Resection and Excision Techniques for Chronic Osteomyelitis

Key Takeaway
Chronic osteomyelitis often necessitates radical resection of infected and necrotic bone to achieve eradication. While historically challenging in essential long bones, modern reconstructive techniques like Ilizarov bone transport and free composite grafting have revolutionized limb salvage. This guide details the surgical principles, biomechanical considerations, and step-by-step operative techniques for resecting osteomyelitis in nonessential bones, including the metatarsals, calcaneus, fibula, and ilium, ensuring optimal functional recovery and infection control.
PRINCIPLES OF RESECTION AND EXCISION FOR CHRONIC OSTEOMYELITIS
The surgical management of chronic osteomyelitis is predicated on a single, uncompromising principle: the radical resection of all infected, necrotic, and devitalized bone and soft tissue. Antibiotic therapy alone is universally insufficient due to the presence of avascular sequestra and the formation of impenetrable bacterial biofilms. To achieve definitive infection control, the surgeon must approach the infected bone with the same oncologic principles applied to a malignant tumor, resecting back to healthy, bleeding cortical and cancellous bone—often referred to clinically as the "paprika sign."
Historically, massive resection of a long bone affected by chronic hematogenous osteomyelitis was considered inadvisable and often led to amputation. This reluctance was based on three primary factors:
1. Periosteal Failure: The periosteum frequently fails to reproduce the entire resected shaft, leaving a critical-sized defect.
2. Poor Bone Stock: The quality of the remaining host bone is usually sclerotic, avascular, and unsatisfactory for standard reconstructive procedures or hardware fixation.
3. Reactivation of Infection: Extensive reconstructive procedures utilizing hardware can reactivate dormant, encapsulated infections.
However, the paradigm of limb salvage has shifted dramatically. Surgeons have reported highly successful treatments of patients who otherwise would have required amputation by utilizing advanced methods of skeletal reconstruction. These include the open cancellous grafting techniques described by Papineau et al., the use of free vascularized composite grafts (such as the free fibula) pioneered by Weiland, Moore, and Daniel, and the revolutionary techniques of distraction osteogenesis and bone transport introduced by Ilizarov.
Fig. 16-19 A, Defect in the tibia of a 4-year-old child after treatment of acute osteomyelitis by removal of a large sequestrum before sufficient involucrum had formed to ensure the continuity of the bone. B, After transplantation of the fibula to bridge the defect.
With these modern techniques of bone and soft-tissue transport, massive resections can now be performed and reconstructed without significant long-term disability, although the patient must be counseled that the time required for complete reconstruction and consolidation may be extensive.
💡 Clinical Pearl: The Golden Rules of Osteomyelitis Resection
• Aggressive Debridement: Remove only necrotic and infected matter, but do so radically. If the bone does not bleed, it is dead and must be excised.
• Dead Space Management: Following resection, the resulting dead space must be managed with antibiotic-impregnated polymethylmethacrylate (PMMA) beads, spacers, or vascularized muscle flaps.
• Drainage: Close the wound loosely over large-bore rubber or suction drains. Drains must exit through separate, dependent stab incisions to permit direct posterolateral gravity drainage.
DRAINAGE OF PELVIC AND ILIAC ABSCESSES
In the chronic phase of osteomyelitis of the ilium, the entire bone is often involved. The infection can be so diffuse that localized debridement is impossible, necessitating extensive drainage or eventual massive resection. Subperiosteal abscesses frequently strip the gluteal muscles laterally and the iliacus medially.
🔪 Surgical Technique 16-7: Drainage of the Ilium
Positioning and Preparation:
Place the patient in the lateral decubitus position. Ensure the entire hemipelvis and proximal thigh are prepped and draped freely to allow for manipulation of the hip joint if necessary.
Surgical Approach:
1. Incision: Begin the incision along the middle third of the iliac crest. Extend it anteriorly or posteriorly as dictated by the extent of the fluctuance and preoperative imaging.
2. Subperiosteal Dissection: Deepen the incision through the subcutaneous tissue to the iliac crest. Incise the apophysis or periosteum directly over the crest. Strip the muscles subperiosteally from both the medial (iliacus) and lateral (gluteus medius and minimus) cortices of the iliac wing.
3. Abscess Evacuation: Usually, pus under significant pressure will escape immediately upon breaching the periosteum. In chronic cases, the muscles will often already have been stripped away from the bone by the expanding subperiosteal abscesses.
4. Joint Protection: Carefully avoid entering the hip joint. The capsule of the hip joint attaches to the acetabular rim; dissection must remain superior to this level to prevent iatrogenic septic arthritis.
5. Drain Placement: Thoroughly irrigate the abscess cavities. Drain each of the abscess pockets with large-bore gravity or suction drains. Bring the drains out through separate, dependent stab incisions to obtain adequate gravity drainage.
6. Closure: Close the skin loosely to prevent the reaccumulation of purulent material under tension.
Postoperative Protocol (Aftertreatment):
Because a severe flexion contracture of the hip usually develops as a result of the inflammatory irritability of the hip flexor muscles (iliopsoas and rectus femoris), Buck traction is applied immediately postoperatively. The patient is turned frequently to the affected side to promote continuous gravity drainage.
MASSIVE RESECTION OF NONESSENTIAL BONES
While essential long bones (femur, tibia, humerus, radius, ulna) require complex reconstruction following resection, massive resection of nonessential bones involved by any type of chronic osteomyelitis can be performed safely without the need for structural bone grafting. Bones such as the metatarsals (excluding the first), tarsals, part of the calcaneus, the proximal three-fourths of the fibula, the ilium, ribs, clavicle, and scapula can be radically resected while still retaining highly satisfactory patient function.
Resection of the Metatarsals
Chronic osteomyelitis of the forefoot frequently involves the metatarsals, often secondary to diabetic foot ulcers or penetrating trauma.
⚠️ Surgical Warning: Biomechanics of the First Ray
The first metatarsal is the primary load-bearing structure of the forefoot, absorbing approximately 50% of the forces during the toe-off phase of the gait cycle. The first metatarsal should be retained if at all possible. Resection of the first ray leads to significant transfer metatarsalgia and biomechanical collapse of the medial column.
🔪 Surgical Technique 16-8: Metatarsal Resection
- Incision: Make a dorsal longitudinal incision directly over the affected metatarsal bone, extending from the distal row of the tarsals to the middle of the proximal phalanx of the corresponding toe.
- Soft Tissue Dissection: Deepen the incision through the subcutaneous tissues directly to the periosteum. Crucially, do not open the extensor tendon sheaths. Breaching the tendon sheaths can allow the infection to track proximally into the leg or distally into the digits.
- Periosteal Stripping: Incise the periosteum in line with the metatarsal shaft. Using a Freer or Key elevator, strip the periosteum completely from the circumference of the bone.
- Resection: Resect the entire infected shaft using an oscillating saw or bone-cutting forceps.
- Pediatric Consideration: Preserve the physis whenever possible in children to allow for continued longitudinal growth (the physis is proximal in the 1st metatarsal and distal in the 2nd-5th metatarsals).
- Closure: Thoroughly irrigate the bed and close the wound loosely over a small drain.
Postoperative Protocol:
A posterior plaster splint is applied to maintain the ankle in neutral and protect the forefoot. This is worn until the wound has completely healed. Following soft-tissue consolidation, protected weight-bearing is started, often utilizing a custom orthosis with a metatarsal pad to redistribute plantar pressures.
Resection of the Tarsals and Partial Calcanectomy
Often, more than one tarsal bone may be involved in chronic osteomyelitis of the midfoot or hindfoot. If necessary, the affected tarsal or tarsals can be excised using combined dorsolateral and dorsomedial longitudinal incisions to avoid the central neurovascular bundle (dorsalis pedis artery and deep peroneal nerve).
If the calcaneus is diffusely involved, the classic split-heel approach of Gaenslen is recommended to provide complete access to the body of the calcaneus. However, for localized heel ulcerations with underlying calcaneal osteomyelitis, a partial calcanectomy is highly effective. Smith et al. demonstrated that partial calcanectomy yields good functional results, with 9 out of 12 patients maintaining their preoperative level of mobility.
🔪 Surgical Technique 16-9: Partial Calcanectomy
- Incision Planning: Tailor the incision to fit the size and shape of the existing plantar ulcer. The goal is to excise the ulcer completely while maintaining viable local tissue. If no ulcers are present, utilize Gaenslen’s longitudinal split-heel approach.
- Soft Tissue Protection: Carry the dissection down to the calcaneus with extreme care to protect the remaining viable plantar heel pad. The specialized fat pad of the heel is irreplaceable for weight-bearing.
- Achilles Tendon Management: Approach the Achilles tendon in the area of the posterior calcaneus that is to be removed. Release the tendon from its insertion and allow it to retract proximally.
- Osteotomy: Begin the bony resection with an oscillating saw, starting the cut approximately 1 cm posterior to the edge of the subtalar and calcaneocuboid joints. Angle the cut to remove the entire posteroinferior tuberosity.
- Wound Approximation: Remove sufficient bone to permit the tension-free mobilization and approximation of the adjacent healthy soft tissue over the raw cancellous bone surface.
- Closure: Close the wounds over suction drains. If primary skin closure is impossible due to tissue loss, pack the wound and allow it to heal by secondary intention or apply negative pressure wound therapy (NPWT).
- Immobilization: Apply a cast with the ankle in 30 degrees of equinus. This plantarflexed position is critical to reduce tension on the posterior skin closure.
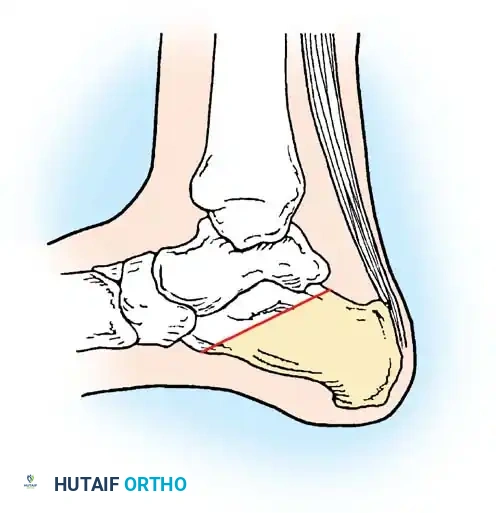
Fig. 16-20 Partial resection of the calcaneus. The shaded area represents the resected infected bone, allowing for soft tissue closure over the defect. (From Smith DG, Stuck RM, Ketner L, et al: Partial calcanectomy for the treatment of large ulcerations of the heel and calcaneal osteomyelitis, J Bone Joint Surg 74A:571, 1992.)
Postoperative Protocol:
When the wounds have fully healed, the patient is placed in a solid, custom-molded ankle-foot orthosis (AFO). Because the Achilles tendon lever arm has been sacrificed, the AFO is necessary to substitute for the lost plantarflexion power and prevent a calcaneal gait pattern.
Resection of the Fibula
The fibula is a largely non-weight-bearing bone, transmitting only about 10-15% of the axial load of the lower extremity. Consequently, the entire proximal three-fourths of the fibula can be resected if necessary.
⚠️ Surgical Warning: The Distal Fibula
The distal fourth of the fibula (the lateral malleolus) is an absolute requirement for the stability of the ankle mortise. It must be retained whenever possible. If the distal fibula is resected, a complex tibiotalar or pantalar arthrodesis is usually required to provide a stable, plantigrade foot.
Furthermore, if the extreme proximal end (fibular head) is resected, the stabilizing structures of the lateral knee—namely the fibular collateral ligament (LCL) and the biceps femoris tendon—must be firmly anchored to the lateral condyle of the tibia to prevent posterolateral rotatory instability.
🔪 Surgical Technique 16-10: Fibular Resection
- Incision: Make a direct longitudinal incision over the involved portion of the fibula.
- Internervous Plane: Approach the bone through the safe internervous interval between the soleus muscle posteriorly (innervated by the tibial nerve) and the peroneal muscles anteriorly (innervated by the superficial peroneal nerve).
- Nerve Protection: Expose and meticulously protect the common peroneal nerve in the proximal end of the wound as it winds around the fibular neck. Retract it gently with a vessel loop.
- Periosteal Stripping: Incise the periosteum in line with the shaft. Using a circumferential stripping technique, separate the periosteum from the entire circumference of the part to be resected.
- Resection and Closure: Resect the diseased portion of the shaft using a Gigli saw or oscillating saw. Copiously irrigate the bed and close the wound loosely over deep suction drains.
Postoperative Protocol:
A long leg posterior plaster splint is applied with the foot in a neutral position, the ankle at exactly 90 degrees, and the knee in 20 degrees of flexion. This splint is worn until the wound has healed, after which protected weight-bearing is initiated.
Resection of the Iliac Wing
Resection of a large portion of the iliac wing is a formidable but highly effective procedure. It is primarily indicated in cases of chronic, refractory osteomyelitis of the ilium associated with prolonged, draining sinus tracts. This condition is often seen following infected pelvic trauma or as a complication after harvesting a large structural iliac crest bone graft.

Fig. 16-21 A, Sliding abdominal hernia and osteomyelitis of the right iliac crest after the removal of a bone graft for fusion of the lumbar spine. B, Appearance of the ilium after radical resection of the involved crest and repair of the abdominal hernia.
🔪 Surgical Technique 16-11: Iliac Wing Resection
Anatomical Considerations:
The iliac crest serves as the origin and insertion for multiple powerful muscle groups. Superiorly, the abdominal musculature (external oblique, internal oblique, transversus abdominis) attaches. Laterally, the tensor fasciae latae (TFL) and gluteal muscles originate. Medially, the iliacus muscle fills the iliac fossa.
- Incision: Make an extensive incision over the iliac crest, beginning at the posterior superior iliac spine (PSIS) and extending anteriorly to the anterior superior iliac spine (ASIS). From the ASIS, extend the incision distally onto the thigh, running parallel with the sartorius muscle for 7.5 to 10 cm (Fig. 16-22A).
- Fascial Incision: Divide the fascia approximately 1.3 cm distal to the crest, and incise the periosteum directly along the ridge of the crest.
- Lateral Dissection: Detach the gluteal muscles and the tensor fasciae latae subperiosteally, sweeping them inferiorly down to the level of the acetabular rim.
- Anterior Exposure: Develop the interval between the tensor fasciae latae (superior gluteal nerve) and the sartorius muscle (femoral nerve). Retract the TFL laterally to expose the anterior aspect of the ilium.
- Pediatric Consideration: In children, the cartilaginous iliac crest apophysis can be detached easily with the abdominal muscles still attached to it, preserving the abdominal wall integrity.
- Superior and Posterior Dissection: Subperiosteally detach the abdominal muscles superiorly. Posteriorly, detach the latissimus dorsi, quadratus lumborum, and erector spinae muscles at their insertions on the posterior crest.
- Medial Dissection: Strip the iliacus muscle from the medial cortex of the ilium, sweeping it distally down to the arcuate line (iliopectineal line) (Fig. 16-22B).
- En Bloc Resection: With the iliac wing completely skeletonized, resect the ilium as a whole. The resection can be carried as far distally as the anterior inferior iliac spine (AIIS) and as far posteriorly as the sacroiliac joint if the extent of the osteomyelitis demands it.
- Drainage and Closure: Place large-bore suction drains deep in the wound bed. Bring them out through the skin via a separate, dependent stab incision to establish adequate gravity drainage. Close the skin loosely to prevent hematoma formation.

You Might Also Like

