Biology and Surgical Management of Spinal Infections
Key Takeaway
Spinal infections primarily originate in the highly vascularized vertebral metaphyses and cartilaginous endplates rather than the avascular intervertebral disc. Pyogenic bacteria typically disseminate via arterial routes, while tuberculous infections often utilize the venous system, specifically Batson's plexus. Understanding this complex microvascular anatomy is critical for accurate diagnosis, determining surgical indications, and executing meticulous operative debridement and stabilization in affected patients.
BIOLOGY OF SPINAL INFECTION: ANATOMICAL AND VASCULAR FOUNDATIONS
A profound knowledge of the structure, composition, and microvasculature of the spinal elements is the absolute prerequisite for understanding the pathogenesis, progression, and surgical management of spinal infections. Historically, the intervertebral disc was erroneously identified as the primary nidus for spinal infections. However, contemporary evidence-based literature unequivocally points to the highly vascularized metaphyses and cartilaginous endplates as the primary starting areas for blood-borne (hematogenous) infections. Today, the intervertebral disc space is considered the primary starting area only in cases of direct inoculation, such as iatrogenic introduction during surgery or discography.
Microscopic Anatomy of the Intervertebral Disc and Endplate
In 1945, Coventry, Ghormley, and Kernohan provided a seminal description of the microscopic anatomy of the intervertebral disc and its contiguous structures. Their critical conclusion was that in adults older than 30 years, the intervertebral disc is essentially avascular; it receives its nutrition entirely from tissue fluid diffusion rather than from a direct blood supply.
They identified multiple perforations in the bony endplates of the vertebral bodies, which correspond directly with the marrow cavities. These perforations are arranged in three distinct anatomical zones:
1. The Central Zone: Characterized by numerous small perforations.
2. The Peripheral Zone: Characterized by fewer, but significantly larger, perforations.
3. The Epiphyseal Ring: A dense ring surrounding the endplate that overlaps the outer surface of the vertebral body, joining the more concave surface of the central and peripheral zones internally.
Adjacent to the bony endplate lies the cartilaginous plate, composed of hyaline cartilage, which forms the critical inner boundary between the osseous vertebral body and the fibrous intervertebral disc.
Clinical Pearl: The avascular nature of the adult intervertebral disc makes it an immunologically privileged site. Once bacteria breach the cartilaginous endplate and enter the disc space, the lack of direct blood supply severely limits the efficacy of the host immune response and systemic antibiotic penetration, often necessitating surgical debridement.
In 1981, Inoue further elucidated the biomechanical adherence of the disc to the vertebral endplate. He discovered that the disc is firmly adherent at its periphery, where two-thirds of its collagenous fibers insert perpendicularly into the endplate (Sharpey's fibers). Conversely, the central portion is less firmly attached, with fibers running parallel to the endplate. This specific architectural composition facilitates the diffusion of nutrients through the endplate perforations into the central nucleus pulposus without compromising the structural integrity of the motion segment under axial load.
VASCULAR ANATOMY OF THE SPINE
The arterial and venous supply to the vertebrae dictates the specific patterns of hematogenous bacterial seeding.
Arterial Supply and Microvasculature
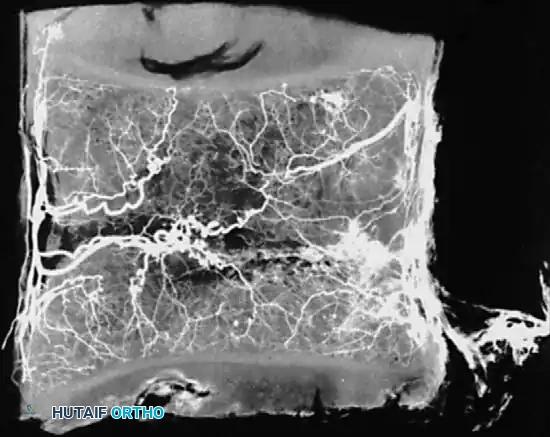
In 1959, Wiley and Trueta demonstrated marked similarities in the arterial and venous supply across the cervical, thoracic, and lumbar levels. At each vertebral level, nutrient vessels derived from the vertebral, intercostal, or lumbar arteries enter the vertebral body.
Posterior spinal branch arteries enter the spinal canal through each neural foramen. These arteries bifurcate into ascending and descending branches that anastomose with corresponding branches at adjacent levels. This posterior network converges centrally to enter a large posterior nutrient foramen.
Whalen et al. investigated the microvasculature of the vertebral endplates, describing vessels oriented obliquely within the cartilage, directing toward the intervertebral disc. These vessels originate from circumferential vessels fed by the arterial plexus outside the perichondrium or from adjacent metaphyseal marrow vessels.
Crucially, Whalen's team concluded that the intervertebral disc is avascular even in infants, whereas the surrounding cartilaginous material is highly vascular. The cartilaginous endplate represents the anatomical terminus of the arterial supply, regardless of the patient's age.
Venous Drainage and Batson's Plexus
The venous drainage of the spine is equally critical to the pathophysiology of infection. First described by Breschet in 1819 and expanded by Batson in 1940, the valveless pelvic venous plexus drains directly into the spinal venous plexus (Batson's plexus). This valveless, bidirectional flow perfectly explains the frequent metastasis of pelvic tumors and the spread of genitourinary infections to the spine.
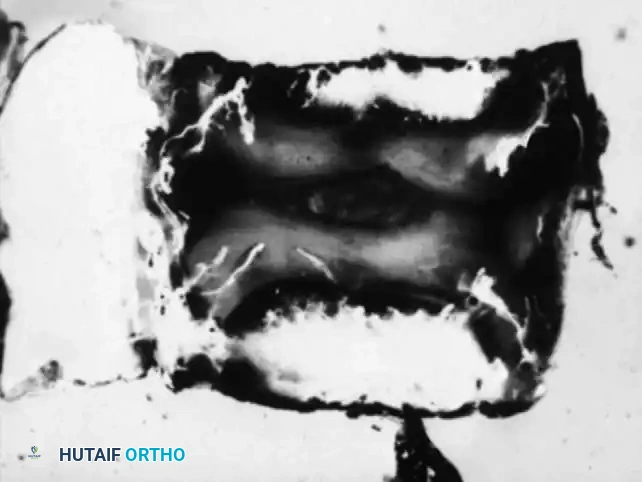
In 1976, Crock and Yoshizawa mapped the venous microcirculation of the vertebral endplate. The venous system begins exactly where the arterial circulation ends. Large subvenous channels run horizontally and parallel to the endplate. This horizontal system drains through small vertical veins that perforate the endplate, connecting with horizontal vessels in the adjacent cancellous bone.
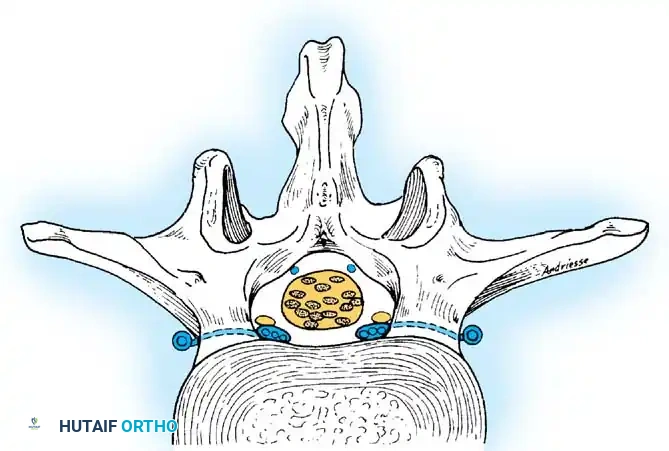
These vertical veins drain into the basivertebral system, converging to form the anterior internal venous plexus. Externally, these vessels anastomose with the anterior internal vertebral, posterior internal vertebral, and posterior radicular veins.
Surgical Warning: The anterior internal veins lie in the lateral aspect of the floor of the spinal canal bilaterally. These veins are routinely sacrificed during radical disc excision and corpectomy. Meticulous bipolar coagulation or the use of hemostatic agents (e.g., bone wax, thrombin-soaked matrices) is mandatory to prevent obscuring the surgical field and postoperative epidural hematoma.
PATHOGENESIS AND ROUTES OF INFECTION
Spinal infections manifest through three primary routes:
- Arterial Spread (Pyogenic Spondylodiscitis): The most common method of spinal infection is the arterial dissemination of pyogenic bacteria (most frequently Staphylococcus aureus). This infection originates in the highly vascularized metaphyseal endplate of the vertebra—likely within the sluggish venous channels where bacteria can easily lodge—and spreads secondarily to the avascular disc as the destructive process progresses.
- Venous Spread (Tuberculous Spondylitis / Pott's Disease): Because tuberculous spinal infection has been experimentally reproduced only by injecting the renal vein (as demonstrated by Hodgson), it is widely accepted that Mycobacterium tuberculosis disseminates via venous spread, utilizing Batson's plexus. This is substantiated by the high frequency of concurrent genitourinary tuberculous disease.
- Direct Inoculation and Contiguous Spread: Infection can occur via direct inoculation (e.g., surgical manipulation, discography, epidural injections) or by local spread from contiguous structures. Contiguous spread has been documented from subphrenic abscesses, colonic perforations, and retroperitoneal abscesses extending from penetrating trauma.
SURGICAL MANAGEMENT OF SPINAL INFECTIONS
While many spinal infections can be managed with prolonged culture-directed intravenous antibiotics and rigid orthosis, surgical intervention becomes mandatory under specific clinical scenarios.
Indications for Surgery
- Progressive neurological deficit (e.g., epidural abscess causing cord or cauda equina compression).
- Spinal instability or progressive kyphotic deformity due to extensive anterior column destruction.
- Failure of medical management (persistent elevated inflammatory markers and intractable pain despite 4-6 weeks of appropriate IV antibiotics).
- Need for open biopsy when percutaneous image-guided biopsy fails to yield a causative organism.
- Intractable pain severely limiting mobilization.
Preoperative Planning and Positioning
Thorough preoperative imaging is essential. Gadolinium-enhanced MRI is the gold standard for evaluating the extent of the epidural abscess, discitis, and osteomyelitis. A fine-cut CT scan is invaluable for assessing the degree of bony destruction and planning instrumentation.
Positioning:
For the standard posterior approach, the patient is positioned prone on a radiolucent Jackson table with all bony prominences meticulously padded. The abdomen must hang free to decrease intra-abdominal pressure, thereby reducing venous engorgement in Batson's plexus and minimizing intraoperative epidural bleeding. For anterior approaches (e.g., retroperitoneal or transthoracic), the patient is positioned in the lateral decubitus position.
Step-by-Step Surgical Approach: Anterior Debridement and Fusion
Because spinal infections predominantly destroy the anterior column (vertebral body and disc), the anterior approach allows for direct, radical debridement of the infected tissue and placement of a load-sharing structural graft.
- Exposure: Depending on the level, a left-sided retroperitoneal approach (lumbar) or transthoracic approach (thoracic) is utilized. The left side is preferred in the lumbar spine to mobilize the aorta rather than the more fragile inferior vena cava.
- Vascular Mobilization: The segmental vessels over the infected vertebral bodies are carefully identified, ligated, and divided. This allows safe mobilization of the great vessels away from the spine.
- Radical Debridement (Corpectomy):
- The infected intervertebral discs above and below the involved vertebrae are excised.
- Using a high-speed burr, rongeurs, and curettes, the necrotic, infected bone of the vertebral body is radically resected.
- Crucial Step: Debridement must continue until healthy, bleeding cancellous bone is encountered at the superior and inferior endplates. Leaving avascular, necrotic bone guarantees persistent infection.
- Epidural Decompression: If an epidural abscess is present, the posterior longitudinal ligament (PLL) is resected to fully decompress the ventral dural sac.
- Structural Grafting: Once the bed is sterilized of gross purulence and necrotic tissue, a structural graft is inserted. While autologous tricortical iliac crest is the gold standard for infection, titanium mesh cages packed with autograft or allograft are increasingly used with high success rates, as titanium is highly resistant to bacterial biofilm formation.
Posterior Instrumentation and Stabilization
In cases of significant instability or multi-level debridement, supplemental posterior instrumentation is required.
- Pedicle Screw Fixation: Utilizing fluoroscopic or navigation guidance, pedicle screws are placed at least one (preferably two) levels above and below the infected segment.
- Avoidance of the Infected Zone: Posterior laminectomy alone without stabilization is contraindicated in anterior column infections, as it destabilizes the posterior tension band, leading to catastrophic kyphotic collapse.
- Wound Closure: Copious irrigation with normal saline (often >9 liters) is performed. Vancomycin powder may be applied locally. Deep subfascial drains are placed before meticulous, multi-layer closure.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative management of spinal infections requires a multidisciplinary approach involving orthopedic surgery, infectious disease, and physical medicine and rehabilitation.
- Antimicrobial Therapy: Intravenous antibiotics are continued postoperatively. The regimen is strictly tailored to intraoperative deep tissue cultures. A standard course consists of 6 weeks of IV antibiotics, often followed by a prolonged course of oral suppressive therapy depending on the organism and inflammatory marker trends (CRP and ESR).
- Mobilization: Early mobilization is encouraged to prevent deep vein thrombosis, atelectasis, and deconditioning. Depending on the rigidity of the internal fixation, a rigid cervicothoracic or thoracolumbosacral orthosis (TLSO) may be prescribed for 6 to 12 weeks to restrict micromotion and promote arthrodesis.
- Monitoring: Weekly monitoring of CRP and ESR is conducted. A steady decline in CRP is the most reliable indicator of infection eradication.
- Follow-up Imaging: Upright plain radiographs are obtained at 2, 6, and 12 weeks to assess spinal alignment and graft incorporation. MRI is generally not repeated early in the postoperative phase unless there is a new neurological deficit, as postoperative edema and granulation tissue can mimic persistent infection.
Understanding the intricate biology and microvascular anatomy of the spine is not merely an academic exercise; it is the fundamental basis upon which successful, life-saving surgical interventions for spinal infections are built.
📚 Medical References
You Might Also Like
