotomies or grafting. When articular cartilage loss results in angular deformity, subluxation, dislocation, impending joint destruction, or intractable pain, osteoarticular grafts may be highly useful.
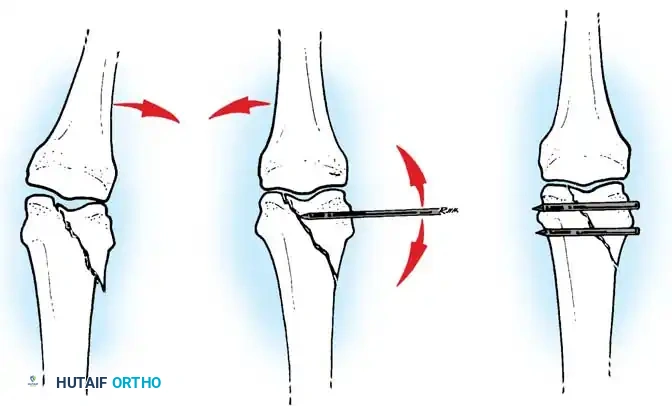
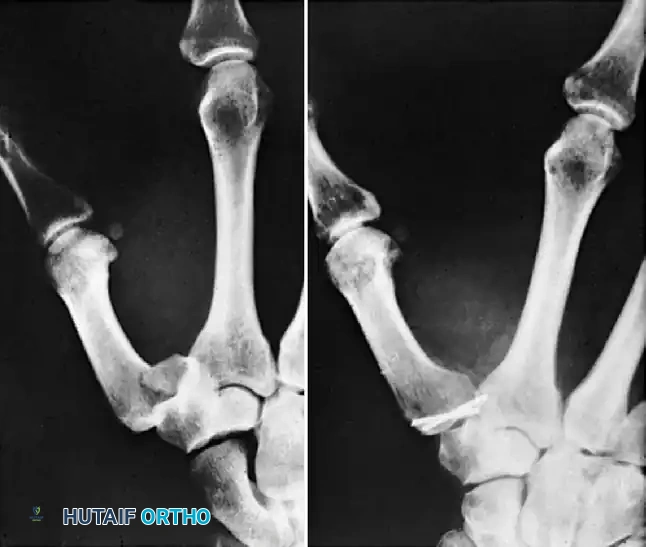
Fig. 64-68 A, Displaced, unstable condylar fracture usually requires open reduction and fixation. B, Manipulation of fracture using intact collateral ligament may permit insertion of Kirschner wire to hold reduction. C, Two wires may be necessary to avoid rotation of reduced fragment.

Fig. 64-67 A and B, Condylar fracture fixed with Kirschner wires.

Fig. 64-69 A, Malunited fracture of base of middle phalanx with splaying of volar and dorsal articular surfaces. B, After wedge resection of bone, volar and dorsal fragments were held securely with cerclage wire fixation.


Fig. 64-70 A and B, Destruction of middle phalanx ulnar base of golfer’s ring finger resulted in ulnar deviation and pain. C and D, Osteoarticular graft fashioned from ipsilateral distal radius resulted in satisfactory correction of deformity.
🔪 Surgical Technique 64-26: Correction of Malunion of the Metacarpal Neck
This technique utilizes a medullary cortical bone peg to provide intrinsic stability to the osteotomy site, minimizing the need for bulky hardware that could tether the extensor mechanism.
- Approach: Make a longitudinal dorsal incision just proximal and lateral to the metacarpal head. Carefully expose the extensor hood, preserving the paratenon, and free it on one side of the metacarpal neck with a sharp scalpel.
- Dissection: Dissect the interosseous muscle from the lateral side of the neck. Elevate the extensor tendon and expansion from its dorsum only as necessary for sufficient exposure to avoid devascularization.
- Osteotomy: If the fracture callus is hard and mature, drill across the old fracture site transversely with a fine K-wire to create stress risers; otherwise, cut across it cleanly with a sharp, thin osteotome.
- Medullary Preparation: Drill the medullary canal proximally and distally so that it accepts a medullary cortical bone peg slightly larger than a matchstick.
- Graft Harvest: Obtain the cortical peg from the proximal ulna or proximal medial tibia.
- Insertion: Insert the peg proximally into the medullary canal of the shaft; cap it with the metacarpal head fragment.
- Alignment: Carefully check rotational alignment by passively flexing the wrist and observing the cascade of the fingers. Impact the fragments gently.
- Augmentation: Pack cancellous bone chips around the osteotomy juncture as needed. If the osteotomy remains rotationally unstable despite the bone peg, insert a single oblique Kirschner wire across the osteotomy site.
- Joint Assessment: Examine the MCP joint for passive flexion. If the collateral ligaments are contracted and allow little or no motion, a formal capsulotomy is indicated.
- Closure: Suture the lateral expansion of the extensor hood in place with fine absorbable suture (e.g., 4-0 Vicryl).
- Immobilization: Hold the MCP joint in 60 to 70 degrees of flexion, and apply a protective volar splint.

Fig. 64-71 Malunited fracture of fifth metacarpal neck treated by open reduction and fixation with one Kirschner wire inserted obliquely. This rarely is necessary because normal motion of fifth carpometacarpal joint permits tolerance of 40 degrees of angulation at fracture site.
Postoperative Protocol:
A dorsal blocking splint is worn for 2 weeks to maintain the MCP joints in 70 degrees of flexion, which keeps the collateral ligaments at their maximal length, while allowing active flexion of the interphalangeal (IP) joints. Sutures are removed at 2 weeks, and a lighter splint is applied that prevents extension of the MCP joint but allows full flexion and extension of the IP joints. This splint is worn for an additional 1 to 2 weeks depending on radiographic consolidation.
Phalangeal Malunion Correction
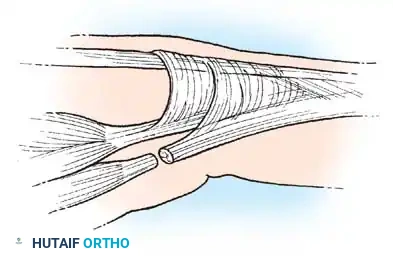
Malunion of a metacarpal shaft or of a phalanx can also be treated with a medullary cortical bone peg; however, the peg must be shaped meticulously to fit snugly without causing iatrogenic comminution.

Fig. 64-72 Malunion of a metacarpal shaft treated with a medullary cortical bone peg.
Malrotation of a proximal phalanx at any level should ideally be treated by a corrective osteotomy at the base of the phalanx whenever possible, rather than at the diaphyseal malunion site. The metaphyseal base of the phalanx heals rapidly due to its rich cancellous bone stock and is cut with far less difficulty than the hard, sclerotic cortical bone in the middle third.
Surgical Warning: Rotational Correction
It is critical to make a longitudinal orientation mark (using a sterile marker or a shallow saw score) on each side of the proposed osteotomy line before the cut is made. These reference points are essential to determine the exact degree of rotational correction achieved during the procedure.

Fig. 64-74 A, Malunited phalangeal fracture with rotational deformity. B, After treatment by osteotomy through proximal end of bone and fixation with two Kirschner wires. Healing usually is more rapid after osteotomy at this level than after one at old fracture.
NONUNION OF HAND FRACTURES
Nonunion in the phalanges is most frequently caused by distraction of the fragments (often from excessive traction during conservative management), deep infection, lack of rigid fixation resulting in micromotion, and gaps between bone ends resulting from traumatic bone loss.
If the nonunion is associated with severe nerve and tendon injuries that permanently impair function, ray amputation must be strongly considered, especially if only a single finger is involved. A stiff, insensate, non-united digit will only serve to impede the function of the adjacent normal fingers.
Distal Phalanx Nonunion
Nonunions of comminuted fractures of the tuft of the distal phalanx usually require no treatment; the fragments commonly unite via fibrous tissue or are eventually resorbed without clinical consequence. However, nonunions of transverse fractures of the distal phalanx diaphysis may require surgical treatment (e.g., K-wire fixation and bone grafting) if they remain persistently painful.
Clinical Evaluation: Differentiating Nonunion Pain from Neuroma
The differentiation between pain originating from a mobile nonunion and pain from scar tissue tethering nerve endings (neuroma) is critical. Applying lateral bending stress to the nonunion site should elicit deep bone pain if the nonunion is symptomatic. Conversely, simple axial tapping of the finger tuft, which stimulates tightly bound nerve endings, will cause sharp, radiating pain characteristic of a neuroma.
Metacarpal Nonunion
Nonunion in the metacarpals is produced most often by high-energy bone loss (e.g., gunshot wounds, industrial crush injuries). For a nonunion in which no bone substance is lost, the technique of repair is identical to that described for malunion (compression plating or medullary peg).
For a nonunion in which bone substance is lost, an interpositional corticocancellous bone graft combined with rigid dorsal plating is the modern gold standard. As an alternative in cases where plating is not feasible due to soft tissue constraints, Littler’s method can be used, provided that bony stability is achieved with the corticocancellous graft alone.
Fig. 64-75 A, Metacarpal nonunion in which bone substance has been lost. B, After grafting by Littler technique.
🔪 Surgical Technique 64-27: Correction of Nonunion of the Metacarpals (Littler Technique)
The success of bone grafting metacarpal defects depends heavily on soft-tissue and bony factors. First, the dorsum of the hand must be well covered by healthy, vascularized skin and subcutaneous tissue. If necessary, local rotational flaps or remote flaps (such as a groin or abdominal pedicle flap) must be performed prior to bone grafting. Second, the fine details of what Bunnell called “bone carpentry” must be exact to ensure osteoconduction and stability.
- Preparation: Administration of prophylactic intravenous antibiotics just before tourniquet inflation is mandatory. Postoperative antibiotics should be considered because the injury producing the bone defect was inherently open and potentially colonized.
- Exposure: Expose the defective metacarpal with a longitudinal or gently curved dorsal incision, avoiding previous compromised scars.
- Soft Tissue Dissection: Dissect all scar tissue from the extensor tendons meticulously, preserving the paratenon intact to prevent postoperative tendon tethering.
- Debridement: Dissect the fibrous nonunion tissue en bloc from between the fragments. Apply longitudinal traction to the digit to restore normal finger length and assess the true size of the bony defect.
- Proximal Preparation: Usually, the sclerotic proximal fragment must be sacrificed as far as its metaphyseal base. Resect it with a sharp osteotome at an angle of 30 degrees, creating a receiving recess in the bone.
- Distal Preparation: Cut the end of the distal fragment transversely with an oscillating saw or rongeur, and open the medullary canal with a burr to receive the doweled end of the graft.
- Graft Harvest: With traction maintained on the finger, measure the exact defect between the fragments. Harvest a corticocancellous graft from the proximal tibia at least 1.3 cm longer than the measured defect.
- Graft Shaping: Fashion a cylindrical dowel at one end of the graft, and cut the other end obliquely at exactly 30 degrees.
- Insertion: Insert the doweled end into the medullary canal of the distal fragment, and press the 30-degree proximal end into the prepared metacarpal or carpal recess. The natural resting tension of the soft tissues will compress the graft between the two fragments, holding it securely in place.
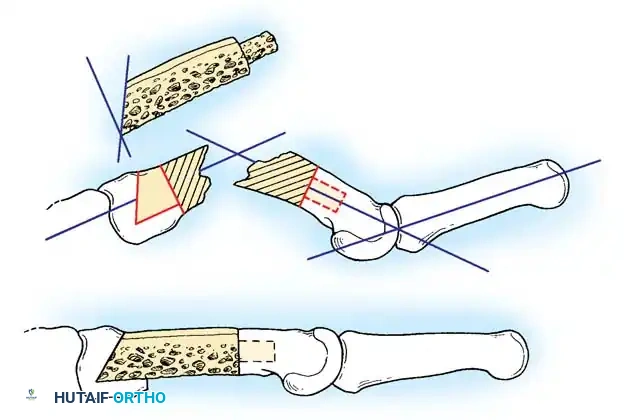
Fig. 64-76 Littler technique for grafting metacarpal nonunion in which bone substance has been lost. Note the 30-degree proximal cut.
- Fixation: If the construct feels unstable, stabilize the graft by passing one or more transverse Kirschner wires through it and into the adjacent, uninvolved metacarpals.
- Closure: Close the periosteal sheath (if present) and the soft tissues over the graft with fine absorbable sutures.
Postoperative Protocol:
With the hand in the intrinsic-plus position of function, a bulky plaster cast or splint is applied that extends to the PIP joints. This cast must be immediately split to accommodate postoperative swelling. On about the 12th day, a new, well-molded cast is applied that immobilizes only the grafted metacarpal and the proximal phalanx; it is left in place for a minimum of 2 months until radiographic union is confirmed.
JOINT CONTRACTURES AND CAPSULOTOMY
Prolonged immobilization of hand fractures frequently leads to severe joint contractures. If joint motion is limited primarily because of secondary contracture of the collateral ligaments, a surgical capsulotomy may be indicated.
Metacarpophalangeal Joint Capsulotomy
The MCP joints are particularly prone to extension contractures if immobilized improperly. The collateral ligaments of the MCP joint are eccentric; they are lax in extension and taut in flexion. Immobilization in extension allows these ligaments to shorten, permanently preventing subsequent flexion.
Surgical Warning: Contraindications for Capsulotomy
When active or passive motion in the MCP joint is already 60 degrees or greater, capsulotomy is strictly contraindicated. Even with perfect surgical technique and normal surrounding soft tissues, only 60 to 70 degrees of motion can typically be expected postoperatively. Operating on a joint with 60 degrees of motion risks making the patient worse.
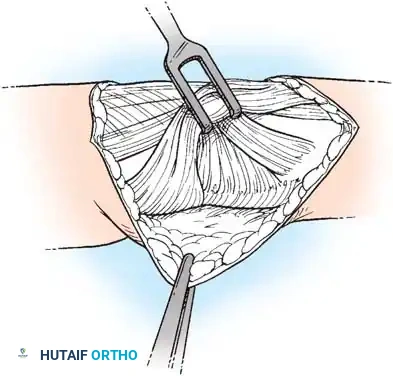
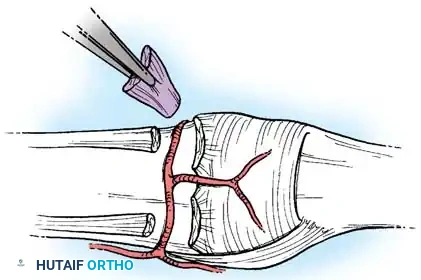
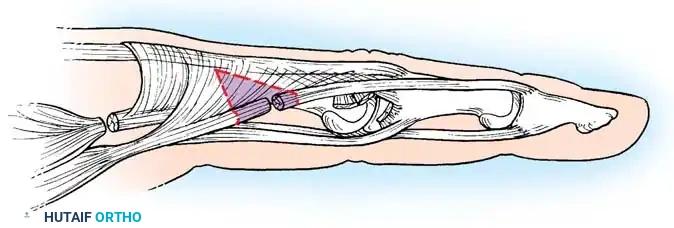
Exposure of the extensor mechanism during dorsal approach to the MCP joint.
🔪 Surgical Technique 64-28: MCP Joint Capsulotomy
- Incision: Make a longitudinal incision 2.5 cm long over the affected joint. If two adjacent joints are affected, make a single incision in the web space between the MCP joints. Second and fourth web space dorsal longitudinal incisions can be used to release all four MCP joints if necessary.
- Extensor Hood Release: At a point 0.5 cm from the central slip of the extensor tendon, incise the extensor hood on both the dorsolateral and dorsomedial aspects of the joint.
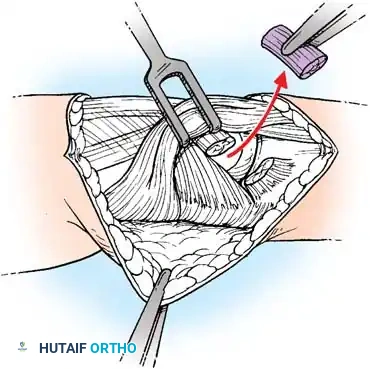
Incision of the extensor hood to expose the underlying capsule.
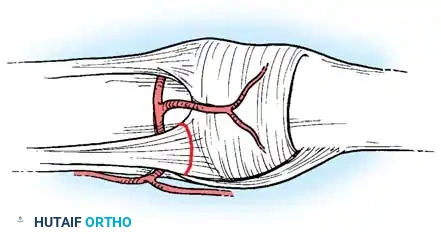
- Exposure: Retract the anterior part of the extensor hood and the intrinsic tendons laterally, exposing the underlying thick collateral ligaments and dorsal capsule.
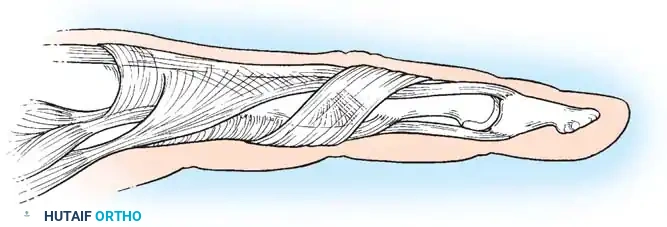
Anatomy of the dorsal joint capsule and collateral ligaments.
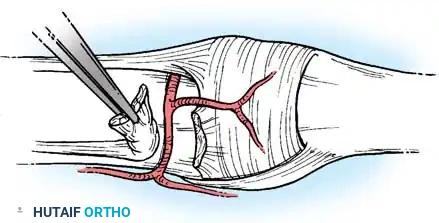
- Capsulectomy: Transect and remove the dorsal joint capsule entirely. Excise portions of the contracted collateral ligaments from each side of the joint to permit volar translation and flexion.
Excision of the contracted collateral ligament to restore flexion.
- Mobilization: Flex the joint passively. Keep the joint surfaces in full contact, and verify that the base of the proximal phalanx remains concentrically seated on the metacarpal head during flexion and glides smoothly without hinging.
- Volar Plate Release: Sometimes the volar pouch is obliterated by scar tissue. During attempted passive flexion, the posterior joint may hinge open due to impingement of the volar proximal phalanx lip. If the volar plate is adherent, carefully strip it from the anterior aspect of the metacarpal head using a blunt probe or Freer elevator.
- Stability Check: Release additional capsule and collateral ligament attachments only as needed to gain full passive flexion. Do not destabilize the joint, especially the radial collateral ligament of the index finger, which is critical for pinch strength.
- Closure: When satisfactory passive
Associated Surgical & Radiographic Imaging
You Might Also Like