Unusual Musculoskeletal Infections: Comprehensive Surgical Management
Key Takeaway
Atypical musculoskeletal infections, including nontuberculous mycobacteria, brucellosis, Lyme disease, and fungal osteomyelitis, present significant diagnostic and therapeutic challenges. These insidious pathogens often mimic common bacterial infections or neoplastic processes. Successful management requires a high index of suspicion, precise histopathological and microbiological identification, and a multidisciplinary approach. Surgical intervention—ranging from radical debridement and synovectomy to complex arthrodesis—is frequently necessary to eradicate chronic osteoarticular involvement and restore functional biomechanics.
INTRODUCTION TO ATYPICAL MUSCULOSKELETAL INFECTIONS
While Staphylococcus aureus and standard pyogenic organisms account for the vast majority of osteoarticular infections, orthopaedic surgeons must maintain a high index of suspicion for atypical pathogens. These unusual infections—ranging from nontuberculous mycobacteria and zoonotic bacteria to endemic fungi—often present with an insidious onset, lacking the classic systemic signs of acute sepsis. Delayed diagnosis can lead to devastating joint destruction, chronic osteomyelitis, and severe functional impairment. Management mandates a synergistic approach combining targeted, often prolonged, antimicrobial chemotherapy with meticulous surgical debridement, synovectomy, and structural reconstruction.
NONTUBERCULOUS MYCOBACTERIAL (NTM) INFECTIONS
Musculoskeletal infections caused by nontuberculous Mycobacterium species have seen a marked increase since the mid-1980s. To date, literature implicates at least 15 different species of Mycobacterium in osteoarticular and tenosynovial infections. The most frequently isolated causative organisms are Mycobacterium avium complex (MAC), Mycobacterium marinum, and Mycobacterium kansasii.
Clinically, radiographically, and histopathologically, NTM infections are virtually indistinguishable from musculoskeletal tuberculosis. Patients frequently present with chronic, progressive swelling, erythema, and restricted range of motion, particularly in the hand and wrist (e.g., "fish tank granuloma" caused by M. marinum).
Clinical Pearl: Optimal culture requirements for NTM species vary significantly. M. marinum grows optimally at 30ºC to 33ºC. Failure to inform the microbiology laboratory of the suspected diagnosis will result in false-negative cultures at standard incubation temperatures.
Surgical Management: Radical Tenosynovectomy
The operative principles for NTM infections mirror those of musculoskeletal tuberculosis. Medical management alone is often insufficient due to poor antibiotic penetration into hypertrophic, avascular granulomatous tissue.
Indications:
* Failure of conservative antimicrobial therapy.
* Progressive tenosynovitis with impending tendon rupture.
* Nerve compression (e.g., carpal tunnel syndrome secondary to flexor tenosynovitis).
Positioning and Preparation:
* The patient is positioned supine with the affected extremity on a radiolucent hand table.
* A well-padded pneumatic tourniquet is applied to the proximal arm to ensure a bloodless field.
Surgical Approach (Volar Wrist/Hand):
1. Incision: Utilize an extensile volar approach, incorporating Brunner zigzag incisions across flexion creases to prevent postoperative contractures.
2. Exposure: Identify and protect the median and ulnar nerves. The transverse carpal ligament is routinely released to decompress the carpal tunnel and access the deep flexor compartment.
3. Debridement: Perform a meticulous, radical tenosynovectomy. Exise all hypertrophic, "rice body"–laden synovium.
4. Tendon Preservation: Carefully dissect the granulomatous tissue away from the flexor tendons. Preserve the critical annular pulleys (A2 and A4) to prevent tendon bowstringing.
5. Closure: Copious irrigation is performed. The wound is closed primarily if tension-free, or left open for delayed primary closure or grafting if severe skin compromise exists.
Postoperative Protocol:
Early active range of motion is initiated within 24 to 48 hours to prevent tendon adhesions. Prolonged multidrug chemotherapy (e.g., rifabutin and clarithromycin for MAC) is directed by an infectious disease specialist based on susceptibility testing.
BRUCELLOSIS
Brucellosis is a zoonotic infection caused by a gram-negative coccobacillus. Of the six recognized species, Brucella melitensis (goats/sheep) is responsible for the majority of human infections worldwide, while B. abortus (cattle) is more common in North America and Central Europe. Transmission occurs via ingestion of unpasteurized dairy products or direct contact with infected animal tissues.
Approximately 66% of patients with brucellosis present with musculoskeletal symptoms. Spinal involvement is the most common osteoarticular manifestation, frequently affecting the superior vertebral endplate. This creates a characteristic "parrot beak" osteophytic configuration on plain radiographs, which can progress to frank osteomyelitis, discitis, and epidural abscess formation.
Diagnostic Pitfall: Brucella epidural abscesses can perfectly mimic the neurological presentation of a herniated nucleus pulposus. Diagnosis relies on a Brucella agglutinin titer of 1:160 or higher, or positive bone biopsy cultures.
Surgical Management of Brucella Spondylitis
Indications:
* Progressive neurological deficit secondary to epidural compression.
* Spinal instability or severe kyphotic deformity.
* Large, refractory psoas abscesses causing mechanical compression (e.g., abdominal aortic arterial thrombosis).
Surgical Approach:
* Anterior Debridement: An anterior approach (e.g., retroperitoneal or transthoracic) is preferred for direct access to the infected vertebral bodies.
* Corpectomy and Fusion: Infected bone and disc material are radically excised back to bleeding, healthy bone. Structural support is restored using autologous bone graft (iliac crest or rib) or titanium mesh cages.
* Instrumentation: Supplemental posterior pedicle screw instrumentation may be required if significant instability exists.
TYPHOID FEVER (SALMONELLA OSTEOMYELITIS)
Caused by Salmonella typhi, a gram-negative anaerobic bacillus, typhoid fever is primarily transmitted via the oral-fecal route. While systemic symptoms (fever, hepatosplenomegaly, gastrointestinal infiltration) predominate, approximately 30% of patients develop arthralgias.
Septic sacroiliitis and osteomyelitis can occur, most frequently affecting the thoracolumbar junction with accompanying disc involvement. Isolated long bone osteomyelitis is rare but can present with profound bone marrow infiltration, suppression, and necrosis.
Treatment:
Traditional primary antibiotic treatment utilizes chloramphenicol, though third-generation cephalosporins (e.g., ceftriaxone) are highly effective and preferred for resistant strains. Surgical intervention is reserved for abscess drainage, debridement of necrotic bone, or stabilization of pathological fractures.
SYPHILIS
Treponema pallidum, a spirochete transmitted sexually or transplacentally, can involve bone at any stage.
* Congenital Syphilis: Characterized by periostitis of the temporal bone and palate, and cortical thickening of the anterior tibia ("saber shins").
* Tertiary Syphilis: Neuropathic joint destruction (Charcot arthropathy) can develop secondary to tabes dorsalis (loss of proprioception and deep pain sensation).
Surgical Considerations:
The mainstay of treatment is penicillin benzathine. Operative intervention for active syphilitic osteitis is rarely required. However, the resultant Charcot joints may require complex arthrodesis. Arthrodesis in neuropathic joints carries a high nonunion rate; therefore, rigid internal fixation (often utilizing intramedullary nails or dual plating) combined with robust bone grafting and prolonged immobilization is mandatory.
ACTINOMYCOSIS
Actinomycosis is a chronic, suppurative, granulomatous disease characterized by the formation of external sinus tracts. It is caused by Actinomyces israelii, a gram-positive, anaerobic, filamentous bacterium (not a fungus).
Histopathological Marker: Diagnosis is confirmed by the identification of macroscopic "sulfur granules" (yellowish colonies of organisms) or branching mycelia in the purulent exudate.
Actinomycotic osteomyelitis most frequently affects the cervicofacial region (mandible) via direct extension from soft tissues. Spinal involvement can mimic tuberculosis but classically spares the intervertebral disc, presenting with dense sclerotic changes and preserved vertebral body height. Treatment consists of high-dose penicillin and image-guided aspiration or surgical incision and drainage of large abscesses.
LYME DISEASE
Lyme disease, caused by the spirochete Borrelia burgdorferi and transmitted by Ixodes ticks, progresses through three clinical stages: cutaneous (erythema migrans), early disseminated (cardiac/neurological), and late arthritic.
The arthritic stage occurs in approximately 60% of untreated patients. It typically presents as a monoarticular or oligoarticular inflammatory arthritis, with the knee being the most commonly affected joint. Chronic Lyme arthritis can lead to aggressive pannus formation, cartilage destruction, and joint space narrowing.
Surgical Management: Arthroscopic Synovectomy
Indications:
Chronic Lyme arthritis of the knee that is refractory to 2 to 3 months of appropriate oral and intravenous antibiotic therapy (e.g., doxycycline, ceftriaxone).
Surgical Technique:
1. Setup: Standard knee arthroscopy setup with a thigh tourniquet.
2. Portals: Standard anterolateral and anteromedial portals are established. Superomedial and superolateral portals are often required for complete access to the suprapatellar pouch.
3. Synovectomy: A motorized shaver and radiofrequency ablation wand are used to perform a comprehensive anterior and posterior synovectomy. Care must be taken to resect the hypertrophic pannus from the medial and lateral gutters, the intercondylar notch, and the posterior compartments.
4. Postoperative Care: Immediate weight-bearing as tolerated and aggressive physical therapy to restore terminal extension and full flexion.
FUNGAL OSTEOMYELITIS AND ARTHRITIS
Fungal osteomyelitis develops insidiously. Because definitive diagnosis relies on specific fungal stains (e.g., Gomori methenamine silver, Periodic acid-Schiff) and prolonged cultures, the surgeon must suspect the diagnosis clinically. Treatment is highly complex, requiring collaboration with infectious disease specialists for prolonged antifungal therapy (e.g., Amphotericin B, ketoconazole, itraconazole).
Coccidioidomycosis
Endemic to the southwestern United States (San Joaquin Valley) and parts of Latin America, Coccidioides immitis is transmitted via inhalation. While usually confined to the lungs, disseminated disease can cause granulomatous lesions in bone (15% of disseminated cases).
Lesions typically affect the metaphyses of tubular bones, bony prominences, and ligamentous attachments. Radiographically, they appear as well-circumscribed lytic lesions with sclerotic margins. Direct extension into large weight-bearing joints can cause severe monoarticular arthritis.
Surgical Management:
* Saucerization: For chronic osseous lesions, the bone is unroofed (saucerized). All overhanging cortical bone is resected with a high-speed burr until healthy, bleeding cancellous bone is reached, eliminating dead space where the fungus can harbor.
* Joint Involvement: Radical synovectomy is required. If the articular cartilage is irreparably destroyed, formal arthrodesis of the joint is the most reliable method to eradicate the infection and provide a stable, painless limb.
Blastomycosis
Caused by Blastomyces dermatitidis, a dimorphic soil-dwelling fungus endemic to the Ohio and Mississippi river valleys. Skeletal infection occurs via hematogenous dissemination from the lungs.
In long bones, Blastomyces exhibits a unique propensity to localize in the epiphysis, frequently extending directly into the adjacent joint space. Vertebral lesions closely mimic tuberculosis. Definitive diagnosis requires the microscopic identification of characteristic broad-based budding yeast. Treatment relies on Amphotericin B, with surgical debridement reserved for joint extension or spinal instability.
Histoplasmosis
Histoplasma capsulatum typically causes a mild, self-limiting pulmonary infection. However, in immunocompromised hosts, or rarely in immunocompetent individuals, it can disseminate to bone and soft tissues.
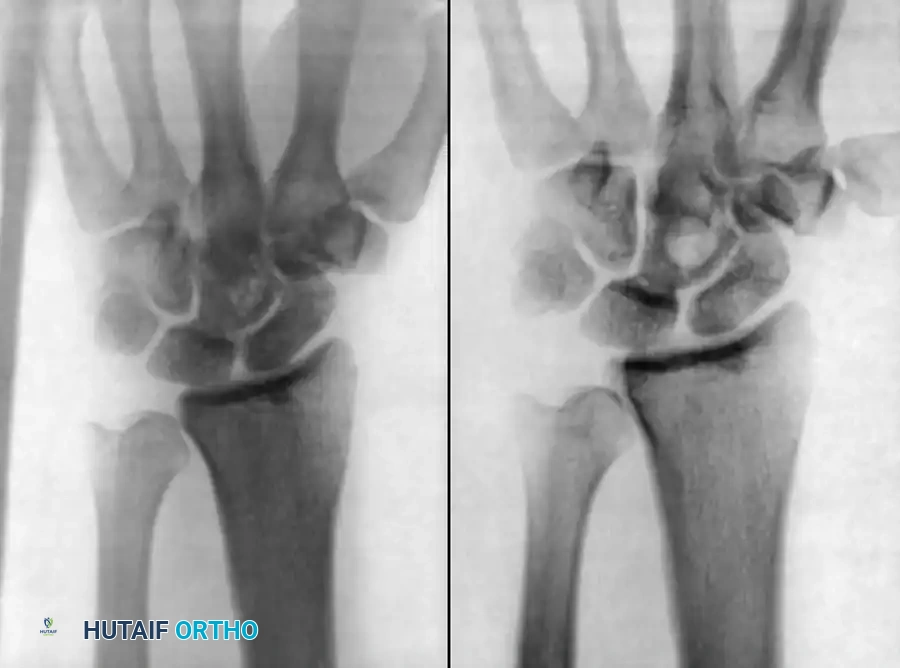
Care and Lacey described a unique case of recurrent histoplasmosis in the wrist of an immunocompetent patient without pulmonary involvement. The prolonged latency period suggests that Histoplasma can remain dormant in the bone marrow for decades before reactivating.
Figure 18-10: Radiographic presentation of recurrent Histoplasmosis in the wrist, demonstrating profound lytic destruction of the carpal rows and distal radius articular surface.
Surgical Management of Carpal Fungal Osteomyelitis:
1. Approach: A dorsal longitudinal approach to the wrist is utilized, centered over the Lister tubercle.
2. Extensor Retinaculum: The third compartment is opened, and the extensor pollicis longus is transposed. The second and fourth compartments are elevated subperiosteally.
3. Radical Debridement: Grossly infected and necrotic carpal bones are excised. In cases of severe destruction (as seen in Fig 18-10), a proximal row carpectomy or complete carpectomy may be necessary.
4. Reconstruction: Depending on the extent of bone loss and infection eradication, a delayed total wrist arthrodesis using a dorsal spanning plate and robust iliac crest autograft is performed once the fungal burden is cleared via systemic antifungals (itraconazole).
CONCLUSION
Unusual musculoskeletal infections demand a rigorous, evidence-based approach. The orthopaedic surgeon must look beyond standard pyogenic pathogens when faced with indolent clinical courses, atypical radiographic features, or patients from specific endemic regions. Mastery of both radical surgical debridement techniques and the nuances of targeted antimicrobial therapy is essential to achieve eradication and restore patient function.
You Might Also Like
