Volar Approach to Flexor Tendons: Comprehensive Surgical Anatomy, Indications, & Principles
Key Takeaway
The volar approach provides essential exposure for hand flexor tendons, nerves, and vessels. It is indicated for primary tendon repair, nerve/vessel reconstruction, and drainage of pyogenic flexor tenosynovitis. Understanding its intricate surgical anatomy, including FDS, FDP, and pulley systems, is crucial for restoring optimal hand function and minimizing complications.
Introduction & Epidemiology
The volar approach to the flexor tendons represents a foundational and indispensable technique in hand surgery, offering unparalleled exposure to the intricate anatomy of the digital and palmar flexor systems, as well as the associated neurovascular structures. Its versatility makes it the cornerstone for managing a broad spectrum of pathologies, ranging from acute traumatic injuries to chronic inflammatory conditions and neoplastic processes.
Flexor tendon injuries, in particular, constitute a significant portion of hand trauma, with an estimated incidence of 3-5 cases per 10,000 person-years. These injuries predominantly affect young, active individuals and can result from lacerations, avulsions, or closed ruptures. The fingers are most commonly involved, followed by the palm and wrist. The delicate balance required for optimal hand function necessitates precise surgical repair and meticulous rehabilitation, underscoring the critical importance of a clear and reproducible surgical approach. The volar incision facilitates direct visualization, minimizing iatrogenic damage and optimizing conditions for repair, which is paramount for restoring functional outcomes and preventing long-term disability.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy and biomechanics of the flexor tendon system is non-negotiable for any surgeon employing a volar approach. The digital flexor system comprises the Flexor Digitorum Superficialis (FDS) and Flexor Digitorum Profundus (FDP) tendons. The FDP tendon originates from the ulna and interosseous membrane, inserting onto the volar base of the distal phalanx, primarily responsible for DIP joint flexion. The FDS tendon originates from the medial epicondyle, ulna, and radius, typically bifurcating around the FDP in the region of the proximal phalanx (Camper's chiasm) before inserting onto the middle phalanx, primarily flexing the PIP joint.
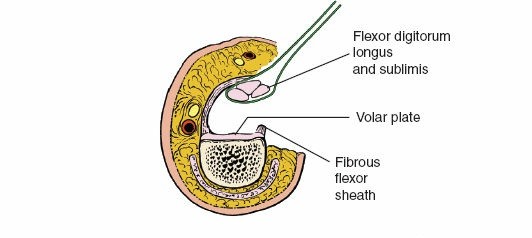
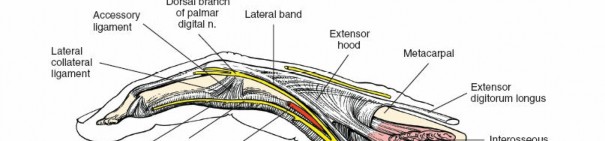
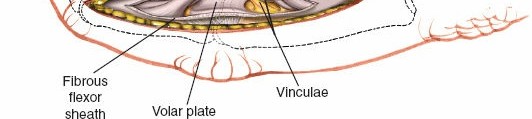
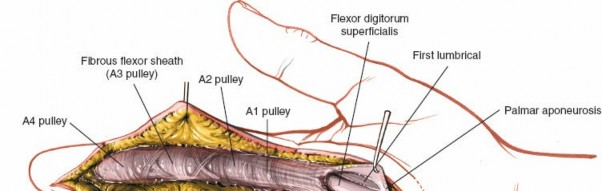
Within the fibro-osseous tunnel, these tendons are enveloped by a synovial sheath that facilitates smooth gliding and nutrition. The integrity of the pulley system, composed of annular (A) and cruciate (C) ligaments, is critical for preventing tendon bowstringing and maintaining efficient mechanical advantage. Typically, five annular pulleys (A1-A5) and three cruciate pulleys (C1-C3) are described in each finger. The A1 pulley is at the metacarpophalangeal (MCP) joint level, A2 at the proximal phalanx, A3 at the proximal interphalangeal (PIP) joint, A4 at the middle phalanx, and A5 at the distal interphalangeal (DIP) joint. The A2 and A4 pulleys are considered the most critical for preventing significant bowstringing.
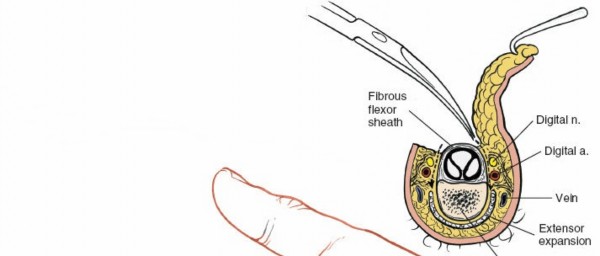
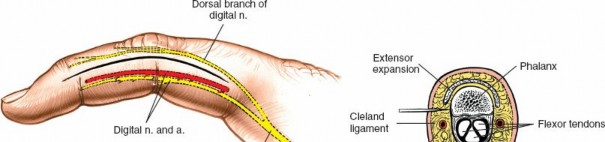
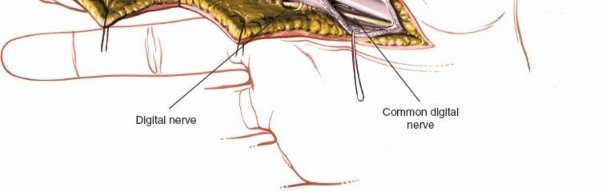
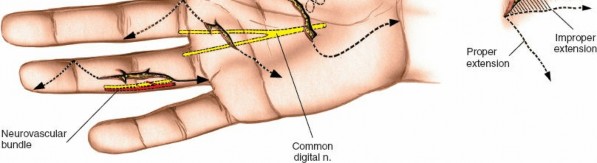
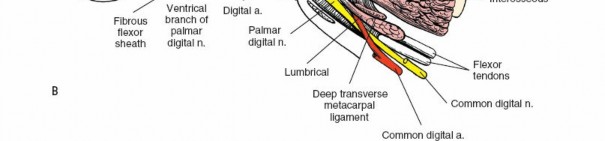
The digital neurovascular bundles (NVBs) run along the radial and ulnar sides of each digit, volar to the collateral ligaments, providing sensation and vascularity. Proper identification and protection of these bundles are paramount during any volar dissection. Proximally, the median nerve gives rise to recurrent motor branches to the thenar muscles and sensory branches to the thumb, index, middle, and radial half of the ring finger. The ulnar nerve supplies the hypothenar muscles, adductor pollicis, and interossei, along with sensory innervation to the little finger and ulnar half of the ring finger. The palmar arches (superficial and deep) provide critical vascular supply to the hand.

The palmar fascia, located superficial to the flexor tendons in the palm, is a dense aponeurosis important in conditions like Dupuytren's contracture. This fascial layer can obscure deeper structures and must be carefully managed during deep palmar dissection. The thenar and hypothenar eminences, as well as the transverse palmar crease, serve as important surface landmarks for guiding incisions and identifying underlying structures. The vincula tendinum (longus and brevis) are mesotenon-like structures that provide vascular supply to the flexor tendons within the sheath, and their preservation, where possible, is beneficial.
Biomechanical principles emphasize the importance of smooth tendon gliding, which is facilitated by an intact synovial sheath and a functional pulley system. Injury or scarring can impair gliding, leading to adhesions and reduced range of motion. The strength and integrity of the tendon repair are critical to withstand early mobilization protocols, which are now standard for optimized outcomes.
Indications & Contraindications
The volar approach provides the most comprehensive exposure to the flexor tendons within their fibrous sheaths, offering excellent visibility of both neurovascular bundles in the finger and allowing for extensions into the palm, wrist, and forearm as dictated by the pathology. This makes it a versatile approach in trauma, where multiple levels of exposure may be required, and allows incorporation of existing lacerations into the surgical incision, optimizing wound healing and cosmesis.
Indications for the Volar Approach:
- Exploration and Repair of Flexor Tendons: This includes primary repair of acute lacerations (Zones I-V), delayed primary repair, and secondary reconstruction (e.g., staged tendon reconstruction with silicone rods, or tenolysis for adhesions).
- Exploration and Repair of Digital Nerves and Vessels: Lacerations or compressions of digital nerves and arteries frequently accompany flexor tendon injuries. The volar approach facilitates direct visualization and microsurgical repair.
- Exposure of the Fibrous Flexor Sheath for Drainage of Pus: In cases of pyogenic flexor tenosynovitis, surgical incision and drainage are critical to prevent tendon necrosis and osteomyelitis. The volar approach allows thorough irrigation and debridement of the sheath.
- Excision of Tumors within the Fibrous Flexor Sheath: Common pathologies include giant cell tumors of the tendon sheath or ganglion cysts, which require complete excision for cure.
- Excision of Palmar Fascia in Dupuytren Contracture: Fasciectomy procedures (limited, regional, or total) are performed via volar incisions to address contractures of the palmar and digital fascia.
- Flexor Tendon Tenolysis: To address adhesions limiting tendon gliding after prior injury or repair.
- Flexor Tendon Transfers: To restore lost function by rerouting healthy tendons.
- Foreign Body Removal: Extraction of foreign bodies lodged within the flexor sheath or adjacent soft tissues.
- Vascular Revascularization/Replantation: While often requiring multiple approaches, the volar approach is crucial for accessing digital vessels.
Contraindications:
- Severe Soft Tissue Compromise: Extensive skin loss or severe devitalization may necessitate alternative approaches (e.g., dorsal approach with skin grafting if volar access is compromised) or deferral until soft tissue coverage is achieved.
- Active Infection (Relative): While tenosynovitis is an indication, surrounding cellulitis or abscess not involving the sheath may warrant initial non-operative management (antibiotics) or incision and drainage at a different site.
- Severe Systemic Comorbidities: Patients with significant medical comorbidities precluding safe anesthesia and surgical intervention.
- Irreparable Damage: In instances of severe crush injury or avulsion with extensive tissue loss where primary repair is not feasible, the volar approach may be used for debridement prior to secondary reconstructive procedures.
Table: Operative vs. Non-Operative Indications for Flexor Tendon Pathology
| Condition | Typical Management Approach | Notes |
|---|---|---|
| Acute Flexor Tendon Laceration | Operative: Primary repair via volar approach | Gold standard for restoring function. |
| Pyogenic Flexor Tenosynovitis | Operative: Incision and drainage of flexor sheath via volar approach | Emergent surgical intervention required. |
| Digital Nerve Laceration | Operative: Microsurgical repair via volar approach | Essential for sensory and motor recovery. |
| Digital Artery Laceration | Operative: Microsurgical repair/ligation via volar approach | Revascularization critical for digital viability. |
| Giant Cell Tumor of Tendon Sheath | Operative: Excision via volar approach | Complete excision to prevent recurrence. |
| Dupuytren Contracture (contracted cord) | Operative: Fasciectomy (limited, regional, total) via volar approach | Addresses contracture, improves extension. |
| Flexor Tenosynovitis (non-infectious) | Non-Operative (initial): Rest, NSAIDs, steroid injection; Operative: Synovectomy/A1 pulley release via volar approach | Trigger finger/stenosing tenosynovitis often requires A1 pulley release. |
| Tendon Adhesions Post-Injury | Non-Operative (initial): Hand therapy; Operative: Tenolysis via volar approach | Failed conservative management or significant functional deficit. |
| Chronic Tendinopathy (non-ruptured) | Non-Operative: Rest, physical therapy, activity modification, NSAIDs | Surgical intervention rare unless significant degenerative changes or rupture. |
| Minor Contusions/Sprains | Non-Operative: RICE, analgesia, early mobilization | No structural damage requiring surgical intervention. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial for optimizing outcomes and anticipating potential challenges. This includes a thorough patient history, physical examination focusing on neurovascular status, hand dominance, previous injuries, and functional demands. Imaging studies such as radiographs (to rule out associated fractures), ultrasound (for dynamic assessment of tendon integrity and retraction), or MRI (for chronic or complex cases) may be indicated.
Anesthesia: The choice of anesthesia depends on patient factors, surgeon preference, and the extent of the procedure. Regional anesthesia (e.g., axillary, supraclavicular block) offers excellent intraoperative analgesia and can provide post-operative pain control, minimizing systemic opioid use. Local anesthesia with or without sedation is an option for more localized procedures, though care must be taken with digital blocks that include epinephrine, especially in digital tip procedures, due to theoretical risk of vasoconstriction. General anesthesia may be preferred for longer, more complex cases or anxious patients.
Patient Positioning:
The patient is typically placed supine on the operating table. The affected arm is abducted approximately 90 degrees and positioned on an arm board, allowing for free movement and access.

The height of the operating table should be adjusted to allow the surgeon to sit comfortably with good ergonomic posture. Most right-handed surgeons prefer to sit on the ulnar side of the affected arm, providing optimal visualization and instrument control for procedures on the radial aspect of the hand and fingers, and vice versa for the left hand or left-handed surgeons.

Tourniquet and Lighting: An exsanguinating bandage (e.g., Esmarch bandage) is applied from distal to proximal to achieve a bloodless field, followed by inflation of a pneumatic tourniquet on the upper arm to a pressure of 250-300 mmHg, or 100 mmHg above systolic pressure. For digital procedures, a small digital tourniquet can be used. A bloodless field is absolutely essential for precise dissection and microsurgical repair. Excellent lighting, often augmented by loupe magnification (typically 2.5x to 4.5x) or an operating microscope, is paramount for identifying delicate structures like digital nerves and vessels and for meticulous tendon repair.
Sterile preparation and draping of the entire upper extremity, from the shoulder to the fingertips, allows for maximum flexibility in manipulating the hand and wrist.
Detailed Surgical Approach / Technique
The volar approach necessitates meticulous attention to anatomical landmarks and careful dissection to optimize exposure while preserving vital neurovascular structures.
Landmarks and Incision
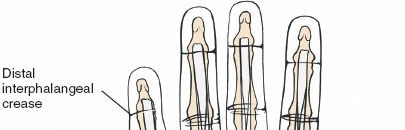
Surface landmarks guide the incision. In the digits, these include the distal phalangeal crease (just proximal to the distal interphalangeal joint), the proximal interphalangeal crease, and the metacarpophalangeal crease. In the palm, the distal palmar crease and thenar/hypothenar creases are important.
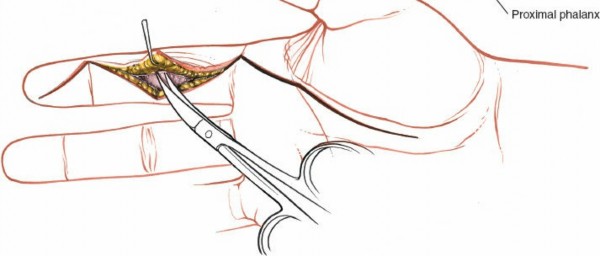
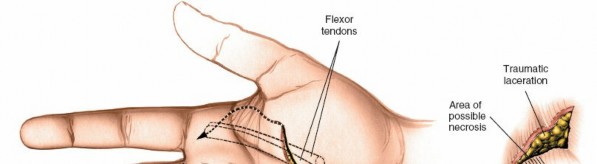
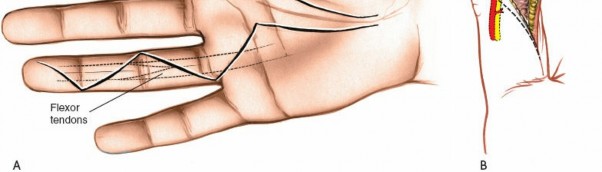
The skin incision must provide adequate exposure without creating straight lines across joint creases, which can lead to scar contracture. The Bruner zigzag incision is the standard for digital access due to its excellent exposure and prevention of flexion contractures. It incorporates the natural creases and extends proximally and distally in a zigzag fashion along the length of the digit. The apices of the V's are typically located over the mobile skin of the phalanges, avoiding the fixed skin over the joint creases.

- Finger Incision (Bruner): Begins dorsally/mid-laterally over the distal phalanx, angles volarly, crosses the volar skin crease, then angles back to the mid-lateral line, avoiding straight lines across joints. This allows creation of triangular skin flaps.
- Palmar Incision: Can be made as a curvilinear extension from the digital Bruner incision, often curving towards the thenar or hypothenar eminence, or as a transverse incision in line with the distal palmar crease. Incorporating a laceration directly into the incision is always preferred to minimize additional skin damage.
- Wrist Incision: Often a longitudinal incision along the course of the flexor carpi radialis or ulnaris tendons, curving slightly to avoid crossing the wrist crease at a right angle.
Skin and Subcutaneous Dissection
After marking the incision, the skin and subcutaneous tissues are carefully incised. In the digits, the triangular skin flaps created by the Bruner incision are elevated using fine skin hooks or small self-retaining retractors. Dissection should proceed in the subcutaneous plane, superficial to the digital neurovascular bundles, which run along the radial and ulnar borders of the digit, immediately adjacent to the flexor sheath.

Care must be taken to identify and protect these bundles. Any existing lacerations or hematomas are debrided. The digital nerves and vessels are carefully dissected free from the surrounding connective tissue and retracted, typically dorsally and laterally, using vessel loops or fine retractors to provide clear access to the underlying flexor sheath.
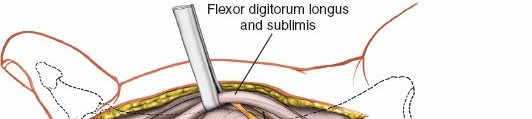
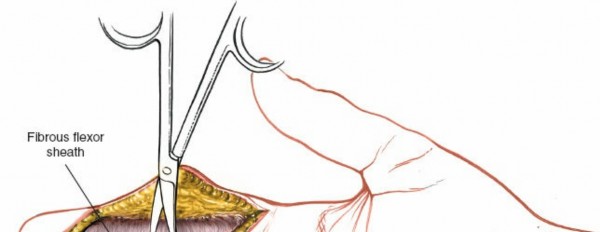
Fibrous Flexor Sheath Exposure
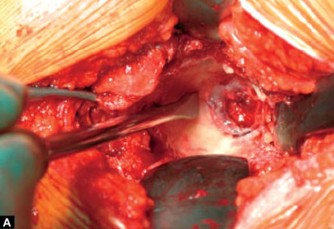
Once the subcutaneous tissue and neurovascular bundles are retracted, the fibrous flexor sheath is visible. This appears as a glistening white, tough structure enveloping the flexor tendons.
The sheath is incised longitudinally. The specific pulleys that need to be released depend on the pathology and zone of injury.
- A1 Pulley Release: For distal palmar or MCP joint access (e.g., trigger finger release, A1 pulley excision for tumor). The A1 pulley can be completely incised longitudinally from proximal to distal without significant risk of bowstringing, as the A2 pulley is the primary stabilizer at the proximal phalanx base.
-
Digital Pulleys (A2-A5, C1-C3):
- For flexor tendon repair, typically the A2 and A4 pulleys must be preserved to prevent bowstringing, which significantly impairs mechanical efficiency.
- The A1, A3, and A5 pulleys, and the cruciate pulleys (C1, C2, C3), can be incised longitudinally or partially vented to expose the tendons and allow for repair.
- When accessing Zone II (no-man's land), the incision usually involves opening the A1, A3, and C1/C2/C3 pulleys, carefully preserving the A2 and A4 pulleys.
- In cases of extensive trauma or adhesions, careful piecemeal division of pulleys may be necessary to gain adequate exposure for repair or tenolysis, with a plan for potential pulley reconstruction if significant bowstringing is anticipated.
Tendon Management
Once the flexor sheath is opened, the FDS and FDP tendons are exposed.
-
Locating Tendon Ends:
In acute lacerations, retracted tendon ends can be challenging to locate. The proximal end may retract significantly into the palm or forearm due to muscle contraction. Techniques to retrieve retracted ends include:
- Milking the forearm muscles proximally.
- Using a small curved hemostat or a tendon retriever.
- Making a more proximal incision (e.g., in the forearm) to pull the tendon distally into the wound.
- Passive wrist and finger extension may bring the proximal stump distally.
- Note the FDS will often retract more than the FDP in the finger if both are cut due to the attachment of FDS in the mid-phalanx.
- Debridement and Preparation: The tendon ends are gently debrided of any frayed or necrotic tissue, ensuring clean, healthy margins for repair. The synovial sheath is preserved where possible.
-
Tendon Repair Techniques:
-
Core Sutures:
The primary repair involves core sutures to provide strength. Common techniques include:
- Modified Kessler: A two-strand repair that is strong but can leave a bulky knot.
- Pennington (Lim-Tsai) or Double-Kessler: Multi-strand repairs (4-strand, 6-strand) that offer superior strength and allow for earlier active mobilization protocols. These involve placing multiple strands longitudinally within the tendon substance.
- Various other techniques exist, aiming for maximum repair strength with minimal bulk.
- Epitendinous Sutures: After core sutures, an epitendinous suture (e.g., running horizontal mattress) is applied to coapt the tendon edges and provide a smooth gliding surface. This also adds approximately 10-20% to the repair strength.
-
Core Sutures:
The primary repair involves core sutures to provide strength. Common techniques include:
- Order of Repair: In the presence of both FDS and FDP injury, the FDP is typically repaired first, followed by the FDS. The FDS may be partially or completely excised if it significantly obstructs the FDP repair, but preservation is preferred.
- Tension: The repair should be performed with appropriate tension, mimicking physiological tension, to allow full range of motion without excessive gapping or undue tension on the repair site.
Neurovascular Bundle Management
If digital nerves or vessels are lacerated, they are repaired after tendon repair or at a separate stage depending on the complexity.
- Nerve Repair: Digital nerves are repaired primarily using microsurgical techniques (e.g., epineurial repair) with fine monofilament sutures (e.g., 8-0 to 10-0 nylon) under magnification. Tension-free repair is paramount.
- Vascular Repair: Digital arteries can be repaired with microsurgical techniques using fine sutures (e.g., 9-0 or 10-0 nylon). Ligation may be necessary if repair is not feasible, provided the contralateral digital artery provides adequate perfusion.
Specific Considerations
- Infection Drainage: For pyogenic flexor tenosynovitis, the sheath is incised longitudinally along its entire length, and thorough irrigation with saline solution is performed. Tissue samples are sent for culture.
- Tumor Excision: Tumors within the sheath are carefully dissected free from the surrounding tendons and neurovascular structures, ensuring clear margins.
- Dupuytren's Fasciectomy: The specific cords of contracted fascia are identified and excised (limited, regional, or total fasciectomy), taking care to avoid injury to the underlying neurovascular bundles and flexor tendons.
- Tenolysis: This involves carefully dissecting adhesions from the tendon surface and the surrounding sheath, restoring tendon gliding. This often requires the use of magnification and specialized instruments.
Wound Closure
After all repairs are complete, the tourniquet is deflated, and meticulous hemostasis is achieved. The wound is copiously irrigated. The flexor sheath is typically left open or partially closed, especially in the digits, to avoid compromising tendon gliding. The skin flaps are carefully reapproximated using fine interrupted sutures (e.g., 5-0 or 6-0 nylon), ensuring no tension.
A sterile dressing is applied, followed by a protective splint. For flexor tendon repairs, a dorsal block splint is universally used to hold the wrist in slight flexion and the MCP joints in 30-70 degrees of flexion, allowing full extension of the IP joints while protecting the repair from excessive tension during early motion.


Complications & Management
Despite meticulous surgical technique, complications can occur following a volar approach to flexor tendons. Early recognition and appropriate management are critical for optimizing patient outcomes.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approximate) | Salvage Strategies |
|---|---|---|
| Tendon Adhesions | 30-50% (variable) | Non-operative: Intensive hand therapy, dynamic splinting, mobilization exercises. Operative: Flexor tenolysis (surgical release of adhesions) with or without adjunctive measures (e.g., anti-adhesion barriers, early active motion). May require repeat surgery. |
| Tendon Rupture | 5-15% | Acute: Primary revision repair if viable. Delayed/Chronic: Staged tendon reconstruction with silicone rod followed by tendon grafting (e.g., palmaris longus, FDS side slip), or tendon transfer if sufficient motor units available. |
| Infection | 1-5% | Superficial: Oral antibiotics, local wound care. Deep (tenosynovitis, osteomyelitis): Surgical incision and drainage, extensive debridement, intravenous antibiotics, wound culture-directed therapy. May necessitate implant removal if applicable. |
| Digital Nerve Injury/Neuroma | 5-10% (transient/minor) | Acute iatrogenic injury: Immediate microsurgical repair (epineurial). Neuroma-in-continuity: Neurolysis. Painful terminal neuroma: Excision and nerve grafting, nerve transfer, nerve cap, targeted muscle reinnervation. Sensory deficit: Hand therapy, sensory re-education. |
| Vascular Compromise/Ischemia | <1% | Acute: Immediate exploration, microsurgical repair of digital artery, or vein graft interposition. If secondary to external compression, release pressure. Long-term: May require complex microvascular reconstruction or result in tissue loss requiring amputation or debridement. |
| Pulley Insufficiency/Bowstringing | 5-10% | Mild: No specific treatment, functional compensation. Moderate-Severe: Pulley reconstruction (e.g., using extensor retinaculum, palmaris longus graft, plantaris tendon, or artificial materials) to restore biomechanical efficiency. Timing is usually secondary after tendon healing. |
| Joint Contracture | 10-20% | Non-operative: Aggressive hand therapy, static and dynamic splinting, serial casting, joint mobilization techniques. Operative: Capsulectomy, arthrolysis, tenolysis if associated with adhesions. May require secondary reconstruction if severe and refractory. |
| Pain/Complex Regional Pain Syndrome (CRPS) | 1-5% (CRPS) | Pain: Analgesics, physical therapy, psychological support. CRPS: Multidisciplinary approach involving pharmacotherapy (neuropathic agents, corticosteroids), physical and occupational therapy, sympathetic nerve blocks, spinal cord stimulators, psychological counseling. Early diagnosis and aggressive treatment are crucial. |
| Scar Sensitivity/Hypersensitivity | Common | Non-operative: Desensitization therapy, massage, silicone gel sheeting, compression garments. Surgical intervention is rarely indicated unless a specific painful neuroma is identified. |
| Flap Necrosis/Wound Dehiscence | 1-3% | Minor: Local wound care, secondary intention healing. Major: Debridement, secondary closure, local or regional flap coverage (e.g., cross-finger flap, thenar flap) for soft tissue reconstruction. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as the surgical repair itself, dictating the ultimate functional outcome. Modern protocols emphasize early, controlled motion to promote tendon gliding, reduce adhesion formation, and improve strength, while protecting the integrity of the repair. The guidance of a certified hand therapist (CHT) is indispensable.
General Principles:
- Protection: The repair site must be protected from excessive tensile forces that could lead to gapping or rupture.
- Controlled Motion: Early, controlled movement helps to prevent adhesions and nourish the tendon.
- Gradual Progression: Rehabilitation progresses systematically from passive to active motion, and then to strengthening and functional activities.
Phased Approach (Commonly Used Protocols like Duran or Kleinert):
Phase I: Immediate Post-Operative (Weeks 0-3)
-
Splinting:
A dorsal block splint (wrist flexed 20-30°, MCPs flexed 30-70°, IP joints fully extended or nearly so) is applied immediately post-op. This allows full passive IP joint flexion but blocks active extension, preventing excessive tension on the repair.

-
Motion:
- Duran Protocol (Passive Motion): Within the splint, the patient performs specific passive flexion exercises to the FDS and FDP tendons, moving the DIP and PIP joints through their full passive range of motion with the other joints stabilized. Typically 10 repetitions per hour.
-
Kleinert Protocol (Dynamic Traction):
Elastic bands are attached to the fingernails and secured to the forearm portion of the splint, providing passive flexion. Active extension is performed against the resistance of the bands, followed by passive flexion back into the splint.

- Wound Care: Regular dressing changes, monitoring for infection.
- Patient Education: Crucial for compliance and understanding limitations.
Phase II: Early Active Motion (Weeks 3-6)
- Splint Modification: The dorsal block splint may be adjusted or a new splint fabricated to allow greater range of motion as tolerated.
- Motion: Gradual initiation of gentle active flexion and extension exercises, initially with the wrist in flexion to minimize tension. Progression to full active ROM as tolerated, emphasizing differential gliding of FDS and FDP.
- Scar Management: Gentle massage, silicone gel sheets, and desensitization exercises for scar management.
- Light Functional Activities: Begin very light activities of daily living, avoiding firm grasp or resistance.
Phase III: Intermediate Strengthening (Weeks 6-12)
- Discontinue Splint: The splint is typically discontinued around 6-8 weeks, depending on repair strength and surgeon preference.
- Strengthening: Gradual introduction of progressive resistive exercises using theraputty, resistance bands, or light weights.
- Advanced Motion: Continued emphasis on full range of motion.
- Activity Progression: Gradual return to more demanding functional tasks and work-related activities.
Phase IV: Return to Activity (Weeks 12+)
- Full Strength and Endurance: Focus on maximizing strength, endurance, and coordination.
- Sport/Work-Specific Training: Tailored exercises to facilitate return to high-demand sports or occupations.
-
Monitoring:
Continued monitoring for adhesions, contractures, or other complications. Full recovery can take 6 months to a year.
Summary of Key Literature / Guidelines
The management of flexor tendon injuries and other pathologies requiring volar access has evolved significantly over decades, driven by advancements in surgical technique, materials science, and rehabilitation protocols. Key literature and guidelines underpin current best practices:
- Repair Strength: Numerous studies have demonstrated that multi-strand repairs (4-strand to 6-strand) using techniques like modified Kessler, Pennington, or similar patterns provide significantly greater tensile strength than traditional two-strand repairs. This increased strength is critical for enabling early active motion protocols, which are now standard. Biomechanical studies continue to refine optimal suture configuration and material selection to minimize gap formation and maximize repair integrity.
- Pulley Management: The consensus emphasizes the critical importance of preserving the A2 and A4 pulleys in the digits to prevent functional bowstringing. Division of A1, A3, and A5, and the cruciate pulleys, is generally well-tolerated and often necessary for adequate exposure and debridement. In situations where A2 or A4 must be sacrificed, elective pulley reconstruction at a later stage may be considered using tendon grafts (e.g., palmaris longus) or fascia.
- Early Active Motion (EAM): The paradigm shift from immobilization to early, controlled motion, pioneered by protocols like Duran and Kleinert, is supported by extensive evidence. EAM significantly reduces adhesion formation, promotes better tendon gliding, and leads to superior functional outcomes compared to prolonged immobilization. The specific protocol (passive, active, or dynamic) chosen depends on the surgeon's preference, repair strength, patient compliance, and the availability of hand therapy.
- Zone-Specific Management: While the volar approach is ubiquitous, treatment strategies are often zone-specific. Zone II ("no man's land") injuries, historically associated with poorer outcomes due to complex anatomy and adhesion formation, have seen improved results with modern multi-strand repairs and EAM. Zone I injuries (FDP avulsion) often require reinsertion of the tendon to the distal phalanx. Zone III (palmar) and Zone IV (carpal tunnel) injuries have distinct considerations due to the confluence of tendons and major neurovascular structures.
- Adhesion Prevention: Research continues into various methods for preventing adhesions, including tenosynovectomy, pharmacological agents (e.g., corticosteroids, hyaluronic acid), and physical barriers. While some show promise, none have definitively eliminated the problem. Meticulous surgical technique and early motion remain the most effective strategies.
- Infection and Tenosynovitis: Clinical guidelines consistently advocate for urgent surgical incision and drainage for pyogenic flexor tenosynovitis, emphasizing the "four cardinal signs" of Kanavel. Prompt diagnosis and treatment are crucial to prevent devastating consequences such as tendon necrosis and spread of infection.
- Dupuytren's Disease: Surgical excision of pathological cords (fasciectomy) remains the gold standard for established Dupuytren's contractures causing functional impairment. Newer modalities like collagenase injection offer a non-surgical alternative for select cases but do not negate the need for surgical expertise for more advanced or recurrent disease.
In conclusion, the volar approach to flexor tendons is a highly effective and versatile technique. Mastery of the underlying anatomy, adherence to meticulous surgical principles, diligent post-operative rehabilitation, and a comprehensive understanding of current literature and guidelines are all essential for achieving optimal outcomes for patients with pathologies of the flexor tendon system.
Clinical & Radiographic Imaging
You Might Also Like