Orthopedic Screw Diameter: Advanced Biomechanics, Anatomy, and Clinical Significance
Key Takeaway
Orthopedic screw diameter is critical as it profoundly impacts mechanical integrity. The core diameter dictates bending and torsional strength, affecting fatigue resistance. The major diameter, with thread depth, determines pull-out strength and bone purchase. Understanding these biomechanical principles is essential for optimal screw selection, ensuring stable fixation and successful clinical outcomes.
Introduction & Epidemiology
Screw fixation remains a cornerstone of orthopedic surgery, providing essential stability for fracture repair, arthrodesis, and osteotomies across various anatomical regions. From the intricate small bone surgery of the hand and foot to complex long bone and spinal reconstructions, the judicious application of orthopedic screws is paramount to achieving successful clinical outcomes. The efficacy of screw fixation is intrinsically linked to fundamental biomechanical principles, among which screw diameter stands as a critical determinant of strength, fit, and ultimately, construct longevity.
The evolution of screw design, materials, and surgical techniques has been continuous since the pioneering work of Robert Danis and the subsequent systematization by the AO Foundation. Despite advancements in plating technology, intramedullary nailing, and external fixation, the direct application of screws for compression, lag fixation, or positional stability continues to be indispensable. Epidemiologically, screw usage is ubiquitous, with millions of screws implanted annually worldwide in procedures ranging from simple malleolar fractures to complex acetabular reconstructions. Understanding the nuances of screw mechanics, particularly the impact of diameter on mechanical performance, is thus a high-yield topic for every orthopedic surgeon.
Surgical Anatomy & Biomechanics
The mechanical behavior and clinical performance of an orthopedic screw are directly dictated by its specific anatomical features, which in turn are critically dependent on its diameter in millimeters. A comprehensive understanding of these components and their biomechanical implications is foundational for appropriate screw selection and application.

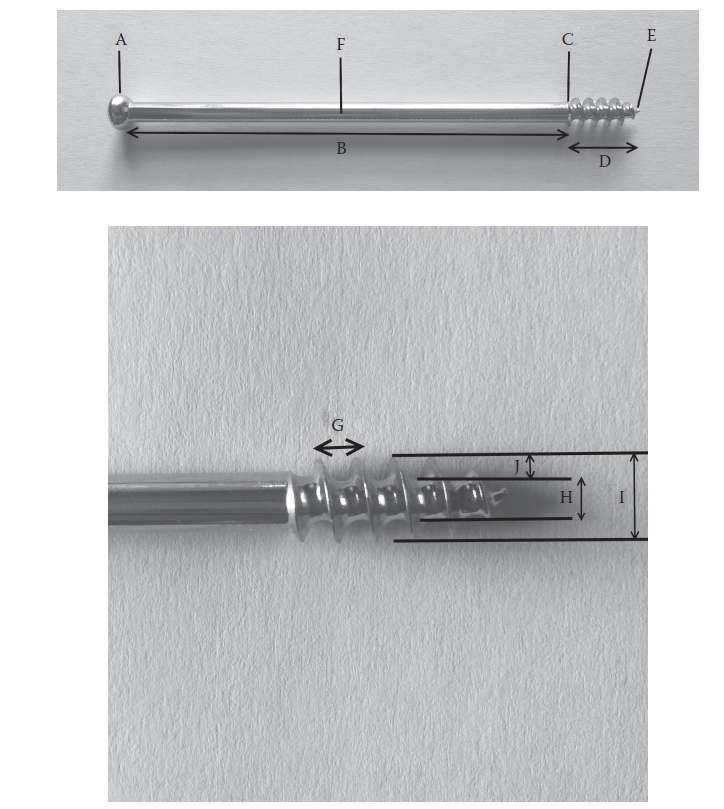
A screw is a mechanical device designed to convert a rotational force (torque) into a linear movement. Its primary function in orthopedic applications is to connect two or more objects, typically bone fragments, by compressing them together, or to provide stable fixation in conjunction with plates. The critical components of an orthopedic screw, as illustrated, include:
- A – Head: The head provides a secure interface for the screwdriver, facilitating the application of torque. Modern head designs, particularly hexagonal or star-drive recesses, are engineered to maximize torque transmission, minimize cam-out, and improve directional control during insertion. The undersurface of the head, when fully seated, acts to prevent further forward motion and provides compressive force against the bone or plate. The design of the head also influences stress distribution at the bone-screw interface and can impact hardware prominence.
- B – Shank (Non-threaded portion): In partially threaded screws, the smooth shank allows a glide hole in the near cortex, essential for achieving interfragmentary compression (lag screw principle). The length of the shank in these screws must correspond to the thickness of the fragment through which it glides.
- C – Run out: This is the transitional zone where the threaded portion of the screw meets the shaft or head. The run-out is a critical region as it represents a stress riser where the cross-sectional area changes abruptly. Consequently, it is often the site where screws are most susceptible to fatigue fracture under cyclic loading. Optimized run-out designs aim to minimize this stress concentration.
- D – Thread: The threads are helical ridges designed to engage and grip the bone. The design of the thread—including its pitch, depth, and profile—is optimized for different bone types and desired mechanical properties.
- E – Tip: The tip is the leading end of the screw. Self-tapping screws feature flutes and a sharpened tip to create their own pilot hole and thread path, eliminating the need for pre-tapping. Non-self-tapping screws require a pre-drilled and pre-tapped hole.
- F – Shaft: This term is often used interchangeably with the body of the screw, encompassing both the threaded and unthreaded portions.
- G – Pitch: The pitch is defined as the axial distance between adjacent threads. It represents the linear distance the screw advances for every single 360-degree turn. A larger pitch allows for faster insertion but may provide less thread purchase per unit length. Cortical screws typically have a fine pitch, while cancellous screws have a coarser pitch.
- H – Core diameter (Minor diameter): This is the diameter of the central core of the screw, measured at the base of the threads. The core diameter is the most critical determinant of a screw’s bending strength, torsional strength, and fatigue resistance. A larger core diameter directly correlates with greater resistance to bending and torsional forces and significantly improves the screw’s fatigue life. The size of the drill bit used to create the pilot hole is equal to the core diameter of the screw for optimal bone-screw interface.
- I – Thread diameter (Major diameter): This is the maximum diameter of the screw, measured at the outer edge of the threads. The major diameter, in conjunction with thread depth, determines the screw’s pull-out strength and its purchase in bone.
- J – Thread depth: Thread depth is half of the difference between the major diameter and the minor (core) diameter. It represents the height of the thread from the core to the outer edge. Greater thread depth, particularly in cancellous screws, increases the surface area of bone engagement, significantly enhancing pull-out resistance.
Biomechanics of Screw Diameter:
The choice of screw diameter in millimeters is not arbitrary; it profoundly impacts the construct’s mechanical integrity.
-
Bending Strength: This is primarily a function of the core diameter (H). According to beam theory, bending stiffness is proportional to the fourth power of the radius (or diameter). Therefore, a small increase in core diameter leads to a substantial increase in bending strength and resistance to plastic deformation. A 4.5 mm cortical screw, for instance, has a significantly greater bending strength than a 3.5 mm cortical screw, due to its larger core diameter. This is crucial in high-stress areas or when the screw is expected to bear substantial load.
-
Torsional Strength: Also largely dependent on the core diameter . Screws must withstand the torsional forces applied during insertion without fracturing. A larger core diameter provides greater resistance to shear stresses.
-
Fatigue Life: Repeated cyclic loading is inherent in musculoskeletal function. Fatigue failure, often occurring at the run-out (C), is a common mode of screw failure. A larger core diameter (H) increases the fatigue resistance by distributing stresses over a larger cross-sectional area and by allowing for a more gradual transition at the run-out. This is particularly relevant in situations requiring long-term implant stability, such as arthrodesis or slow-healing fractures.
-
Pull-out Strength: This refers to the force required to pull the screw axially out of the bone. It is predominantly influenced by the major diameter (I), thread depth (J), and the quality of the bone. Larger major diameter and deeper threads provide a greater surface area for bone engagement, leading to increased pull-out resistance. This is why cancellous screws, designed for softer, trabecular bone, typically have a larger major diameter and deeper, coarser threads compared to cortical screws. The number of cortices engaged (monocortical vs. bicortical) also significantly impacts pull-out strength.
-
Shear Strength at the Bone-Screw Interface: This relates to the ability of the bone threads to resist stripping when torque is applied during insertion or under subsequent loading. This is influenced by thread depth, thread form, and bone quality. An appropriately sized core diameter ensures adequate bone between threads, maximizing resistance to stripping.

Screw Types and Diameter Considerations:
- Cortical Screws: Characterized by smaller major diameters (e.g., 2.7 mm, 3.5 mm, 4.5 mm), finer pitch, and shallower threads. They are designed for dense cortical bone, providing excellent purchase through multiple cortices. The emphasis is on core diameter for bending strength in a predominantly load-sharing construct.
- Cancellous Screws: Feature larger major diameters (e.g., 4.0 mm, 6.5 mm, 7.3 mm), coarser pitch, and deeper threads. Optimized for engagement in softer cancellous bone, prioritizing pull-out strength through increased thread-bone interface. They are often partially threaded to achieve lag compression across the fracture gap.
- Locking Screws: These screws thread into a specially designed plate hole, creating a fixed-angle construct. While their primary stability comes from the fixed-angle interface with the plate, the core diameter of locking screws remains critical for their intrinsic strength and fatigue resistance. Unlike conventional screws, their pull-out strength from bone is less dependent on interfragmentary compression and more on the integrity of the bone-screw interface and the fixed-angle construct.
- Self-Tapping Screws: The flutes present in self-tapping screws facilitate the removal of swarf (bone debris) during insertion. This reduces insertion torque and helps prevent thread stripping by clearing bone from the thread path.
In summary, the specific diameter chosen for an orthopedic screw directly dictates its mechanical properties, including bending, torsional, and pull-out strength, as well as its fatigue life. This profound influence mandates meticulous selection based on biomechanical principles, bone quality, and anticipated loading conditions.
Indications & Contraindications
The indications for screw fixation in orthopedic surgery are vast, encompassing nearly all subspecialties. The choice of screw diameter and type is directly correlated with the specific anatomical site, bone quality, fracture morphology, and desired mechanical stability.
General Indications for Screw Fixation:
-
Fracture Fixation:
- Interfragmentary compression (Lag Screw Principle): Achieves direct reduction and compression of fracture fragments. Applicable in oblique, spiral, or butterfly fractures (e.g., tibial shaft, malleoli, humeral condyle).
- Positional Screws: Holds fragments in a reduced position without compression, often in short oblique or transverse fractures, or to prevent displacement (e.g., syndesmotic screws, screws for patellar fractures).
- Plate Fixation: Used in conjunction with plates to secure the plate to the bone and/or compress fragments. This includes cortical screws, cancellous screws, and locking screws.
- Arthrodesis: Fusion of joints (e.g., ankle, subtalar, knee, wrist, spine) to provide rigid compression across the fusion site, promoting bone union.
- Osteotomies: Stabilization after corrective osteotomies (e.g., high tibial osteotomy, femoral osteotomy, bunionectomy).
- Ligament/Tendon Reattachment: Securing soft tissues to bone (e.g., ACL reconstruction, rotator cuff repair using interference screws).
- Tumor Resection Reconstruction: Providing stability after bone tumor excision and reconstruction.
Specific Diameter Considerations for Indications:
-
Small Diameter Screws (1.5mm, 2.0mm, 2.4mm, 2.7mm):
- Indications: Hand, wrist, foot, ankle, facial fractures; pediatric fractures; small fragment fixation; periarticular fractures in low-stress areas. Cortical screws (e.g., 2.7mm, 3.5mm) for diaphyseal fractures in the radius/ulna.
- Rationale: Smaller size to match small bone anatomy, minimize soft tissue irritation, and prevent iatrogenic fracture of small bones. Sufficient strength for low-load applications.
-
Medium Diameter Screws (3.5mm, 4.0mm):
- Indications: Forearm fractures (both diaphyseal and periarticular), ankle fractures (malleoli), fibula fractures, small to medium fragment cortical fixation, metaphyseal fixation in larger bones. 4.0mm cancellous screws are common in the metaphysis of long bones.
- Rationale: Offers a balance of strength and size for a wide range of applications, providing improved bending and torsional strength over smaller screws.
-
Large Diameter Screws (4.5mm, 6.5mm, 7.3mm):
- Indications: Long bone diaphyseal and metaphyseal fixation, intertrochanteric fractures, femoral neck fractures, tibial plateau fractures, calcaneal fractures, spine fusion (pedicle screws are typically large diameter, e.g., 5.5mm-7.5mm).
- Rationale: Maximize pull-out strength in cancellous bone and provide robust bending and torsional strength for high-load-bearing situations. Critical for primary weight-bearing constructs.
Contraindications for Screw Fixation:
Absolute contraindications for screw fixation are generally aligned with those for any internal fixation, while relative contraindications often involve balancing the benefits of fixation against potential risks, often related to bone quality or infection.
-
Absolute Contraindications:
- Active Local Infection: Significant risk of septic arthritis, osteomyelitis, and implant failure.
- Severely Compromised Soft Tissues: Open wounds, necrotic tissue, or inadequate soft tissue coverage that precludes primary closure and increases infection risk.
- Inadequate Bone Stock: Severely comminuted fractures or critical bone loss where screws cannot achieve adequate purchase, leading to inevitable failure.
-
Relative Contraindications:
- Severe Osteoporosis: Reduced bone quality significantly compromises screw pull-out strength, increasing the risk of screw loosening, stripping, or iatrogenic fracture during insertion. This often necessitates adjunctive fixation methods (e.g., locking plates, cement augmentation) or larger diameter screws to maximize bone engagement.
- Patient Non-Compliance: Unreliable patients who may not adhere to post-operative weight-bearing or rehabilitation protocols, risking implant failure.
- Medical Comorbidities: Uncontrolled diabetes, severe peripheral vascular disease, or immunosuppression that increases surgical risks and impairs bone healing.
- Highly Comminuted Fractures Unsuitable for Direct Reduction: Fractures with multiple small fragments where screws alone cannot achieve stable fixation; often requiring plate fixation as a bridge.
Table of Operative vs. Non-Operative Indications for Fracture Management Where Screw Fixation May Be Considered
| Indication Category | Operative Management (Screw Fixation Typically Indicated) | Non-Operative Management (Screw Fixation Averted/Contraindicated) |
|---|---|---|
| Fracture Displacement | Displaced Intra-articular Fractures: To restore anatomical congruence (e.g., tibial plateau, pilon, malleolar fractures, femoral condyle). | Non-Displaced or Minimally Displaced Fractures: Stable patterns with acceptable alignment (e.g., stable ankle fractures, some distal radius fractures, toe/finger phalanx fractures). |
| Unstable Extra-articular Fractures: Requiring rigid stabilization to prevent displacement (e.g., oblique/spiral long bone fractures, unstable pelvic ring injuries). | Stable Extra-articular Fractures: Not prone to displacement (e.g., undisplaced avulsion fractures, stress fractures). | |
| Functional Demands | Fractures in High-Demand Patients: To allow early mobilization and return to function (e.g., athletes, young active individuals). | Fractures in Low-Demand, Frail Patients: Where surgery poses significant risks, and functional outcome with non-operative care is acceptable, or where bone quality is too poor for fixation. |
| Bone Quality | Adequate Bone Stock: Allows for secure screw purchase and stable construct. Larger diameter screws or locking constructs may be chosen in moderately osteopenic bone. | Severe Osteoporosis: Insufficient bone quality for reliable screw purchase; high risk of pull-out or stripping. Alternative fixation (e.g., external fixation) or non-operative care may be chosen. |
| Soft Tissue Envelope | Healthy Soft Tissues: Allows for primary wound closure and minimizes infection risk. | Severe Open Fractures (Gustilo Type III B/C) / Active Infection: High risk of deep infection, requiring initial debridement, external fixation, or delayed definitive fixation. |
| Fracture Pattern | Long Oblique/Spiral Fractures: Ideal for lag screw fixation. | Highly Comminuted Fractures: Where individual fragments are too small for screw purchase, or extensive bone loss; often requiring bridging plates or non-operative management if stable. |
| Articular Depression/Impaction: Requiring elevation and subchondral support (e.g., tibial plateau, calcaneal fractures), often secured with cancellous screws. | ||
| Associated Injuries | Polytrauma Patients with Multiple Injuries: Early definitive fixation often improves overall patient outcome, decreases hospital stay, and prevents complications (e.g., fat embolism syndrome). | Medical Instability: Patients too unwell to tolerate surgery; temporary stabilization or non-operative care until stable. |
| Location | Weight-Bearing Joints/Bones: Requires rigid fixation to allow for early weight-bearing and prevent collapse (e.g., femur, tibia, ankle, pelvis). | Non-Weight-Bearing or Less Critical Bones: Where acceptable function can be achieved with non-operative management (e.g., some metacarpal/metatarsal fractures, undisplaced ulna shaft fractures with intact radius). |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful orthopedic screw fixation, directly influencing implant selection, surgical approach, and reduction strategy. The selection of appropriate screw diameter, length, and type is a critical aspect of this phase.
Pre-Operative Assessment & Imaging
- Clinical Evaluation: A thorough history and physical examination are essential to assess the patient's overall health, comorbidities, neurovascular status, and the condition of the soft tissue envelope around the fracture site.
-
Radiographic Imaging:
- Standard Radiographs: Anteroposterior and lateral views, often supplemented by oblique views, are the initial and most fundamental imaging modalities. They provide basic information on fracture pattern, displacement, and approximate bone dimensions.
- Computed Tomography (CT) Scans: Indispensable for complex periarticular fractures (e.g., tibial plateau, pilon, acetabulum, calcaneus), assessing articular congruence, fragment size, and location. 3D reconstructions are particularly valuable for understanding fracture morphology and planning screw trajectory. CT also helps evaluate bone density, which influences screw pull-out strength and diameter selection.
- Magnetic Resonance Imaging (MRI): Less frequently used for acute fracture planning but invaluable for assessing associated soft tissue injuries (ligamentous, meniscal, tendinous) that may influence the overall treatment plan and necessitate specific screw applications (e.g., interference screws for ligament repair).
Screw Selection Algorithm
The choice of screw parameters, especially diameter, is multifactorial:
- Bone Quality and Density: In osteoporotic bone, larger major diameter screws with deep threads (e.g., 6.5mm cancellous screws) are preferred to maximize bone-screw interface and pull-out strength. Locking screws may be chosen to provide angular stability, with their larger core diameter offering superior bending strength, reducing the reliance on bone purchase.
-
Anatomical Location and Bone Size:
- Small bones (hand, foot, wrist) dictate smaller diameter screws (1.5mm, 2.0mm, 2.4mm, 2.7mm) to avoid iatrogenic fracture and soft tissue prominence.
- Large long bones and pelvis require larger diameter screws (3.5mm, 4.5mm cortical; 4.0mm, 6.5mm, 7.3mm cancellous) to withstand higher physiological loads.
-
Fracture Pattern and Biomechanical Demand:
- Interfragmentary Compression: Lag screws (partially threaded or fully threaded with overdrilled near cortex) are chosen. The core diameter should be sufficient to prevent shear fracture during compression, and the major diameter/thread depth for adequate pull-out.
- Neutralization/Position Fixation: Screws placed in neutral holes of plates, or positional screws (e.g., syndesmotic screws). The diameter should match the plate holes and provide adequate strength without compromising bone integrity.
- Load-Bearing: Screws acting as primary load bearers (e.g., in comminuted metaphyseal fractures fixed with locking plates) require robust core diameters for bending and fatigue strength.
- Screw Length: Critical for bicortical purchase (where desired) and avoiding neurovascular structures. Measurements are taken from pre-operative imaging and intra-operatively.
-
Screw Type:
- Cortical vs. Cancellous: Based on the predominant bone type at the fixation site.
- Fully vs. Partially Threaded: For lag vs. positional/plate fixation.
- Self-Tapping vs. Non-Self-Tapping: Self-tapping are more convenient, but non-self-tapping (requiring pre-tapping) may offer better bone-screw interface in dense cortical bone.
- Locking vs. Non-Locking: Locking screws provide angular stability, often preferred in osteoporotic bone or comminuted fractures to create a fixed-angle construct.
Instrumentation and Implants
Ensure all necessary instrumentation (drill bits matching core diameters, taps matching major diameters, screw drivers, depth gauges, countersinks) and a full range of appropriate screw diameters and lengths are available. Consider modular trays for efficiency.
Patient Positioning
Patient positioning must allow for optimal surgical exposure, unimpeded imaging access (fluoroscopy), and patient safety.
- Standard Anatomical Positioning: Supine for anterior approaches to the lower extremity (e.g., ankle, knee), lateral decubitus for hip or posterior lower extremity, prone for posterior spine or calcaneus.
- Support and Padding: Adequate padding of pressure points (e.g., heels, elbows, sacrum) and protection of neurovascular structures.
- Tourniquet Application: Typically applied to the proximal limb for exsanguination and bloodless field, especially in extremity surgery. Duration should be monitored.
- Fluoroscopy Access: Critical for confirming reduction and screw placement. Ensure C-arm can obtain required views without repositioning the patient.
Detailed Surgical Approach / Technique
The technical execution of screw fixation is as critical as implant selection, requiring precision to maximize the biomechanical advantages of the chosen screw diameter and avoid complications.
General Principles of Screw Insertion
Regardless of the specific application, the following steps are fundamental:
- Exposure and Reduction: Adequate surgical exposure to visualize the fracture fragments and achieve anatomical reduction. Temporary fixation with K-wires or reduction clamps may be necessary.
-
Pilot Hole Drilling:
- Matching Drill Bit to Core Diameter: This is paramount. The drill bit diameter must be equal to the core (minor) diameter of the screw to ensure optimal thread purchase in bone. An undersized drill bit leads to excessive insertion torque, risking iatrogenic fracture or screw breakage. An oversized drill bit compromises thread engagement and pull-out strength, increasing the risk of stripping and loosening.
- Controlled Drilling: Use sharp drill bits, appropriate speed (often low speed for cortical, higher for cancellous bone), and intermittent drilling with saline irrigation to prevent thermal necrosis of bone. Thermal injury compromises bone viability and weakens the bone-screw interface.
- Correct Trajectory: Drill accurately along the planned trajectory, often under fluoroscopic guidance, ensuring desired bicortical purchase and avoiding neurovascular structures.
-
Countersinking (Optional but Recommended):
- A countersink burr creates a recess in the outer cortex where the screw head will sit flush. This prevents hardware prominence, minimizes soft tissue irritation, and distributes stress more evenly around the screw head, reducing stress concentration at the bone-screw interface. Essential for cortical screws in dense bone.
-
Depth Measurement:
- Using a depth gauge, measure the exact length required for the screw. For bicortical screws, measure from the near cortex to just beyond the far cortex. For unicortical screws, measure to the far cortex. Accurate length prevents neurovascular impingement and ensures optimal purchase.
-
Tapping (for Non-Self-Tapping Screws):
- If using non-self-tapping screws, a tap corresponding to the major (thread) diameter of the screw is used to create the helical thread path in the bone. Tapping reduces insertion torque, especially in dense cortical bone, and minimizes the risk of stripping or iatrogenic fracture during screw insertion. The tap should be advanced carefully, often under fluoroscopic control.
-
Screw Insertion:
- Controlled Torque: Insert the screw carefully and slowly, using the appropriate screwdriver. Avoid excessive force or rapid rotation, which can lead to over-compression, thermal necrosis, or stripping of threads, particularly in osteoporotic bone.
- "Feel" for Purchase: A surgeon's tactile sense is crucial. The screw should engage the bone firmly. A sudden loss of resistance indicates stripping.
- Final Seating: Ensure the screw head is fully seated, flush with the bone or plate, but avoid overtightening.
Specific Screw Techniques
-
Lag Screw Principle:
- Purpose: To achieve interfragmentary compression across a fracture plane, converting shear or bending forces into axial compression, which promotes primary bone healing.
-
Technique:
- Near Cortex Overdrilling: For a fully threaded screw or a partially threaded screw functioning as a lag screw, the drill bit used for the near cortex is the same as the major (thread) diameter of the screw. This creates a glide hole, allowing the screw head to pull the far fragment towards the near fragment.
- Far Cortex Drilling: The drill bit for the far cortex is the core (minor) diameter of the screw, ensuring thread purchase in the far fragment.
- Threaded Length: For partially threaded lag screws, the threaded length must be shorter than the distance from the fracture line to the far cortex, ensuring only the far fragment is engaged.
- Diameter Significance: The core diameter dictates the bending strength of the lag screw, crucial for resisting shear forces before complete healing. The major diameter and thread depth determine the grip on the far fragment and the amount of compression achievable without stripping.
-
Position Screws:
- Purpose: To hold fragments in a reduced position without necessarily generating interfragmentary compression. Often used to maintain reduction or to fix ligaments (e.g., syndesmotic screws).
- Technique: Both near and far cortices are drilled with the core (minor) diameter drill bit, and if non-self-tapping, both cortices are tapped. A fully threaded screw is then inserted.
- Diameter Significance: The diameter must be strong enough to resist pull-out and maintain position, often chosen to be relatively small (e.g., 3.5mm or 4.5mm cortical screw) to minimize bone removal, but robust enough to prevent breakage.
-
Neutralization Screws:
- Purpose: Used in conjunction with a plate to protect the lag screws from bending or torsional forces, thus neutralizing the forces acting on the fracture site.
- Technique: Lag screws achieve interfragmentary compression, and then a plate is applied and secured with neutralization screws, often bicortical cortical screws.
- Diameter Significance: The diameter of neutralization screws is chosen to match the plate hole and provide sufficient strength against bending and shear forces, augmenting the primary lag fixation.
-
Buttress Screws:
- Purpose: To prevent collapse of an articular or metaphyseal fragment, often in conjunction with a buttress plate.
- Technique: Screws are placed to support the fragment, often perpendicular to the fragment's tendency to displace.
- Diameter Significance: Diameters are chosen to provide robust mechanical support, often larger cancellous screws in metaphyseal bone or cortical screws in denser regions.
-
Locking Screws (Fixed-Angle Constructs):
- Purpose: To create a fixed-angle construct with a plate, providing angular stability, particularly advantageous in comminuted fractures or osteoporotic bone where direct screw purchase may be tenuous.
- Technique: Pilot hole drilling with the core diameter drill bit, followed by insertion of a locking screw that threads into the plate hole. No compression is generated between the plate and bone; instead, the screw acts as a fixed column.
- Diameter Significance: The core diameter of locking screws is paramount for their intrinsic strength and resistance to bending and fatigue. While pull-out from bone is still important, the angular stability provided by the screw-plate interface reduces the dependence on interfragmentary compression. Therefore, larger core diameter locking screws offer superior stability.
Complications & Management
Despite meticulous technique, complications associated with screw fixation can occur, ranging from minor hardware-related issues to catastrophic implant failure. A thorough understanding of these complications, their incidence, and appropriate management strategies is essential. Many of these are directly linked to the selection and application of screw diameter.
Common Complications
-
Screw Breakage (Incidence: 1-5%):
- Etiology: Most commonly due to fatigue failure from repetitive stress, often occurring at the stress riser of the run-out zone (C) or at the bone-screw interface. Undersized core diameter for the applied load, premature weight-bearing, or non-union can accelerate fatigue.
- Management: If the fracture is healed and the screw is not causing symptoms, observation may be appropriate. If the fracture is unhealed or the broken screw is symptomatic/interfering with function, surgical removal of the broken fragments is indicated. This often requires specialized screw removal kits, trephines, or burrs. Revision with a new, stronger construct (e.g., larger core diameter screw, plate augmentation) is necessary if fixation stability is compromised.
-
Screw Loosening / Pull-out (Incidence: 5-15% in osteoporotic bone):
- Etiology: Inadequate thread purchase (e.g., undersized major diameter, insufficient thread depth), poor bone quality (osteoporosis), over-tightening leading to stripping, premature weight-bearing, or non-union allowing micromotion.
- Management: If the fracture is healed, symptomatic loose screws can be removed. If the fracture is unhealed and stability is compromised, revision surgery is required. This may involve using larger diameter screws (to engage new bone or stripped holes), longer screws, bone grafting, cement augmentation (especially in osteoporotic bone), or converting to a different fixation method (e.g., locking plate, intramedullary nail).
-
Stripping of Threads (Incidence: 2-10%):
- Etiology: Applying excessive insertion torque, using an undersized pilot drill bit (leading to too much interference), using a mismatched tap, or poor bone quality (especially osteoporosis). This occurs when the bone threads fail to resist the shear forces generated by the screw.
- Management: If encountered during insertion, immediate action is required. One can attempt to move to a larger diameter screw (salvage screw) if sufficient bone stock allows. Alternatively, the stripped hole can be augmented with bone cement, or bicortical purchase can be sought if the stripping was unicortical. If the hole is unusable, a new trajectory or fixation point may be required.
-
Iatrogenic Fracture during Insertion (Incidence: <1-3%):
- Etiology: Occurs when the screw diameter is too large for the bone, when insertion torque is excessive, or when drilling/tapping creates stress risers in compromised bone. Small bones or osteoporotic bone are particularly susceptible.
- Management: Depending on the fracture pattern and stability, this may require immediate modification of the fixation plan, including using a smaller diameter screw, plate augmentation, or revising the entire construct.
-
Infection (Incidence: <1-5% for elective procedures):
- Etiology: A general complication of all surgical procedures, but the presence of foreign material (screws) can provide a nidus for bacterial colonization.
- Management: Superficial infections may be managed with antibiotics and local wound care. Deep infections often require surgical debridement, pulsed lavage, appropriate antibiotic therapy, and potentially removal of hardware once the fracture has healed or if stability is compromised.
-
Neurovascular Injury (Incidence: <1%):
- Etiology: Incorrect screw trajectory or excessive screw length, particularly problematic near major nerves (e.g., peroneal nerve around fibular head, median nerve in distal radius) or blood vessels.
- Management: Immediate recognition is key. If neurological deficit or vascular compromise is noted, the screw must be repositioned or removed immediately. Surgical exploration and repair of damaged structures may be necessary. Meticulous pre-operative planning and intra-operative fluoroscopy help minimize this risk.
-
Nonunion / Malunion (Incidence: 5-10%):
- Etiology: Inadequate stability of the screw construct (often due to inappropriate screw diameter, poor biomechanical design, or early weight-bearing), poor bone biology, infection, or poor reduction.
- Management: Nonunions often require revision surgery, including removal of failed hardware, biological augmentation (bone grafting), and more rigid fixation (e.g., larger diameter screws, locking plates, intramedullary nails). Malunions are managed with corrective osteotomy if symptomatic.
-
Hardware Prominence / Irritation (Incidence: 10-30% in some sites):
- Etiology: Screw heads or shafts protruding under the skin or impinging on tendons, particularly in superficial locations (e.g., ankle, wrist, clavicle, olecranon). Improper countersinking contributes.
- Management: If symptoms are significant after fracture healing, hardware removal is indicated.
Table of Common Complications of Screw Fixation
| Complication | Incidence (Approx.) | Primary Etiologies Related to Screw Diameter/Fit | Salvage Strategies |
|---|---|---|---|
| Screw Breakage | 1-5% | Inadequate core diameter for load (low bending/torsional strength), fatigue failure at run-out, non-union leading to prolonged cyclic stress, poor bone quality. | Removal of broken fragments (specialized kits). Revision with larger core diameter screw or stronger construct (e.g., locking plate, IMN). Bone grafting for non-union. |
| Screw Loosening / Pull-out | 5-15% | Undersized major diameter or insufficient thread depth for bone quality, inadequate number of engaged cortices, osteoporotic bone, over-tightening leading to stripping, premature load bearing. | Removal if healed. Revision with larger major diameter /longer screws (if bone allows), bone graft, cement augmentation, plate reinforcement. Convert to locking plate construct. |
| Stripping of Threads | 2-10% | Excessive insertion torque, undersized pilot hole (not matching core diameter ), mismatched tap to major diameter , poor bone quality (osteoporosis). | Use larger major diameter salvage screw. Augment hole with bone cement. Seek bicortical purchase (if unicortical strip). Relocate screw to new trajectory. |
| Iatrogenic Fracture | <1-3% | Screw diameter too large for bone (especially in small bones or osteoporotic bone), excessive insertion torque, poor pre-drilling technique (e.g., off-center). | Immediate modification of fixation (smaller diameter screw, plate augmentation). Revision of entire construct if unstable. |
| Infection | <1-5% | General surgical risk. Presence of foreign body (screw) as a nidus. | Debridement, pulsed lavage, targeted antibiotics. Hardware removal (if fracture healed or for deep, refractory infection). |
| Neurovascular Injury | <1% | Incorrect screw trajectory, excessive screw length. | Immediate screw repositioning/removal. Surgical exploration and repair of damaged structures. |
| Nonunion / Malunion | 5-10% | Inadequate fixation stability (suboptimal screw diameter or construct design), persistent micromotion, poor biology. | Revision surgery with more rigid fixation (e.g., larger diameter screws, locking plates, IMN). Bone grafting (autograft/allograft). Corrective osteotomy for malunion. |
| Hardware Prominence / Irritation | 10-30% | Inadequate countersinking, incorrect screw length, superficial anatomical location. Screw head diameter too large for available space. | Elective hardware removal after fracture healing. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following screw fixation is tailored to the specific fracture, the stability of the surgical construct, the patient's comorbidities, and the anticipated healing time. The biomechanical strength imparted by the selected screw diameter plays a crucial role in determining the allowed range of motion and weight-bearing status.
Immediate Post-Operative Period (Day 0-7)
- Pain Management: Multimodal analgesia to control post-operative pain and facilitate early mobilization.
- Wound Care: Regular dressing changes, monitoring for signs of infection (erythema, swelling, discharge).
- Edema Control: Elevation of the extremity, compression dressings/stockings, and early active motion (if permitted) to reduce swelling.
-
Early Mobilization (if construct allows):
- Stable Constructs (e.g., Locking plate with robust screws, well-compressed intra-articular fractures): May allow immediate passive or active-assisted range of motion (ROM) in adjacent joints, non-weight-bearing (NWB) to touch-down weight-bearing (TDWB) in the operated extremity, depending on the fracture and location. A strong screw construct (large core diameter, good bone purchase) allows for more aggressive early motion.
- Less Stable Constructs (e.g., delicate fixation in osteoporotic bone, small fragment screws): Often require strict immobilization (splint, brace) and non-weight-bearing.
- Neurovascular Monitoring: Regular checks for sensation, motor function, and vascular integrity.
Early Rehabilitation Phase (Weeks 1-6)
-
Weight-Bearing Progression:
- Gradual progression from NWB to TDWB, then partial weight-bearing (PWB) as per fracture healing and implant stability. Fluoroscopic checks may be performed to confirm construct integrity prior to increasing weight-bearing.
- Large Diameter Screws: Constructs using large diameter cortical or cancellous screws, particularly in load-bearing bones, often permit earlier and more aggressive weight-bearing progression due to their superior bending and pull-out strength.
- Small Diameter Screws: Fixation with small diameter screws (e.g., hand, foot) typically allows earlier functional use, but protected weight-bearing is often maintained longer in the lower extremity.
- Range of Motion (ROM): Continued progression of active and passive ROM exercises, respecting pain and avoiding undue stress on the fracture site.
- Muscle Strengthening: Isometric exercises to maintain muscle tone, progressing to isotonic strengthening as healing advances.
- Gait Training: With assistive devices (crutches, walker) as weight-bearing progresses.
Intermediate Rehabilitation Phase (Weeks 6-12)
- Consolidation of Healing: Radiographic evidence of callus formation and early union.
- Full Weight-Bearing: Typically achieved by this stage for most stable fractures, contingent on clinical and radiographic assessment.
- Progressive Strengthening: Focus on restoring full muscle strength, endurance, and proprioception.
- Functional Activities: Incorporating activities of daily living (ADLs) and specific tasks related to the patient's occupation or hobbies.
Advanced Rehabilitation Phase (Months 3-6+)
- Return to Activity: Gradual return to sports, work, and recreational activities. Emphasis on progressive loading and sport-specific training.
- Monitoring for Complications: Continued vigilance for signs of nonunion, malunion, hardware loosening, or infection.
-
Hardware Removal:
- Indications: Symptomatic hardware (prominence, pain, irritation), impending soft tissue compromise, infection, or prophylactic removal in younger patients (especially in weight-bearing joints) to prevent late fatigue fracture of the implant.
- Timing: Generally, hardware is removed after complete fracture union, typically 12-18 months post-operatively, but can vary from 6 months (e.g., syndesmotic screws) to never (e.g., many locking plates in adults).
- Diameter Implications: Removal of large diameter screws, particularly from dense bone or if ingrown, can be technically challenging and may require specialized instruments.
Summary of Key Literature / Guidelines
The understanding and application of orthopedic screw fixation are deeply rooted in scientific literature and clinical guidelines, prominently shaped by organizations like the AO Foundation. The biomechanical principles of screw diameter, thread design, and bone-screw interaction have been extensively studied.
- AO Principles: The AO (Arbeitsgemeinschaft für Osteosynthesefragen) Foundation has been a driving force in standardizing fracture care, emphasizing anatomical reduction, stable internal fixation (including screws), preservation of blood supply, and early active mobilization. Their principles dictate that screw selection should be based on fracture morphology, bone quality, and anticipated mechanical loads. The lag screw principle, neutralization plating, and buttress fixation are cornerstones of their philosophy.
-
Biomechanical Studies on Screw Strength:
-
Numerous studies have elucidated the relationship between screw design parameters and mechanical properties. Key findings consistently demonstrate that:
- Core diameter is the primary determinant of a screw's bending and torsional strength, with strength increasing exponentially with diameter.
- Major diameter and thread depth are critical for pull-out strength, particularly in cancellous bone. Deeper, coarser threads maximize bone engagement.
- The bone-screw interface is a critical zone; thermal necrosis during drilling or overtightening can compromise this interface and lead to early failure.
- Research comparing cortical and cancellous screw designs highlights their respective optimizations for different bone types, underscoring the importance of diameter and thread morphology.
-
Numerous studies have elucidated the relationship between screw design parameters and mechanical properties. Key findings consistently demonstrate that:
- Fatigue Testing: Long-term in vivo stability of screw fixation relies heavily on fatigue resistance. Studies on fatigue life demonstrate that larger core diameters and optimized run-out designs significantly prolong the lifespan of screws under cyclic loading, a critical factor for constructs intended to last until full biological healing.
- Locking Screw Technology: The advent of locking screws (fixed-angle constructs) represents a significant advancement, particularly for osteoporotic bone and comminuted fractures. Literature supports their enhanced angular stability and reduced dependence on bone quality for primary purchase, though the core diameter remains fundamental for the screw's intrinsic strength. Variable angle locking screws further enhance adaptability.
- Clinical Outcomes Data: Meta-analyses and large cohort studies consistently demonstrate that appropriate screw selection and meticulous surgical technique are associated with lower rates of nonunion, malunion, and hardware-related complications. The correct choice of screw diameter is a recurring theme in minimizing implant failure. For instance, studies on femoral neck fractures often advocate for larger diameter cancellous screws (e.g., 6.5mm, 7.3mm) to enhance stability and reduce reoperation rates.
- Advances in Materials and Coatings: Ongoing research into new materials (e.g., absorbable polymers, advanced titanium alloys) and surface coatings aims to improve biocompatibility, osteointegration, and reduce infection rates. While these innovations are significant, they build upon the foundational biomechanical principles related to screw geometry, including diameter.
In conclusion, the orthopedic literature unequivocally supports the notion that "Why Screw Diameter in mm Matters for Strength & Fit" is not merely an academic exercise but a fundamental concept with direct clinical implications. Optimal outcomes in screw fixation hinge upon a profound understanding of how core diameter dictates bending and fatigue strength, and how major diameter and thread depth govern pull-out resistance and fit within specific bone architecture. Surgeons must continuously integrate this biomechanical knowledge into their pre-operative planning and intra-operative decision-making to select the most appropriate screw diameter for each unique clinical scenario.
Clinical & Radiographic Imaging

You Might Also Like