Surgical Treatment of Acute and Chronic Paronychia and Felons

Introduction & Epidemiology
Acute paronychia, defined as an infection of the soft tissue fold surrounding the nail plate, represents the most prevalent soft tissue infection encountered in the hand. The pathogenesis typically involves a breach in the eponychial seal, allowing bacterial ingress. The vast majority of cases are attributable to Staphylococcus aureus , often in conjunction with other organisms, indicative of a polymicrobial etiology. Risk factors include trauma, nail-biting (onychophagia), cuticle manipulation, and exposure to irritants. Untreated or inadequately managed acute paronychia can progress to a subungual abscess or osteomyelitis of the distal phalanx.
Chronic paronychia, in contrast, is characterized by recurrent inflammation and infection of the eponychium, leading to thickening and rounding of the nail fold. This condition is frequently observed in individuals with occupations involving prolonged or repeated water exposure, such as dishwashers, bartenders, and healthcare professionals. The microbial flora implicated in chronic paronychia is diverse, commonly encompassing Candida albicans , various gram-positive cocci, gram-negative rods, and occasionally Mycobacterium species. Immunocompromised states, diabetes mellitus, and dermatological conditions like psoriasis can predispose individuals to chronic paronychia.
Herpetic whitlow, caused by the herpes simplex virus (HSV), presents as painful vesicles on an erythematous base, often mimicking acute paronychia or a felon. Its recognition is critical as surgical incision and drainage (I&D) is contraindicated and can exacerbate the viral infection. Herpetic whitlow is more common in children due to thumb-sucking and in medical personnel who handle oral secretions.
A felon is a deep, tense abscess within the distal pulp space of a digit, involving the multiple fibrous septa that compartmentalize the pulp. These septa extend from the periosteum of the distal phalanx to the skin, creating confined spaces that, when infected, lead to significant pressure, pain, and potential compromise of local vascularity. The most common causative organism is also
Staphylococcus aureus
, typically introduced through a penetrating injury. If left untreated, a felon can lead to osteomyelitis of the distal phalanx, tenosynovitis, or septic arthritis. Early and accurate diagnosis, coupled with appropriate intervention, is paramount to preserving digit function and preventing irreversible sequelae.
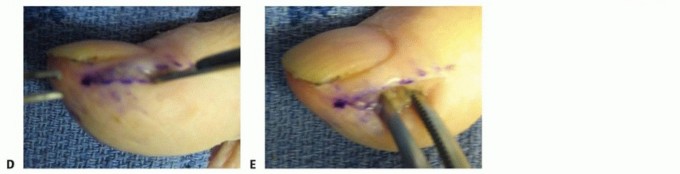
Figure 1: Clinical presentation of a Felon, demonstrating significant swelling and erythema of the fingertip pulp.
Surgical Anatomy & Biomechanics
A comprehensive understanding of the anatomy of the nail unit and fingertip pulp is fundamental for the surgical management of paronychia and felons. The nail unit comprises several critical structures:
*
Nail Plate:
The visible keratinized structure.
*
Nail Bed:
Composed of the sterile matrix (distal) and germinal matrix (proximal), responsible for nail growth.
*
Eponychium (Proximal Nail Fold):
The skin fold covering the proximal nail plate, forming a protective seal.
*
Paronychium (Lateral Nail Folds):
The skin folds along the lateral margins of the nail plate, also contributing to the protective seal.
*
Hyponychium:
The tissue beneath the free edge of the nail plate, forming another protective seal.
*
Distal Phalanx:
The underlying bone, which can be affected by deep infections.
The protective seals formed by the eponychium and paronychium are crucial barriers against microbial invasion. Disruption of these seals, whether traumatic or chronic, is the primary entry point for pathogens in paronychia. The nail matrix, particularly the germinal matrix, is highly susceptible to damage from infection or surgical trauma, leading to permanent nail dystrophy.
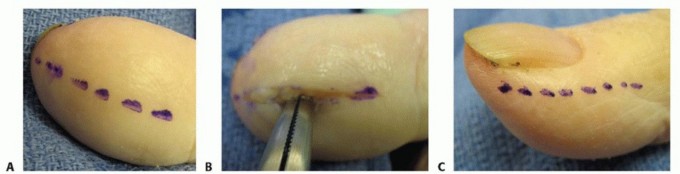
Figure 2: Detailed anatomical representation of the nail unit, highlighting the eponychium, paronychium, and underlying matrix.
The fingertip pulp, relevant to felons, is a unique soft tissue structure. It is richly vascularized and innervated, providing tactile sensation and aiding grip. Characteristically, the pulp space is divided into numerous small, vertically oriented fibrous septa that extend from the dermis to the periosteum of the distal phalanx. These septa provide structural support but also create a compartmentalized space. When infection occurs within this space, the inflammatory exudate and pus are confined, leading to rapidly escalating pressure, intense pain, and potential compromise of the local microcirculation. This increased pressure can lead to local tissue necrosis and direct pressure erosion of the distal phalanx, resulting in osteomyelitis.
Vascular supply to the digits is primarily via the paired digital arteries, running along the dorsolateral aspects of the fingers, anterior to the digital nerves. Surgical incisions must respect these structures to prevent iatrogenic ischemia or nerve damage. The digital nerves provide sensation to the fingertip, making careful dissection essential. The lymphatic drainage of the digits can transmit infection proximally, leading to lymphangitis or epitrochlear lymphadenopathy.
Figure 3: Cross-sectional anatomy of the fingertip, illustrating the fibrous septa within the pulp space and the position of neurovascular bundles.
Biomechanically, the nail plate provides support and protection to the fingertip. Damage to the germinal matrix can result in a deformed nail plate, affecting both aesthetics and function. The fibrous septa of the pulp, while protective, are detrimental in the context of infection due to their compartmentalizing effect. Surgical intervention for a felon aims to decompress these compartments effectively while preserving critical neurovascular structures and the integrity of the fingertip's biomechanical properties.
Indications & Contraindications
Indications for Surgical Intervention
Surgical intervention for paronychia and felons is primarily indicated when conservative measures fail, or when a localized abscess has formed requiring drainage and debridement.
Acute Paronychia:
*
Fluctuant abscess:
Any palpable collection of pus within the nail fold.
*
Subungual abscess:
Pus extending beneath the nail plate, often visible as a yellowish discoloration through the nail.
*
Progressive infection:
Spreading cellulitis, lymphangitis, or signs of systemic involvement despite oral antibiotics.
*
Failure of conservative treatment:
Persistence of pain, erythema, and swelling after 24-48 hours of warm soaks and oral antibiotics for early, non-fluctuant cases.
Chronic Paronychia:
*
Persistent inflammation and hypertrophic changes:
Failed medical management with topical antifungals/steroids, leading to significant thickening of the eponychium.
*
Recurrent acute exacerbations:
Frequent episodes of acute infection superimposed on chronic inflammation.
*
Subungual granuloma or abscess:
Indications for nail plate removal and debridement.
*
Significant nail dystrophy:
Caused by chronic inflammation affecting the nail matrix.
Felon:
*
Any palpable fluctuant abscess:
This is the primary indication, as felons are deep, tense infections that rarely resolve with antibiotics alone.
*
Progressive pain and swelling:
Increasing pressure within the pulp space.
*
Signs of impending necrosis or osteomyelitis:
Severe tenderness, dusky discoloration of the skin, or radiographic evidence of bone involvement.
*
Failure of conservative treatment:
For very early, non-fluctuant cases (rarely effective).
Contraindications for Surgical Intervention
Specific contraindications must be recognized to prevent iatrogenic complications or inappropriate treatment.
- Herpetic Whitlow: This is an absolute contraindication for incision and drainage. Surgical intervention can lead to viral dissemination, superinfection, prolonged healing, and potential for recurrent outbreaks. Diagnosis is often clinical (vesicles on an erythematous base, grouped lesions, patient history) but can be confirmed with Tzanck smear or viral culture.
- Cellulitis without abscess formation: In early stages of infection, particularly in acute paronychia or mild cellulitis surrounding a felon, oral antibiotics and warm soaks may be sufficient. Surgical I&D in the absence of a drainable collection is not beneficial and can introduce bacteria into deeper tissues.
- Severe coagulopathy: Relative contraindication, requiring careful assessment and correction of coagulopathy prior to surgery.
- Poor general health/uncontrolled systemic disease: Relative contraindication, requiring optimization of patient's medical status before elective or semi-elective procedures.
Operative vs. Non-Operative Indications
| Condition | Non-Operative Indications | Operative Indications |
|---|---|---|
| Acute Paronychia | Early erythema, mild swelling, no fluctuance. | Fluctuant abscess, subungual pus, failure of conservative care. |
| Chronic Paronychia | Mild inflammation, no hypertrophic changes, limited water exposure. | Persistent hypertrophic eponychium, recurrent acute episodes, subungual pathology. |
| Felon | Extremely early onset, minimal swelling, no fluctuance (rare). | Any palpable fluctuance, severe pain, signs of impending tissue necrosis, osteomyelitis. |
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning is essential to ensure a successful outcome and minimize complications.
Diagnostic Evaluation
- History: Detailed history including duration of symptoms, preceding trauma, presence of comorbidities (e.g., diabetes, immunosuppression), prior treatments (antibiotics, topical agents), and occupational/recreational exposures (e.g., water immersion, chemicals).
-
Physical Examination:
- Inspection: Assess erythema, swelling, warmth, fluctuance, nail plate discoloration, and presence of vesicles (to rule out herpetic whitlow). Evaluate for signs of proximal spread (lymphangitis, lymphadenopathy).
- Palpation: Gently palpate the affected area to identify fluctuance, delineate the extent of the abscess, and assess tenderness. For felons, note the tenseness of the pulp space.
- Neurovascular Status: Assess digital capillary refill and sensation.
-
Imaging:
- Radiographs (AP, lateral, oblique views of the digit): Routinely indicated for felons and chronic paronychia to rule out underlying osteomyelitis of the distal phalanx. May also reveal foreign bodies. Not typically necessary for acute paronychia unless infection is severe or prolonged.
- Ultrasound: Can be helpful in discerning between cellulitis and abscess, particularly in atypical presentations or for guiding drainage.
-
Laboratory Studies:
- Culture: Obtain intraoperative cultures of pus or tissue for Gram stain, aerobic and anaerobic cultures, and fungal cultures (especially for chronic paronychia).
- Blood work: Complete blood count (CBC) to assess leukocytosis; C-reactive protein (CRP) and Erythrocyte Sedimentation Rate (ESR) may be elevated in more severe or chronic infections.
Anesthesia
- Digital Block: The most common and preferred method. A local anesthetic such as 1% lidocaine (without epinephrine) is infiltrated circumferentially around the base of the affected digit, ensuring complete blockade of the digital nerves. Avoid epinephrine due to risk of digital ischemia.
- Wrist Block: May be used for more extensive infections or when a digital block is technically challenging.
- Regional Anesthesia (Axillary Block): Indicated for complex cases, patients unable to tolerate local anesthesia, or procedures involving multiple digits.
- General Anesthesia: Rarely required for these procedures but may be considered for pediatric patients or highly anxious adults.
Tourniquet Application
A bloodless field is crucial for precise surgical dissection and adequate visualization of the abscess and neurovascular structures.
*
Digital Tourniquet:
A sterile Penrose drain, a rolled finger cot, or a dedicated digital tourniquet can be applied at the base of the digit. Ensure the tourniquet time is recorded and limited (typically <20 minutes).
Patient Positioning and Preparation
- Patient Position: Supine on the operating table. The affected arm should be placed on a dedicated hand table.
- Surgical Prep: The hand and distal forearm are prepped and draped in a sterile fashion using an antiseptic solution (e.g., povidone-iodine or chlorhexidine).
- Instrumentation: Standard hand surgery tray including a No. 11 or 15 scalpel blade, fine dissecting scissors, mosquito hemostats, small curette, blunt probe, irrigation syringe with saline, and non-adherent dressing material.
Detailed Surgical Approach / Technique
The primary goals of surgical intervention are to adequately drain the purulent collection, debride necrotic tissue, obtain cultures, and preserve the vital structures of the digit, particularly the nail matrix and neurovascular bundles.
Acute Paronychia
The surgical approach for acute paronychia depends on the extent and location of the pus.

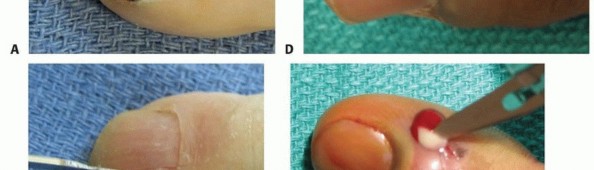
Figure 4: Acute paronychia with significant swelling and pus evident beneath the eponychial fold.
- Early, Non-fluctuant: If there is erythema and swelling but no obvious fluctuance, elevation of the eponychial fold with a blunt instrument (e.g., small Freer elevator or the flat end of a No. 15 blade) can often release trapped pus. This is performed proximally, lifting the fold away from the nail plate.
-
Unilateral Fluctuant Abscess:
- Perform a digital block and apply a tourniquet.
- Make a small longitudinal incision (No. 11 blade) along the affected lateral nail fold, extending just distal to the eponychial fold (typically 3-5 mm). The incision should be parallel to the nail fold and away from the nail matrix.
- Carefully spread the tissues with a mosquito hemostat or blunt probe to open the abscess pocket.
- Drain the pus, obtain a culture, and irrigate thoroughly with saline.
-
A small piece of packing (e.g., gauze wick) can be placed to maintain drainage for 24-48 hours.
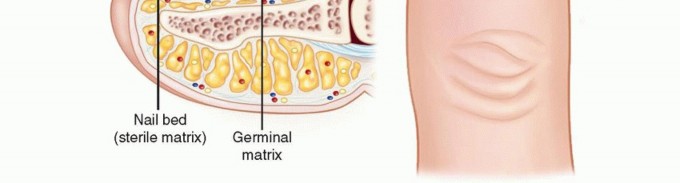
Figure 5: Incision and drainage of an acute paronychia, showing the release of pus from beneath the nail fold.
-
Bilateral Fluctuant Abscess (Collar-Button Abscess):
- If pus is present on both sides of the nail or tracking across the eponychial fold, bilateral longitudinal incisions may be necessary.
- Alternatively, a small transverse incision across the eponychial fold, just proximal to the nail plate, can connect the bilateral pockets, forming an inverted "U" incision. This should be performed cautiously to avoid damage to the nail matrix.
-
Subungual Abscess:
- If pus has tracked beneath the nail plate, a portion of the nail plate overlying the pus must be removed. This can be achieved by carefully dissecting the involved nail segment from the nail bed using a fine scissor or scalpel, then excising it.
-
Drainage and irrigation are performed, and the nail bed is inspected for granuloma formation or foreign bodies.

Figure 6: Partial nail plate avulsion for drainage of a subungual abscess associated with paronychia.
Chronic Paronychia
The goal of surgical treatment for chronic paronychia is to excise the chronically inflamed tissue, address any underlying pathology, and allow for reformation of a healthy eponychial seal.

Figure 7: Chronic paronychia with thickened eponychium and nail plate dystrophy.
-
Eponychial Marsupialization (Modified Atasoy/Kutler Flap Excision):
This is the gold standard for recalcitrant chronic paronychia.
- After digital block and tourniquet, make a crescentic incision along the proximal border of the eponychium, excising a portion of the hypertrophied eponychial fold. The width of excision depends on the degree of hypertrophy, typically 2-4 mm.
- The incision extends laterally to the base of the lateral nail folds.
- Carefully elevate the proximal flap, exposing the underlying nail matrix. Any granulomatous tissue or osteophytes affecting the matrix should be meticulously debrided.
- The proximal nail plate may be temporarily avulsed to allow better access for debridement of the germinal matrix area, especially if a subungual abscess or granuloma is present.
- The skin edges are not typically reapproximated; the wound is left open to granulate, which allows for drainage and reduces recurrence.
-
A non-adherent dressing is applied.
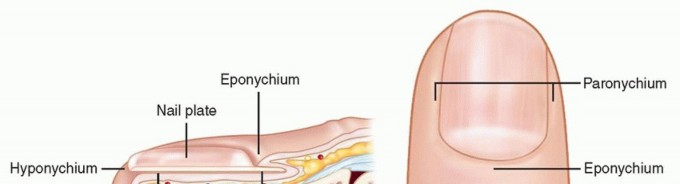
Figure 8: Surgical excision (marsupialization) of the eponychial fold in chronic paronychia.
Felon
Surgical drainage of a felon requires precise incision planning to adequately decompress the pulp space while protecting crucial neurovascular structures.

Figure 9: Clinical presentation of a felon, demonstrating significant tension and swelling of the distal pulp.
- Digital Block and Tourniquet: Essential for a bloodless field and adequate analgesia.
-
Incision Choices:
-
Unilateral Longitudinal Incision:
The preferred method. A longitudinal incision is made along the
mid-lateral aspect
of the digit, away from the volar pulp and the nail. The incision should be made on the side of maximal fluctuance. It extends from approximately the distal interphalangeal joint crease to just proximal to the nail fold.
-
Technique:
Incise the skin and subcutaneous tissue. Bluntly dissect into the pulp space, separating the fibrous septa to ensure complete drainage. Avoid incising too deeply towards the bone to prevent damage to the flexor tendon sheath or distal phalanx periosteum.

Figure 10: Unilateral longitudinal incision for felon drainage, made along the mid-lateral aspect of the digit.
-
Technique:
Incise the skin and subcutaneous tissue. Bluntly dissect into the pulp space, separating the fibrous septa to ensure complete drainage. Avoid incising too deeply towards the bone to prevent damage to the flexor tendon sheath or distal phalanx periosteum.
- Bilateral Longitudinal Incisions: Used for extensive felons involving the entire pulp. Incisions are made on both mid-lateral aspects of the digit. Care must be taken to avoid creating a "through-and-through" tunnel that could compromise pulp viability.
-
Hockey Stick (L-shaped) or J-incision (Fishmouth) / Transverse Incisions:
Historically used but generally
discouraged
. These incisions traverse the volar pulp, increasing the risk of:
- Damage to digital nerves and arteries, leading to paresthesia or ischemia.
- Formation of painful neuromas.
- Painful scarring and contracture of the fingertip.
- Instability of the pulp fat pad.
-
Transverse Volar Incisions:
Absolutely contraindicated due to the high risk of neurovascular damage and subsequent pulp instability.

Figure 11: A depiction of a longitudinal lateral incision for felon drainage (left), contrasted with older, less favored approaches.
-
Unilateral Longitudinal Incision:
The preferred method. A longitudinal incision is made along the
mid-lateral aspect
of the digit, away from the volar pulp and the nail. The incision should be made on the side of maximal fluctuance. It extends from approximately the distal interphalangeal joint crease to just proximal to the nail fold.
-
Drainage and Debridement:
- Once the incision is made, carefully use a mosquito hemostat or blunt probe to break down the fibrous septa within the pulp, ensuring all purulent pockets are entered and drained.
- Obtain a culture for microbiology.
- Copiously irrigate the cavity with sterile saline.
- Inspect for necrotic tissue; debride any devitalized tissue gently.
-
Inspect the distal phalanx if osteomyelitis is suspected; any loose bone fragments should be removed and sent for pathology and culture.
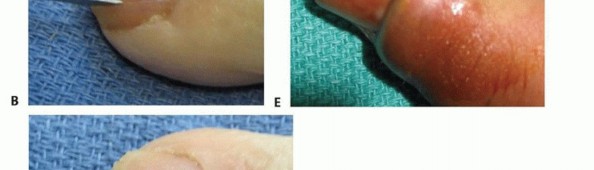
Figure 12: Drainage of a felon following a lateral incision, demonstrating pus evacuation.

Figure 13: Intraoperative view after drainage and debridement of a felon.
-
Wound Management:
- A small piece of loose gauze packing (e.g., iodoform gauze or plain gauze wick) is typically placed in the incision to maintain drainage and prevent premature skin closure. This is usually removed in 24-48 hours.
- Do not suture the wound closed.
-
Apply a sterile, bulky dressing over the packing.

Figure 14: Post-operative dressing applied after felon drainage and packing.

Figure 15: Example of a packed wound following incision and drainage of a felon.
Complications & Management
Despite appropriate surgical intervention, complications can arise, necessitating vigilant post-operative care and, at times, further management strategies.
Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence | Salvage / Management Strategy |
|---|---|---|
| Infection Recurrence | 5-15% (varies by primary condition and patient factors) | Re-evaluation for retained purulent material, inadequate drainage, or resistant organisms. Repeat I&D, adjust antibiotic regimen based on culture results. For chronic paronychia, consider more aggressive eponychial marsupialization or re-excision. Rule out underlying osteomyelitis or foreign body. |
| Onychodystrophy / Nail Deformity | Up to 20-30% after severe paronychia or matrix injury | Prevention is key by preserving the nail matrix. For established dystrophy, protective nail care, topical agents (e.g., urea cream), or nail avulsion. If severe and painful, surgical reconstruction or permanent matrix ablation (chemical or surgical) may be considered, but often not without cosmetic compromise. |
| Persistent Pain/Scarring | Variable, depending on incision technique (higher with volar/transverse felon incisions). | Early mobilization and scar massage. Silicone sheeting or topical steroids for hypertrophic scars. Nerve blocks or gabapentinoids for neuropathic pain. Excision of painful neuromas in select cases (rare). |
| Digital Stiffness/Contracture | 10-15%, especially after prolonged immobilization or extensive infection. | Early and aggressive hand therapy, range-of-motion exercises, dynamic splinting. Surgical release of contractures (e.g., capsulotomy, tenolysis) in refractory cases. |
| Osteomyelitis of Distal Phalanx | <5%, higher in felons or delayed treatment. | Confirmation via MRI or bone biopsy. Prolonged course of culture-directed intravenous antibiotics (4-6 weeks). Surgical debridement of necrotic bone; partial phalangectomy if severe and persistent. |
| Septic Arthritis / Tenosynovitis | Rare (<1%), typically from deeper spread of felon. | Urgent surgical drainage and debridement of joint or tendon sheath. Culture-directed IV antibiotics. Serial irrigation and debridement may be necessary. Hand therapy to prevent stiffness. |
| Anesthetic/Hypesthetic Fingertip | Up to 10-15% with inappropriate felon incisions (e.g., J-incision). | Prevention through proper incision placement. Usually resolves partially over time. Nerve gliding exercises. Surgical exploration and neurolysis for persistent symptomatic nerve compression/entrapment (rare). |
| Complex Regional Pain Syndrome (CRPS) | Rare (<1%), but devastating. | Early recognition is crucial. Aggressive pain management, sympathetic blocks, hand therapy focusing on desensitization and active range of motion. Neuromodulation in refractory cases. |
General Management Principles for Complications:
- Prompt Diagnosis: Early identification of complications is key to effective management.
- Culture-Directed Therapy: Re-culture any recurrent infection and tailor antibiotic therapy based on sensitivities.
- Multidisciplinary Approach: Collaborate with infectious disease specialists, hand therapists, and pain management teams as needed.
- Patient Education: Inform patients about potential complications and the importance of adherence to post-operative care and rehabilitation protocols.
Post-Operative Rehabilitation Protocols
Post-operative care and rehabilitation are critical for optimizing functional outcomes, preventing complications, and ensuring complete recovery after surgical intervention for paronychia and felons.
General Principles
- Wound Care: Maintain a clean wound environment. Regular dressing changes are essential, typically daily or every other day. Non-adherent dressings are preferred.
- Soaks: Warm saline or dilute antiseptic soaks (e.g., povidone-iodine solution) 2-3 times daily for 10-15 minutes can aid wound cleansing, reduce pain, and promote drainage.
- Elevation: Keep the affected hand elevated, especially in the first few days, to reduce swelling and pain.
- Pain Management: Prescribe appropriate analgesia (NSAIDs, acetaminophen, or short-course opioids for severe pain).
- Antibiotics: Continue the prescribed course of oral antibiotics, typically 7-10 days, or as directed by culture results and clinical response.
Specific Protocols
Acute Paronychia
- Wound Packing: If packing was inserted to maintain drainage, it is usually removed within 24-48 hours.
- Mobilization: Encourage early active range of motion of the affected digit and adjacent joints as soon as pain allows. This helps prevent stiffness.
- Nail Care: Advise gentle nail care and avoidance of cuticle manipulation.
- Return to Activity: Light activities can typically resume within a few days to a week. Avoid activities that could re-injure the nail fold until complete healing.
Chronic Paronychia (Post-Eponychial Marsupialization)
- Wound Care: The wound is left open to heal by secondary intention. Continue regular soaks and dressing changes until the wound is clean and granulating. Healing can take several weeks (4-8 weeks).
- Water Exposure: Strict avoidance of prolonged water exposure during the healing phase and ideally thereafter, using waterproof gloves for wet work. This is crucial for preventing recurrence.
- Mobilization: Gentle active range of motion should be initiated early to prevent stiffness.
- Steroids: In some cases, topical steroids may be used once the wound has closed to manage residual inflammation or hypertrophic scarring.
- Nail Growth: Expect the nail plate to appear abnormal during initial regrowth if the matrix was affected; improvement typically occurs over 6-12 months.
Felon
- Wound Packing: The packing (if used) is typically removed within 24-48 hours. After removal, warm soaks and gentle massage can help encourage further drainage.
- Mobilization: Early active and passive range of motion exercises for the affected digit are paramount to prevent stiffness, particularly of the DIP joint. This should begin once acute pain subsides and drainage lessens.
- Swelling Management: Continue elevation. Gentle massage of the fingertip can help reduce residual swelling and improve tissue pliability once the wound is stable.
- Sensation: Monitor for persistent numbness or altered sensation. Nerve gliding exercises may be beneficial if nerve irritation is present.
- Return to Activity: Avoid heavy gripping or activities that put direct pressure on the fingertip until the wound is fully healed and the pulp has regained its normal contour and stability. This may take several weeks.
Hand Therapy Referral
-
Consider referral to a certified hand therapist for patients with:
- Significant pain or stiffness limiting joint motion.
- Delayed wound healing or hypertrophic scarring.
- Persistent swelling or pulp induration.
- Neuropathic symptoms.
- Complex Regional Pain Syndrome (CRPS) development.
- Patients requiring guidance on specific exercise programs, splinting, or desensitization techniques.
Summary of Key Literature / Guidelines
The surgical management of paronychia and felons is largely guided by established principles of hand surgery, focusing on appropriate drainage, debridement, and preservation of functional anatomy. While extensive randomized controlled trials are less common for these acute conditions compared to complex orthopedic procedures, a consensus has emerged from clinical experience, observational studies, and expert opinion.
Key Principles from Literature:
- Early Intervention: Literature consistently supports early incision and drainage for fluctuant abscesses (both paronychia and felons) to prevent progression, reduce pain, and minimize complications such as osteomyelitis. Delay in treatment is a significant risk factor for adverse outcomes.
- Accurate Diagnosis: Differentiating bacterial infections from conditions like herpetic whitlow is paramount. Misdiagnosis and inappropriate surgical intervention for herpetic whitlow lead to worsening viral spread and complications. Clinical examination and patient history are often sufficient, but ancillary tests (Tzanck smear, viral culture) confirm challenging cases.
-
Surgical Incision Selection:
- For felons, the literature strongly advocates for unilateral longitudinal mid-lateral incisions . These approaches provide adequate drainage while minimizing the risk of digital nerve injury, pulp instability, and painful scarring compared to older techniques such as transverse (fishmouth/J-shaped) incisions. While these older techniques ensure thorough drainage, the long-term morbidity associated with them has led to their general abandonment.
- For acute paronychia, simple elevation of the nail fold or a small unilateral incision is typically sufficient. Subungual extensions necessitate partial nail avulsion.
- For chronic paronychia, eponychial marsupialization (e.g., modified Atasoy or Kutler technique) is widely regarded as the most effective surgical treatment for recalcitrant cases, providing high success rates by excising the chronically inflamed pocket and promoting healing by secondary intention.
- Culture-Directed Antibiotics: Obtaining cultures of purulent material is a crucial step, especially for deeper infections or those resistant to initial empiric therapy. While empiric antibiotics targeting Staphylococcus aureus are often initiated, definitive treatment should be guided by culture and sensitivity results. The routine use of post-operative antibiotics for simple acute paronychia after adequate drainage is debated, but generally recommended for felons, deep infections, or immunocompromised patients.
- Preservation of Nail Matrix: All surgical approaches to paronychia emphasize careful technique to avoid injury to the nail matrix. Irreversible damage to the germinal matrix can result in permanent nail dystrophy.
- Post-Operative Management: Adherence to wound care, early mobilization, and avoidance of exacerbating factors (especially water exposure for chronic paronychia) are consistently highlighted as essential components for successful recovery and preventing recurrence.
Guidelines:
While no single, overarching national or international guideline body specifically details the surgical treatment of paronychia and felons in orthopedics, the principles outlined above are widely accepted within the hand surgery community, often integrated into surgical hand trauma and infection management protocols by professional organizations such as the American Society for Surgery of the Hand (ASSH) and the British Society for Surgery of the Hand (BSSH). The emphasis remains on a meticulous, anatomically aware surgical technique combined with appropriate post-operative care to optimize functional and cosmetic outcomes for these common hand infections.
Clinical & Radiographic Imaging
You Might Also Like