Closed Pinning Techniques for Hand Fractures

Key Takeaway
Closed pinning utilizing Kirschner wires remains a cornerstone in the management of unstable metacarpal and phalangeal fractures. This minimally invasive technique, particularly the Wagner method for Bennett fractures, provides crucial skeletal stability while preserving the soft tissue envelope. Success relies on precise anatomical reduction, understanding deforming muscular forces, and strategic pin placement to maintain articular congruity and rotational alignment during osseous union.
Introduction to Closed Pinning in Hand Trauma
The management of hand fractures requires a delicate balance between achieving rigid skeletal stability and preserving the intricate gliding mechanisms of the surrounding soft tissues. Closed pinning, utilizing Kirschner wires (K-wires), remains one of the most versatile, effective, and frequently employed techniques in operative orthopaedics. By avoiding extensive surgical dissection, closed pinning minimizes the risk of iatrogenic soft tissue scarring, tendon adhesions, and devascularization of fracture fragments.
This comprehensive guide details the advanced principles of closed pinning, with a specific focus on the Wagner technique for first carpometacarpal (CMC) joint fracture-dislocations (Bennett fractures), extra-articular metacarpal base fractures, and complex phalangeal reconstructions.
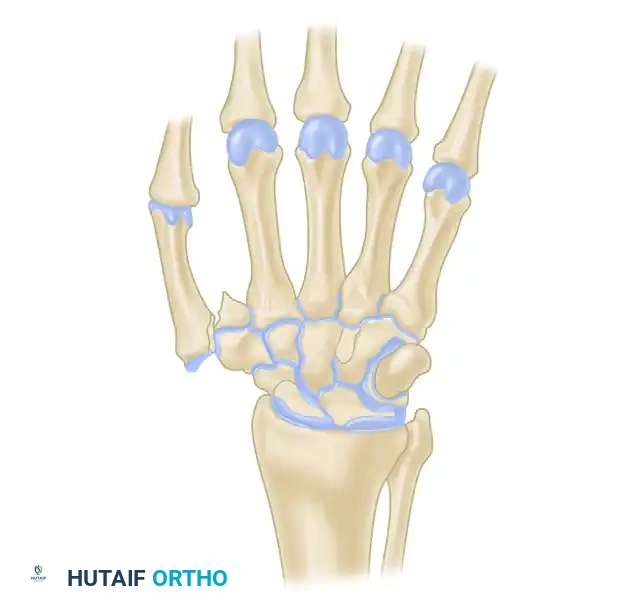
Biomechanics and Pathoanatomy of Deforming Forces
To successfully execute a closed pinning procedure, the surgeon must possess a profound understanding of the intrinsic and extrinsic deforming forces acting upon the hand skeleton.
The Bennett Fracture-Dislocation
A Bennett fracture is an intra-articular fracture-dislocation of the base of the first metacarpal. The biomechanical hallmark of this injury is the divergent pull of the surrounding musculature:
1. The Volar Ulnar Fragment: This small articular fragment remains anatomically secured to the trapezium by the robust anterior oblique ligament (AOL). It does not displace.
2. The Metacarpal Shaft: The primary deforming forces act upon the shaft. The abductor pollicis longus (APL) pulls the shaft proximally, dorsally, and radially. Simultaneously, the adductor pollicis pulls the distal metacarpal head into adduction, exacerbating the apex-dorsal and radial angulation.
Clinical Pearl: In a Bennett fracture, the first metacarpal shaft is displaced by the divergent pull of muscles. The goal of closed reduction is not to reduce the small volar fragment to the shaft, but rather to reduce the displaced metacarpal shaft back to the anatomically anchored volar ulnar fragment.
The Wagner Technique for Closed Pinning
The Wagner technique is the gold standard for the closed management of Bennett fractures. It relies on reversing the deforming forces through specific manual maneuvers, followed by percutaneous transarticular fixation.
Step 1: Patient Positioning and Setup
The procedure is performed under regional anesthesia (supraclavicular or axillary block) or general anesthesia. The patient is positioned supine with the arm extended on a radiolucent hand table. A mini C-arm fluoroscopy unit is brought in perpendicular to the hand to allow for real-time orthogonal imaging (posteroanterior, lateral, and Robert's views).
Step 2: The Closed Reduction Maneuver
Maintaining fracture reduction requires a precise sequence of manual traction and pressure:
* Longitudinal Traction: Apply firm axial traction to the thumb to overcome the proximal pull of the APL.
* Palmar Abduction and Pronation: Bring the thumb into palmar abduction and pronation to tension the volar ligaments and align the articular surface.
* Direct Pressure: Apply direct, firm pressure over the dorsal-radial aspect of the first metacarpal base to push the shaft back into the CMC joint and align it with the volar ulnar fragment.
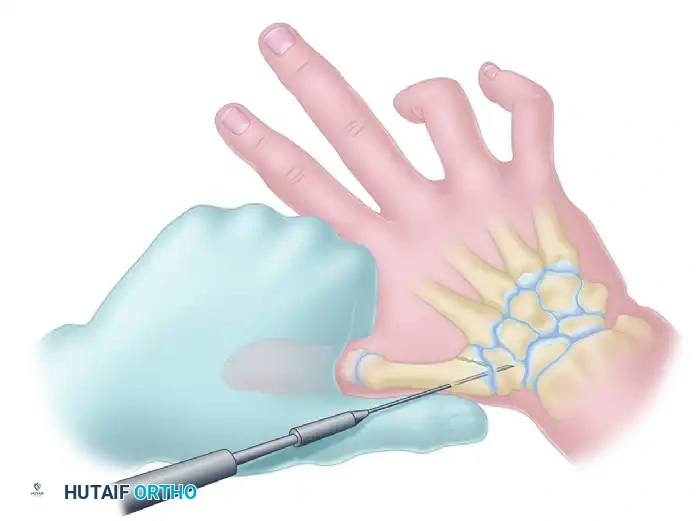
Step 3: Percutaneous Pin Placement
While an assistant (or the surgeon's non-dominant hand) maintains the reduction, the pinning is executed:
* Drill a 0.045-inch or 0.062-inch Kirschner wire into the base of the metacarpal.
* Direct the wire proximally across the CMC joint and into the body of the trapezium.
Surgical Warning: Fixation merely to the volar oblique fragment is often insufficient to prevent the loss of fracture reduction. The K-wire must engage the trapezium to neutralize the deforming forces of the APL.
Sometimes, more than one Kirschner wire is required to achieve absolute rotational stability. Depending on the fracture geometry, the secondary wire may engage carpal bones other than the trapezium (such as the trapezoid or the capitate) for adequate fixation.
Step 4: Fluoroscopic Verification and Pin Management
- Check the reduction meticulously using multi-planar fluoroscopy. Ensure there is no articular step-off greater than 1 mm.
- If the reduction is accurate and stable, cut the K-wire near the skin. Bending the wire outside the skin facilitates easy removal in the clinic but requires meticulous pin-site care to prevent infection. Alternatively, wires can be buried beneath the skin, though this necessitates a minor secondary procedure for removal.
Management of Extra-Articular Thumb Base Fractures
Extra-articular fractures of the first metacarpal base (epibasal fractures) are common and often present with significant apex-dorsal angulation due to the unopposed pull of the APL.
Consider the case of an extra-articular thumb base fracture with 35 degrees of apex dorsal angulation in a 65-year-old male. While up to 30 degrees of angulation can sometimes be tolerated due to the compensatory mobility of the CMC joint, greater angulation requires reduction to prevent symptomatic hyperextension of the metacarpophalangeal (MCP) joint.
Surgical Steps for Epibasal Fractures:
1. Perform closed reduction using longitudinal traction and direct volar-directed pressure over the fracture apex.
2. Secure the reduction with K-wire fixation driven from the metacarpal shaft into the trapezium, bypassing the fracture site to provide a stable strut.
The following sequence illustrates the progression from injury to successful closed reduction and K-wire fixation into the trapezium:






Metacarpal Shaft and Phalangeal Fractures
While closed pinning is highly effective for thumb base injuries, it is equally critical in the management of metacarpal shaft and phalangeal fractures, particularly in the setting of severe trauma or multiple-digit replantation.
Oblique and Spiral Metacarpal Fractures
Oblique fractures of the metacarpal shaft often result in shortening and malrotation. While closed pinning (transverse or intramedullary) is an option, the lag screw technique provides superior interfragmentary compression for long oblique fractures where the fracture length is at least twice the diameter of the bone.

Alternative pinning configurations for metacarpal shaft fractures:


Complex Phalangeal Trauma and Replantation
In cases of severe open fractures with bone loss, structural grafting and complex pinning techniques are required. For example, in open fractures of the right hand with loss of the distal end of the middle phalanx and a painful small finger partial amputation, the proximal phalanx of the stiff small finger can be utilized as a structural graft to restore the articular column of the middle finger.



Various techniques are employed to manage middle phalangeal fractures in multiple-digit replantation. A combination of intramedullary Kirschner wire rods and wiring in the index finger, alongside intraosseous wiring alone in the middle finger, can provide excellent rotational control and stability necessary for early rehabilitation.
Management of Delayed Presentations
Closed pinning is highly time-sensitive. Fractures presenting late (beyond 2-3 weeks) often exhibit early callus formation and cannot be reduced closed.
Consider a young man presenting with a 6-week-old Bennett fracture and an accompanying dorsal trapezial rim fracture. At this stage, the deforming forces have led to fixed malunion.
Surgical Approach for Delayed Union:
1. An open approach (Wagner or radiopalmar incision) is mandatory.
2. The CMC joint is exposed, and the organizing fracture callus is meticulously excised.
3. The fracture fragments are mobilized and anatomically reduced under direct vision.
4. Fixation is then achieved using the same pinning principles, driving K-wires across the joint to secure the reduction.
The following images detail the complex reconstruction, callus excision, and subsequent K-wire fixation required for delayed Bennett fracture presentations:




Postoperative Protocol and Rehabilitation
The success of closed pinning is heavily dependent on rigorous postoperative care and immobilization to protect the K-wires from cyclical loading and failure.
Immobilization Strategy
Immediately following the procedure, apply a well-padded forearm cast or a rigid thermoplastic splint.
* Wrist Position: Hold the wrist in approximately 20 to 30 degrees of extension.
* Thumb Position: Hold the thumb in palmar abduction to maintain the first web space and neutralize the adductor pollicis.
* IP Joint: Crucially, leave the thumb interphalangeal (IP) joint free to allow for early active range of motion, which prevents extensor tendon adhesions and promotes tendon gliding.
Pin Removal and Therapy
- Timeline: K-wires are typically left in place for 4 to 6 weeks, depending on radiographic evidence of clinical union and the patient's age.
- Pin Care: If pins are left proud, patients must be instructed on daily pin-site care using chlorhexidine or saline to prevent superficial tract infections.
- Rehabilitation: Once the pins are removed, the patient is transitioned to a removable splint. Hand therapy is initiated immediately, focusing on active and active-assisted range of motion of the CMC, MCP, and IP joints. Strengthening exercises are generally delayed until 8 weeks post-injury.
Pitfall: Premature pin removal before adequate osseous union can lead to catastrophic loss of reduction, especially in Bennett fractures where the APL exerts continuous proximal force. Always confirm bridging callus on multiple radiographic views prior to extracting transarticular wires.
Conclusion
Closed pinning remains an indispensable technique in the orthopaedic surgeon's armamentarium for managing hand trauma. Whether executing the Wagner technique for a Bennett fracture or stabilizing a complex phalangeal injury during replantation, strict adherence to biomechanical principles, precise fluoroscopic guidance, and meticulous postoperative care are paramount. By respecting the soft tissue envelope and achieving rigid skeletal stability, surgeons can ensure optimal functional outcomes and restore the intricate mechanics of the human hand.
📚 Medical References
- closed pinning, Clin Orthop Relat Res 219:174, 1987.
- Ay S, Akinci M, Kamiloglu S, et al: Open reduction of displaced pediatric supracondylar humeral fractures through the anterior cubital approach, J Pediatr Orthop 25:149, 2005.
- Barrett WP, Almquist EA, Staheli LT: Fracture separation of the distal humeral epiphysis in the newborn, J Pediatr Orthop 4:617, 1984.
- Battaglia TC, Armstrong DG, Schwend RM: Factors affecting forearm compartment pressures in children with supracondylar fractures of the humerus, J Pediatr Orthop 22:431, 2002.
- Beals RK: The normal carrying angle of the elbow, Clin Orthop Relat Res 119:194, 1976.
- Bellemore MC, Barrett IR, Middleton RWD: Supracondylar osteotomy of the humerus with correction of cubitus varus, J Bone Joint Surg 66B:566, 1984.
- Biyani A, Gupta SP, Sharma JC: Determination of medial epicondylar epiphyseal angle for supracondylar humeral fractures in children, J Pediatr Orthop 13:94, 1993.
- Blount WP: Fractures in children, Instr Course Lect 7:194, 1950.
- Bosanquet JS, Middleton RW: The reduction of supracondylar fractures of the humerus in children treated by traction-inextension, Injury 14:373, 1983.
- Boyd DW, Aronson DD: Supracondylar fractures of the humerus: a prospective study of percutaneous pinning, J Pediatr Orthop 12:789, 1992.
- Brown IC, Zinar DM: Traumatic and iatrogenic neurological complications after supracondylar humerus fractures in children, J Pediatr Orthop 15:440, 1995.
- Butcher CC, Hoffman EB: Supracondylar fractures of the femur in children: closed reduction and percutaneous pinning of displaced fractures, J Pediatr Orthop 25:145, 2005.
- Canale ST, Beaty JH, Warner WC, et al: Passive fl exion sign: a simple tool for diagnosis of anterior interosseous nerve injury in children, J Bone Joint Surg 82A:1354, 2000.
- Casiano E: Reduction and fi xation by pinning “banderillero,” Mil Med 125:262, 1961.
- Celiker O, Pestilci FI, Tuzuner M: Supracondylar fractures of the humerus in children: analysis of the results in 142 patients, J Orthop Trauma 4:265, 1990.
- Chen RS, Liu CB, Lin XS, et al: Supracondylar extension fracture of the humerus in children, J Bone Joint Surg 83B:883, 2001.
- Clement DA, Phil D: Assessment of a treatment plan for managing acute vascular complications associated with supracondylar fractures of the humerus in children, J Pediatr Orthop 10:97, 1990.
- Culp RW, Osterman AL, Davidson RS, et al: Neural injuries associated with supracondylar fractures of the humerus in children, J Bone Joint Surg 72A:1211, 1990.
- Dameron TB: Transverse fractures of the distal humerus in children, Instr Course Lect 30:224, 1981.
- Danielsson L, Pettersson H: Open reduction and pin fi xation of severely displaced supracondylar fractures of the humerus in children, Acta Orthop Scand 51:249, 1980.
- Davids JR, Maguire MF, Mubarak SJ, et al: Lateral condylar fracture of the humerus following post-traumatic cubitus varus, J Pediatr Orthop 14:466, 1994.
- De Boeck H, De Smet P, Peners W, et al: Supracondylar elbow fractures with impaction of the medial condyle in children, J Pediatr Orthop 15:444, 1995.
- DeLee JC, Wilkins KE, Rogers LF, et al: Fracture-separation of the distal humerus epiphysis, J Bone Joint Surg 62A:46, 1980.
- DeRosa GP, Graziano GP: A new osteotomy for cubitus varus, Clin Orthop Relat Res 236:160, 1988.
- Dodge HS: Displaced supracondylar fractures of the humerus in children: treatment by Dunlop’s traction, J Bone Joint Surg 54A:1408, 1972.
- Eaton RG, Green WT: Epimysiotomy and fasciotomy in the treatment of Volkmann’s ischemic contracture, Orthop Clin North Am 3:175, 1972.
- Flynn JC, Matthews JG, Benoit RL: Blind pinning of displaced supracondylar fractures of the humerus in children, J Bone Joint Surg 56A:263, 1974.
- Foster BK, Paterson DC: Diffi cult supracondylar elbow fractures in children: analysis of percutaneous pinning technique, J Pediatr Orthop 12:11, 1991.
- Fowles JV, Kassab MT: Displaced supracondylar fractures of the elbow in children, J Bone Joint Surg 56B:490, 1974.
- French PR: Varus deformity of elbow following supracondylar fractures of the humerus in children, Lancet 2:439, 1959.
- Fuller DJ, McCullough CJ: Malunited fractures of the forearm in children, J Bone Joint Surg 64B:364, 1982.
- Gadgil A, Hayhurst C, Maffulli N, et al: Elevated, straight-arm traction for supracondylar fractures of the humerus in children, J Bone Joint Surg 87B:82, 2005.
- Garbuz DS, Leitch K, Wright JG: The treatment of supracondylar fractures in children with an absent radial pulse, J Pediatr Orthop 16:594, 1996.
- Gartland JJ: Management of supracondylar fractures of the humerus in children, Surg Gynecol Obstet 109:145, 1959.
- Gelberman RH, Garfi n SR, Hergenroeder PT, et al: Compartment syndromes of the forearm: diagnosis and treatment, Clin Orthop Relat Res 161:252, 1981.
- Gordon JE, Patton CM, Luhmann SJ, et al: Fracture stability after pinning of displaced supracondylar distal humerus fractures in children, J Pediatr Orthop 21:313, 2001.
- Gosens T, Bongers KJ: Neurovascular complications and functional outcome in displaced supracondylar fractures of the humerus in children, Injury 34:267, 2003.
- Graham B, Tredwell SJ, Beauchamp RD, et al: Supracondylar osteotomy of the humerus for correction of cubitus varus, J Pediatr Orthop 10:228, 1990.
- Graves SC, Beaty JH: Supracondylar fractures of the humerus in children: treatment by closed reduction and pinning, Orthop Trans 13:540, 1989.
- Green NE: Overnight dealay in the reduction of supracondylar fractures of the humerus in children, J Bone Joint Surg 83A:321, 2001.
- Gruber MA, Hudson OC: Supracondylar fractures of the humerus in childhood, J Bone Joint Surg 46A:1245, 1964.
- Gupta N, Kay RM, Leitch K, et al: Effect of surgical delay on perioperative complications and need for open reduction in supracondylar humerus fractures in children, J Pediatr Orthop 24:245, 2004.
- Haddad RJ, Saer JK, Riordan DC: Percutaneous pinning of displaced supracondylar fractures of the elbow in children, Clin Orthop Relat Res 71:112, 1970.
- Hadlow AT, Devane P, Nicol RO: A selective treatment approach to supracondylar fracture of the humerus in children, J Pediatr Orthop 16:104, 1996.
- Hansen PE, Barnes DA, Tullos HS: Arthroscopic diagnosis of an injury pattern in the distal humerus of an infant, J Pediatr Orthop 2:569, 1982.
- Herzenberg JE, Korseka J, Carroll NC, et al: Biomechanical testing of pin fi xation techniques for pediatric supracondylar elbow fractures, Orthop Trans 12:678, 1988.
- Holda ME, Manoli A, LaMont RL: Epiphyseal separation of the distal end of the humerus with medial displacement, J Bone Joint Surg 62A:52, 1980.
- Hui JP, Torode IP, Chatterjee A: Medial approach for corrective osteotomy of cubitus varus: a cosmetic incision, J Pediatr Orthop 24:477, 2004.
- Ippolito E, Caterini R, Scola E: Supracondylar fractures of the humerus in children: analysis at maturity of fi fty-three patients treated conservatively, J Bone Joint Surg 68A:333, 1986.
- Kaewpornsawan K: Comparison between closed reduction with percutaneous pinning and open reduction with pinning in children with closed totally displaced supracondylar humeral fractures: a randomized controlled trial, J Pediatr Orthop 10B:131, 2001.
- Kasser JR: Percutaneous pinning of supracondylar fractures of the humerus in children, Instr Course Lect 41:385, 1992.
- Kekomäki M, Luoma RR, Rikalainen H, et al: Operative reduction and fi xation of diffi cult supracondylar extension fracture, J Pediatr Orthop 4:13, 1984.
- Keppler P, Salem K, Schwarting B, et al: The effectiveness of physiotherapy after operative treatment of supracondylar humeral fractures in children, J Pediatr Orthop 25:314, 2005.
- Kim HT, Lee JS, Yoo CI: Management of cubitus varus and valgus, J Bone Joint Surg 87A:771, 2005.
- Kim WY, Chandru R, Bonshahi A, et al: Displaced supracondylar humeral fractures in children: results of a national survey of paediatric orthopaedic consultants, Injury 34:274, 2003.
- King D, Secor C: Bow elbow (cubitus varus), J Bone Joint Surg 33A:572, 1951.
- Kiyoshige Y: Critical displacement of neural injuries in supracondylar humeral fractures in children, J Pediatr Orthop 19:816, 1999.
- Kramhøft M, Keller IL, Solgaard S: Displaced supracondylar fractures of the humerus in children, Clin Orthop Relat Res 221:215, 1987.
- Kumar R, Kiran K, Malhotra R, et al: Surgical management of the severely displaced supracondylar fracture of the humerus in children, Injury 33:517, 2002.
- Kurer MHJ, Regan MW: Completely displaced supracondylar fracture of the humerus in children: a review of 1708 comparable cases, Clin Orthop Relat Res 256:205, 1990.
- Labelle H, Bunnell WP, Duhaime M, et al: Cubitus varus deformity following supracondylar fractures of the humerus in children, J Pediatr Orthop 2:539, 1982.
- Leet AI, Frisancho J, Ebramzadeh E: Delayed treatment of type 3 supracondylar humerus fractures in children, J Pediatr Orthop 22:203, 2002.
- Lucas JC, Mehlman CT, Laor T: The location of the biceps tendon in completely displaced proximal humerus fractures in children: a report of four cases with magnetic resonance imaging and cadaver correlation, J Pediatr Orthop 24:249, 2004.
- Lyons JP, Ashley E, Hoffter MM: Ulnar nerve palsies after percutaneous cross-pinning of supracondylar fractures in children’s elbows, J Pediatr Orthop 18:43, 1998.
- Mapes RC, Hennrikus WL: The effect of elbow position on the radial pulse measured by Doppler ultrasonography after surgical treatment of supracondylar elbow fractures in children, J Pediatr Orthop 18:441, 1998.
- Marion J, LaGrange J, Faysse R, et al: Les fractures d l’extremite inferieure de l’humerus chez l’enfant, Rev Chir Orthop 48:337, 1962.
- Matsuzaki K, Nakatani N, Harada M, et al: Treatment of supracondylar fracture of the humerus in children by skeletal traction in a brace, J Bone Joint Surg 86B:232, 2004.
- Mazda K, Boggione C, Fitoussi F, et al: Systematic pinning of displaced extension-type supracondylar fractures of the humerus in children, J Bone Joint Surg 83B:888, 2000.
- Mehlman CT, Strub WM, Roy DR, et al: The effect of surgical timing on the perioperative complications of treatment of supracondylar humeral fractures in children, J Bone Joint Surg 83A:323, 2001.
- Mehserle WL, Meehan PL: Treatment of the displaced supracondylar fracture of the humerus (type III) with closed reduction and percutaneous cross-pin fi xation, J Pediatr Orthop 11:705, 1991.
- Merchan ECR: Supracondylar fractures of the humerus in children: treatment by overhead skeletal traction, Orthop Rev 21:475, 1992.
- Mizuno K, Hirohata K, Kashiwagi D: Fracture-separation of the distal humeral epiphysis in young children, J Bone Joint Surg 61A:570, 1979.
- Mohammad S, Rymaxzewski LA, Runciman J: The Baumann angle in supracondylar fractures of the distal humerus in children, J Pediatr Orthop 19:65, 1999.
- O’Brien WR, Eilert RE, Chang FM, Glavey GL: The metaphyseal-diaphyseal angle as a guide to treating supracondylar fractures of the humerus in children. Paper presented at the fi fty-fourth annual meeting of the American Academy of Orthopaedic Surgeons, San Francisco, Jan. 1987.
- Oh CW, Park BC, Ihn JC, et al: Fracture separation of the distal humeral epiphysis in children younger than three years old, J Pediatr Orthop 20:173, 2000.
- Oppenheim WL, Calder TJ, Smith C, et al: Supracondylar humeral osteotomy for traumatic childhood cubitus varus deformity, Clin Orthop Relat Res 188:34, 1984.
- Parikh SN, Wall EJ, Foad S, et al: Displaced type II extension supracondylar humerus fractures: do they all need pinning? J Pediatr Orthop 24:380, 2004.
- Peiro A, Mut T, Aracil J, et al: Fracture-separation of the lower humeral epiphysis in young children, Acta Orthop Scand 52:295, 1981.
- Pirone AM, Graham HK, Krajbich JI: Management of displaced extension-type supracondylar fractures of the humerus in children, J Bone Joint Surg 70A:641, 1988.
- Ponce BA, Hedequist DJ, Zurakowski D, et al: Complications and timing of follow-up after closed reduction and percutaneous pinning of supracondylar humerus fractures. Follow-up after percutaneous pinning of supracondylar humerus fractures, J Pediatr Orthop 24:610, 2004.
- Rang M, Moseley CF, Roberts JM, et al: Symposium: management of displaced supracondylar fractures of the humerus, Contemp Orthop 18:497, 1989.
- Rasool MN, Naidoo KS: Supracondylar fractures: posterolateral type with brachialis muscle penetration and neurovascular injury, J Pediatr Orthop 19:518, 1999.
- Re PR, Waters PM, Hresko T: T-condylar fractures of the distal humerus in children and adolescents, J Pediatr Orthop 19:313, 1999.
- Reitman RD, Waters P, Millis M: Open reduction and internal fi xation for supracondylar humerus fractures in children, J Pediatr Orthop 21:157, 2001.
- Roach JW, Hernandez MA: Corrective osteotomy for cubitus varus deformity, J Pediatr Orthop 14:487, 1994.
- Rorabeck CH: A practical approach to compartmental syndromes: III. Management, Instr Course Lect 33:102, 1983.
- Royce RO, Dutkowsky JP, Kasser JR, et al: Neurologic complications after Kirschner wire fi xation of supracondylar humerus fractures in children, J Pediatr Orthop 11:191, 1991.
- Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of the humerus, J Pediatr Orthop 17:303, 1997.
- Shannon FJ, Mohan P, Chacko J, et al: “Dorgan’s” percutaneous lateral cross-wiring of supracondylar fractures of the humerus in children, J Pediatr Orthop 24:376, 2004.
- Shaw BA, Kasser JR, Emans JB, et al: Management of vascular injuries in displaced supracondylar humerus fractures without arteriography, J Orthop Trauma 4:25, 1990.
- Shim JS, Lee YS: Treatment of completely displaced supracondylar fracture of the humerus in children by cross-fi xation with three Kirschner wires, J Pediatr Orthop 22:12, 2002.
- Silberstein MJ, Brodeur AE, Graviss ER: Some vagaries of the capitellum, J Bone Joint Surg 61A:244, 1979.
- Skaggs DL, Cluck MW, Mostofi A, et al: Lateral-entry pin fi xation in the management of supracondylar fractures in children, J Bone Joint Surg 86A:702, 2004.
- Skaggs DL, Hale JM, Bassett J, et al: Operative treatment of supracondylar fractures of the humerus in children, J Bone Joint Surg 83A:735, 2001.
- Smith FM: Children’s elbow injuries: fractures and dislocations, Clin Orthop Relat Res 50:7, 1967.
- Smith L: Deformity following supracondylar fractures of the humerus, J Bone Joint Surg 42A:235, 1960.
- Spinner M, Schreiber SN: Anterior interosseous nerve paralysis as a complication of supracondylar fractures of the humerus in children, J Bone Joint Surg 51A:1584, 1969.
- Swenson AL: The treatment of supracondylar fractures of the humerus by Kirschner wire fi xation, J Bone Joint Surg 30A:993, 1948.
- Thometz JG: Techniques for direct radiographic visualization during closed pinning of supracondylar humerus fractures in children, J Pediatr Orthop 10:555, 1990.
- Topping RE, Blanco JS, Davis TJ: Clinical evaluation of crossedpin versus lateral-pin fi xation in displaced supracondylar humerus fractures, J Pediatr Orthop 15:435, 1995.
- Uchida Y, Ogata K, Sugioka Y: A new three-dimensional osteotomy for cubitus varus deformity after supracondylar fracture of the humerus in children, J Pediatr Orthop 11:327, 1991.
- Vasli LR: Diagnosis of vascular injury in children with supracondylar fractures of the humerus, Injury 9:11, 1988.
- Voss FR, Kasser JR, Trepman E, et al: Uniplanar supracondylar humeral osteotomy with preset Kirschner wires for post-traumatic cubitus varus, J Pediatr Orthop 14:471, 1994.
- Webb AJ, Sherman FC: Supracondylar fractures of the humerus in children, J Pediatr Orthop 9:315, 1989.
- Weber BG, Brunner C, Freuler F, eds: Treatment of fractures in children and adolescents, New York, 1980, Springer-Verlag. Wilkins KE: The operative management of supracondylar fractures, Orthop Clin North Am 21:269, 1990.
- Williamson DM, Coates CJ, Miller RK, et al: Normal characteristics of the Baumann (humerocapitellar) angle: an aid in assessment of supracondylar fractures, J Pediatr Orthop 12:636, 1992.
- Worlock PH, Colton C: Severely displaced supracondylar fractures of the humerus in children: a simple method of treatment, J Pediatr Orthop 7:49, 1987.
- Yates C, Sullivan JA: Arthrographic diagnosis of elbow injuries in children, J Pediatr Orthop 7:54, 1987.
- Fractures of the Shaft and Proximal End of the Humerus, Acromioclavicular Dislocations, and Fractures and Dislocations of the Shaft and Epiphysis of the Clavicle Beaty JH: Fractures of the proximal humerus and shaft in children, Instr Course Lect 41:369, 1992.
- Beringer DC, Weiner DS, Noble JS, et al: Severely displaced proximal humeral epiphyseal fractures: a follow-up study, J Pediatr Orthop 18:31, 1998.
- Curtis RJ Jr: Operative management of children’s fractures of the shoulder region, Orthop Clin North Am 21:315, 1990.
- Dameron TB, Reibel DB: Fractures involving the proximal humeral epiphyseal plate, J Bone Joint Surg 51A:289, 1969.
- Falstie-Jensen S, Mikkelsen P: Pseudodislocation of the
You Might Also Like


