Polydactyly: Comprehensive Guide to Preaxial & Postaxial Duplications

Key Takeaway
Polydactyly is a congenital anomaly characterized by supernumerary digits, primarily categorized as preaxial (thumb duplication) or postaxial (small finger duplication). Preaxial polydactyly is classified by the Wassel system (Types I-VII), detailing skeletal duplication. Postaxial polydactyly, often simpler, involves well-formed duplicates (Type A) or rudimentary tissue. Understanding embryology and surgical anatomy is crucial for management.
Preaxial and Postaxial Polydactyly
Introduction & Epidemiology
Polydactyly, characterized by supernumerary digits, represents one of the most common congenital hand anomalies. It is defined as having more than the normal complement of five digits on a given limb. This condition is broadly categorized based on the anatomical location of the duplication relative to the limb axes: preaxial (radial side, thumb duplication), central (middle digits), and postaxial (ulnar side, small finger duplication). While the prevalence varies geographically and ethnically, it is generally reported to be between 1 in 500 to 1 in 1,000 live births. Postaxial polydactyly is more prevalent among individuals of African descent, often occurring as an isolated, autosomal dominant trait, whereas preaxial polydactyly is more common in Caucasian and Asian populations, frequently sporadic but can also be syndromic. Central polydactyly is the least common type.
Duplication of digits typically occurs early in embryogenesis, during the complex processes of limb bud formation and patterning. The developing limb bud is orchestrated by several signaling centers along three primary axes:
*
Proximodistal axis:
Modulated by the apical ectodermal ridge (AER), governing limb outgrowth.
*
Anteroposterior (radial-ulnar) axis:
Governed by the zone of polarizing activity (ZPA), which expresses Sonic Hedgehog (SHH) protein. Abnormalities in SHH signaling or its downstream targets (e.g., GLI3) are implicated in various forms of polydactyly. Ectopic SHH expression on the anterior limb bud can lead to preaxial polydactyly, while increased SHH activity or altered temporal expression may contribute to postaxial forms.
*
Dorsal-ventral axis:
Influenced by the Wnt signaling pathway.
Understanding the embryological origins provides crucial insight into the anatomical variations observed in duplicated digits, from rudimentary skin tags to fully articulated, well-formed digits.
Surgical Anatomy & Biomechanics
Successful management of polydactyly hinges upon a comprehensive understanding of the intricate anatomy of the duplicated and residual digits, as well as the biomechanical implications of the anomaly. The extent of duplication can range from a simple soft tissue nubbin to complete duplication of metacarpals and phalanges, often with associated joint abnormalities, tendon anomalies, and neurovascular variations.
Preaxial Polydactyly (Thumb Duplication)
Preaxial polydactyly, or thumb duplication, exhibits significant variability. The Wassel classification, based on the level of skeletal duplication, remains the most widely accepted system for characterizing thumb polydactyly, originally expanding on Flatt's observations. This classification stratifies the anomaly into seven types (I-VII), where Type I represents a bifid distal phalanx and Type VII involves a triphalangeal thumb with duplication at the metacarpal level.

Wassel Classification Summary:
*
Type I:
Bifid distal phalanx.
*
Type II:
Duplication of the distal phalanx (most common type of bony duplication).
*
Type III:
Bifid proximal phalanx.
*
Type IV:
Duplication of the proximal phalanx (most common overall Wassel type, often with associated distal phalanx duplication).
*
Type V:
Bifid metacarpal.
*
Type VI:
Duplication of the metacarpal.
*
Type VII:
Triphalangeal thumb with associated duplication.
In cases of digit duplication, one may observe duplication in some or all of the elements of the finger (bone, nail, joints, and tendon). The duplicate finger may be well formed and near normal in appearance or underdeveloped and rudimentary in appearance.
Key Anatomical Considerations in Thumb Duplication:
*
Skeletal Structures:
Radiographs are essential to define the extent of bony duplication, presence of epiphyses, and articular surfaces. The duplicated components often share common epiphyseal plates or exhibit hypoplasia.
*
Articular Anatomy:
Joint congruity and stability are paramount. Collateral ligaments are frequently hypoplastic, attenuated, or inserted anomalously, leading to inherent instability in the retained digit.
*
Tendon Anatomy:
Extrinsic flexor (FPL) and extensor (EPL, EPB) tendons often bifurcate, with variable insertions into the duplicated digits. Intrinsic muscles (thenar muscles, abductor pollicis brevis, opponens pollicis, adductor pollicis) may also show abnormal insertions, contributing to imbalance and rotational deformities.
*
Neurovascular Bundles:
Each duplicated digit typically possesses its own neurovascular supply. Meticulous dissection is required to preserve the dominant neurovascular bundle of the digit to be retained.
*
Nail Matrix:
Care must be taken to reconstruct a functional and cosmetically acceptable nailbed.
Biomechanics of the Duplicated Thumb:
The primary biomechanical goals for the thumb are opposition, pinch, and grasp. Duplication frequently compromises these functions due to:
*
Angulation:
Often radial or ulnar deviation at the IP or MCP joint.
*
Instability:
Lax collateral ligaments lead to joint instability.
*
Rotational Deformity:
Impaired opposition due to abnormal intrinsic muscle pull.
*
Size Discrepancy:
Unequal size and stiffness of the duplicated parts.
Postaxial Polydactyly (Small Finger Duplication)
Postaxial polydactyly is generally simpler than preaxial duplication but can still present a spectrum of anatomical complexity. It is classified by the degree of skeletal and soft tissue development. A commonly used classification, building on the seed content, identifies:
Postaxial Polydactyly Classification:
*
Type A:
A well-formed duplicate small finger with osseous components (bone or tendon attachments). This may involve duplication at the metacarpal, proximal phalanx, or distal phalanx level.


*
Type B:
A small pediculated nubbin, typically lacking skeletal elements or possessing only rudimentary cartilage/bone within a soft tissue stalk. These are often attached by a narrow skin bridge.
*
Type C & D (less common):
Can involve an isolated metacarpal without phalanges or more complex forms associated with syndactyly.
Key Anatomical Considerations in Small Finger Duplication:
*
Skeletal Structures:
Type A requires careful radiographic assessment to identify the level of duplication (metacarpal, phalangeal) and the presence of shared articular surfaces or growth plates.
*
Neurovascular Bundles:
The duplicated digit typically shares a common neurovascular pedicle with the preserved digit, necessitating careful dissection to avoid injury.
*
Tendons and Ligaments:
The abductor digiti minimi (ADM) muscle often inserts abnormally, frequently into the radial-most duplicated digit, contributing to angulation or splaying. Collateral ligaments may be hypoplastic.
*
Skin and Soft Tissue:
The width of the pedicle and the quality of the surrounding skin are important, particularly for Type B.
Biomechanics of the Duplicated Small Finger:
The small finger contributes significantly to power grip. Postaxial polydactyly primarily causes:
*
Cosmetic Deformity:
The most common concern, especially for well-formed duplicates.
*
Impingement:
During grasp, the supernumerary digit can impinge on the ring finger.
*
Functional Loss:
Less common, but can occur if the dominant digit is removed or if significant splaying compromises grip.
Central Polydactyly
Central polydactyly, involving duplication of the index, middle, or ring fingers, is the rarest and often most complex type. It is frequently associated with syndactyly and other congenital anomalies. The anatomy is highly variable, often involving shared neurovascular bundles, complex tendon insertions, and abnormal articular surfaces.
Indications & Contraindications
The decision-making process for managing polydactyly involves careful consideration of functional impairment, cosmetic concerns, patient age, and associated conditions. The primary goal is to create a functional, stable, and aesthetically acceptable digit, while minimizing complications and preserving growth potential.
General Considerations:
*
Age of Patient:
Early intervention for certain types (e.g., postaxial Type B) versus delayed intervention for complex preaxial types to allow for better anatomical assessment and reduce anesthetic risks.
*
Functional Assessment:
Evaluate grasp, pinch, and fine motor skills.
*
Cosmetic Concerns:
A significant driver for intervention, particularly for well-formed duplicates.
*
Syndromic Associations:
Identification of associated syndromes (e.g., Bardet-Biedl, VACTERL, Fanconi anemia) is critical for comprehensive patient care and genetic counseling.
*
Parental Expectations:
Detailed discussion regarding surgical goals and potential outcomes is essential.
Operative Indications
-
Functional Impairment:
- Compromised grip, pinch, or opposition (e.g., unstable thumb duplication).
- Limited range of motion in the retained digit due to the duplicate.
-
Cosmetic Deformity:
- Well-formed, prominent, or bulky supernumerary digit.
- Digit angulation or splaying.
- Mechanical Impingement or Irritation: The extra digit interferes with daily activities or shoe wear (for foot polydactyly).
- Progressive Deformity: Evidence of worsening angulation or joint instability over time.
- Associated Deformities: Polydactyly with syndactyly requiring separation.
- Pain: Rare in infancy, but can be a factor in older children or adults.
Non-Operative Indications
- Rudimentary Postaxial Nubbins (Type B): Ligation at birth is a common and effective non-operative surgical approach for these non-ossified, pediculated digits, though it is a minor procedure.
- Minimal Functional Deficit: If the duplicate digit causes no functional impairment and minimal cosmetic concern, observation may be appropriate, especially in very young children with high anesthetic risk.
- Severe Comorbidities: Medical conditions precluding safe general anesthesia.
- Parental Preference: After thorough counseling, if parents elect against surgical intervention for non-critical cases.
| Indication Type | Specific Condition / Feature | Decision for Intervention |
|---|---|---|
| Operative | Functional impairment (pinch, grasp, opposition) | Surgical excision and reconstruction |
| Significant cosmetic deformity (well-formed, bulky) | Surgical excision and reconstruction | |
| Joint instability or significant angulation | Surgical reconstruction (osteotomy, ligament repair) | |
| Mechanical impingement or irritation | Surgical excision | |
| Associated syndactyly requiring separation | Surgical separation and reconstruction | |
| Progressive deformity leading to worsening function/cosmesis | Surgical correction | |
| Non-Operative | Rudimentary Postaxial Type B (pediculated nubbin) | Ligation at birth (minor procedure, often outpatient) |
| Minimal functional deficit, mild cosmetic concern | Observation, consider future intervention if concerns arise | |
| Significant medical comorbidities precluding anesthesia | Observation, supportive care | |
| Insufficient tissue for viable reconstruction | Observation, consider prosthetic options |
Contraindications
- Unstable Medical Condition: Patients with severe comorbidities that significantly increase anesthetic risk.
- Acute Infection: Local or systemic infection that needs to be resolved prior to elective surgery.
- Inadequate Tissue: Insufficient healthy tissue for a viable reconstruction, particularly in complex or revision cases.
- Unrealistic Expectations: Patients or parents with expectations that cannot be met surgically should be managed with clear communication and counseling.
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is crucial to optimize outcomes and mitigate complications in polydactyly surgery.
Clinical Evaluation
- Detailed History: Include family history of limb anomalies, syndromic associations, and developmental milestones.
-
Physical Examination:
- Neurovascular Assessment: Capillary refill, sensation, motor function of duplicated and adjacent digits.
- Skeletal Assessment: Range of motion, joint stability, angulation, and rotational deformities.
- Tendon Function: Active and passive range of motion to assess tendon insertions and integrity.
- Skin and Soft Tissue: Assess quality, availability of skin flaps, and scar burden from prior interventions.
- Overall Hand Function: Observe spontaneous use of the hand, grip, and pinch patterns.
Imaging
-
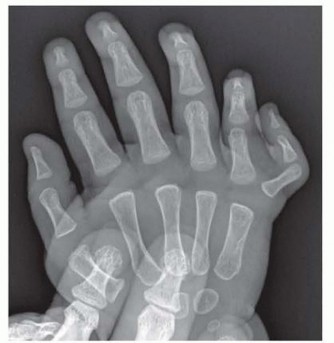
Radiographs:
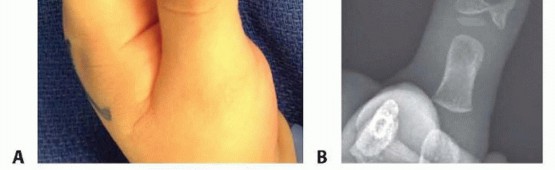
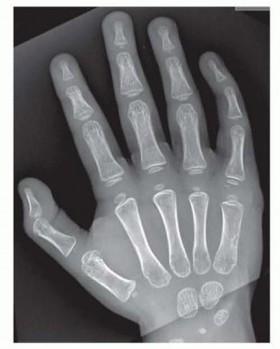
High-quality anteroposterior, lateral, and oblique views are mandatory. These define the skeletal architecture, number of phalanges, presence of epiphyses, joint congruity, and any associated carpal or metacarpal anomalies. Standard views allow for accurate classification (e.g., Wassel for thumb) and detailed surgical planning.
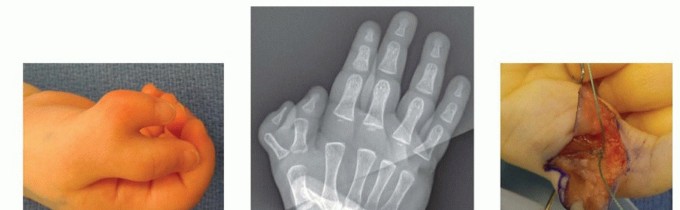
(Likely X-ray of thumb polydactyly)
(Clinical image of preaxial polydactyly)
(Clinical image of preaxial polydactyly) -
Advanced Imaging:
Rarely indicated for routine polydactyly.
- CT Scans: May be considered for very complex cases, especially central polydactyly, to visualize 3D bony architecture, joint surfaces, and guide osteotomy planning.
- MRI: Useful for evaluating soft tissue anomalies, particularly tendon insertions, and neurovascular structures in exceptionally complex cases, but often not necessary.
Timing of Surgery
- Postaxial Polydactyly (Type B): Ligation can be performed shortly after birth (within the first few days or weeks).
- Preaxial & Postaxial (Type A) Polydactyly: Generally performed between 6 and 12 months of age. This timing allows for sufficient growth of the hand, making structures larger and easier to work with, reduces anesthetic risks compared to neonates, and precedes the critical period for developing prehension and fine motor skills.
Surgical Goals
- Preserve or reconstruct a single, functional digit with adequate stability.
- Correct any angular or rotational deformities.
- Achieve a satisfactory cosmetic appearance.
- Prevent growth disturbance.
- Minimize scar burden.
Anesthesia and Positioning
- Anesthesia: General anesthesia is standard for infants and young children. Regional blocks (e.g., axillary block) can be used as an adjunct for post-operative pain control.
- Patient Positioning: Supine with the affected arm on a specialized arm table. The arm should be abducted, externally rotated, and the elbow flexed to allow optimal access to the hand.
- Tourniquet: A pneumatic tourniquet on the upper arm is essential for a bloodless field, which is critical for meticulous dissection of neurovascular structures. For digital procedures, a finger tourniquet may be used.
- Magnification: Loupe magnification (2.5x to 4.5x) is highly recommended for all cases to aid in precise dissection and repair of delicate structures.
Detailed Surgical Approach / Technique
The core principle in polydactyly surgery is the excision of the less functional or less developed duplicate digit, followed by the reconstruction and centralization of the remaining, dominant digit. This often involves careful soft tissue management, bone reshaping, joint stabilization, and tendon rebalancing.
Preaxial Polydactyly (Thumb Duplication)
The surgical approach is largely dictated by the Wassel classification. The radial-most digit is typically excised, as it is often smaller, more unstable, and less functional, but clinical judgment is critical, especially when the ulnar digit is significantly smaller or malformed.
General Steps for Excision and Reconstruction (e.g., Wassel Type IV):
- Incision: A racquet-shaped incision is often employed, encompassing the radial base of the duplicated digit and extending proximally to allow exposure for osteotomies and ligament reconstruction. Skin flaps (e.g., V-Y plasty) may be designed to prevent scar contracture and improve cosmesis.
-
Dissection:
- Carefully identify and preserve the neurovascular bundle to the retained (ulnar) digit. The neurovascular bundle to the radial-most digit is ligated and divided.
- Dissect the extrinsic flexor (FPL) and extensor (EPL, EPB) tendons. These often bifurcate. The tendon slips inserting into the excised digit are identified and either released or harvested for later reconstruction. Those inserting into the retained digit are preserved.
- Address the intrinsic muscles (thenar eminence). The abductor pollicis brevis (APB) and opponens pollicis often have aberrant insertions. The abductor pollicis brevis, if inserting into the radial digit, should be detached and reinserted to the radial side of the remaining proximal phalanx or metacarpal head to provide proper thumb abduction.
-
Skeletal Excision:
- The radial-most metacarpal/phalangeal head or segment is excised. If the duplicated metacarpal head is present, care is taken to reshape the base of the remaining phalanx to articulate with the metacarpal head, creating a stable joint.
-
For Wassel Type IV (Duplication of Proximal Phalanx):
- The radial proximal phalanx is excised. If the remaining ulnar phalanx exhibits angulation, a wedge osteotomy at its base may be performed to correct this, providing a straight axis. The osteotomy is stabilized with a K-wire.
- The retained ulnar proximal phalanx may need to be centralized over the metacarpal head.
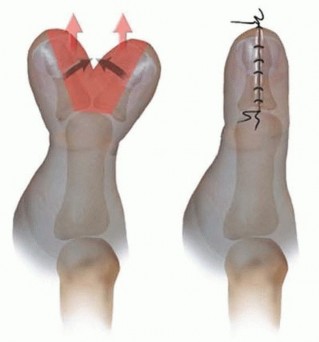
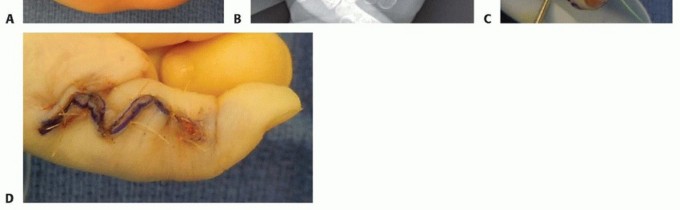
- Bilhaut-Cloquet Procedure: For Wassel Types II and III with two equally sized and functional distal or proximal phalanges, this procedure involves excising a longitudinal wedge from the center of the two digits, then fusing the remaining halves to create a single, broader, but well-aligned digit. This sacrifices the IP joint for Type II, and proximal phalanx joint for Type III. It is generally reserved for situations where both digits are suboptimal and a single functional digit is desired at the cost of fusion.
-
Joint Reconstruction:
- Collateral Ligament Reconstruction: This is paramount for preventing future angulation and instability. The radial collateral ligament of the retained thumb is often deficient. A strip of the joint capsule or a portion of the collateral ligament from the excised digit can be used to reconstruct or reinforce the radial collateral ligament of the preserved digit. The remaining extensor tendon slips may also be utilized to augment collateral ligament stability.
- Capsulorrhaphy around the MCP joint is performed to tighten the capsule.
- Tendon Rebalancing: Reinsert any detached intrinsic muscles (e.g., APB) to the radial aspect of the retained digit to optimize opposition.
- Nailbed Reconstruction: If the duplication involves the distal phalanx, careful reconstruction of the nailbed is required to achieve a cosmetically acceptable nail plate.
- Skin Closure: Meticulous skin closure with fine sutures, using any designed V-Y or Z-plasties to minimize scar contracture and achieve aesthetic results.
Postaxial Polydactyly (Small Finger Duplication)
The surgical approach varies significantly based on Type A or Type B.
Type B (Pediculated Nubbin):
1.
Ligation:
This is typically performed as an outpatient procedure in the nursery or clinic, often within the first few weeks of life.
2.
Technique:
A strong, absorbable suture (e.g., chromic gut or braided absorbable suture) is tied tightly around the base of the pediculated nubbin, ensuring complete constriction of the neurovascular supply. This causes ischemic necrosis and autoamputation.
3.
Post-Ligation:
The digit typically darkens and sloughs off within 7-10 days. Parents are advised on wound care.
*
Caveat:
Ensure no bone or cartilage is present within the stalk on palpation, as ligation of an ossified digit can lead to a painful neuroma or residual stump. If there's any doubt, formal excision is safer.
Type A (Well-formed Duplicate Small Finger):
1.
Incision:
A racquet-shaped or elliptical incision around the ulnar-most (supernumerary) digit, extending proximally to expose the metacarpal if necessary.
2.
Dissection:
* Carefully dissect soft tissues, identifying the common neurovascular bundle. The branch supplying the ulnar-most digit is ligated and divided, while the bundle to the retained (radial) digit is meticulously preserved.
* Release the abductor digiti minimi (ADM) tendon, which frequently inserts into the radial-most of the two small fingers.
3.
Skeletal Excision:
The ulnar-most phalanx or metacarpal head is excised. If the retained digit exhibits angulation or splaying, an osteotomy (e.g., closing wedge) at the base of the retained phalanx or metacarpal head may be required to realign the digit.
4.
Joint and Tendon Reconstruction:
* Reinsert the ADM tendon to the base of the retained proximal phalanx (ulnar aspect) to ensure proper abduction and prevent radial deviation of the small finger.
* Tighten the ulnar collateral ligament of the retained digit by capsulorrhaphy or imbrication, using any available soft tissue.
5.
Skin Closure:
Meticulous layered closure, potentially using Z-plasty for skin lengthening if needed, to prevent scar contracture and ensure an aesthetic outcome.
Central Polydactyly
These are highly complex and demand individualized planning. Often associated with syndactyly, the goal is to create a functional two-phalangeal finger with good alignment and mobility. Techniques may include:
*
Ablation of the least developed digit
with reconstruction of collateral ligaments and tendons.
*
On-top plasty:
Resecting a central portion of a duplicated ray and bringing the viable parts together.
*
Combined excision and osteotomy.
* Often requires staged procedures due to complexity.
Complications & Management
Polydactyly surgery, while generally safe, is not without potential complications. The incidence and severity vary depending on the type of polydactyly, surgical technique, and patient factors.
| Complication | Incidence (Approximate) | Salvage Strategies |
|---|---|---|
| Recurrent Angulation/Deformity | 15-30% (Preaxial thumb) | Revision osteotomy, growth plate manipulation (epiphysiodesis/hemiepiphysiodesis), ligament reconstruction/tightening. Serial splinting in mild cases. |
| Joint Instability | 10-20% (Preaxial thumb) | Ligament reconstruction using local tissue (capsule, tendon graft), tenodesis, joint fusion (rarely in children). |
| Stiffness / Reduced ROM | 5-15% | Aggressive physical therapy, dynamic splinting, scar revision, tenolysis (rarely). |
| Nail Deformity | 5-10% (Distal duplications) | Nailbed reconstruction, matricectomy for ingrown nails, revision of hypertrophic nail folds. |
| Scarring (Hypertrophic, Contracture) | 5-10% | Scar massage, silicone sheeting, intralesional steroid injections, Z-plasty or V-Y plasty for contractures, fractional laser. |
| Growth Arrest / Physeal Injury | <5% | Careful surgical technique to avoid physeal injury. If it occurs, monitor for limb length discrepancy/angulation, consider epiphysiodesis of opposite side or corrective osteotomy. |
| Neurovascular Injury / Ischemia | <1% | Meticulous dissection is key to prevention. Urgent exploration and microvascular repair if recognized intraoperatively. Post-operative monitoring. |
| Infection | <5% | Antibiotic therapy, wound debridement, irrigation. Rarely requires hardware removal. |
| Residual Cosmetic Deformity | Up to 20% | Revision surgery for soft tissue contouring, scar improvement, or re-excision of a prominent stump. |
| Painful Neuroma / Stump (Type B ligation) | 1-5% (if bone present) | Excision of the neuroma/bone fragment and formal surgical excision of the residual stump. |
| Reoperation | 10-25% (overall) | Dependent on primary complication. Patients and families should be counseled on the potential need for revision surgery, especially for thumb polydactyly. |
General Management Principles:
*
Prevention:
Meticulous surgical technique, precise identification and preservation of vital structures, and appropriate fixation are the best preventive measures.
*
Early Recognition:
Careful post-operative monitoring for signs of neurovascular compromise, infection, or excessive swelling.
*
Multidisciplinary Approach:
Collaboration with hand therapists for rehabilitation and geneticists for syndromic cases.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is critical for optimizing functional and aesthetic outcomes, particularly after complex reconstructive procedures. The protocol is individualized based on the specific surgical procedure, stability of the reconstruction, and patient's age.
Immediate Post-Operative Phase (0-3 weeks)
-
Immobilization:
- A well-padded short arm cast or splint (including the thumb if it's the operated digit) is applied to protect the surgical site, maintain corrected alignment, and promote healing.
- For K-wire fixation, the cast/splint immobilizes the joints above and below the osteotomy or fusion site.
- Duration: Typically 3-6 weeks, depending on bone healing and joint stability.
-
Pin Care (if K-wires used):
- Daily cleaning of pin sites with sterile saline or antiseptic solution to prevent infection.
- Monitor for signs of infection (redness, swelling, purulent discharge).
-
Edema Control:
- Elevation of the hand above heart level.
- Gentle compression if appropriate (e.g., soft bandage beneath the cast).
- Pain Management: Age-appropriate analgesia.
Intermediate Phase (3-6 weeks)
- K-wire Removal: K-wires are typically removed at this stage after radiographic confirmation of initial bone healing.
-
Initiation of Motion:
- Once stable, gradual initiation of passive range of motion (PROM) exercises, followed by active range of motion (AROM) , under the guidance of a hand therapist.
- Focus on isolated joint movements and gentle stretching.
- Avoid forced or aggressive movements that could compromise healing or stability.
-
Scar Management:
- Begin scar massage once the incision is well-healed to minimize adherence and improve pliability.
- Silicone gel sheeting or topical silicone products may be initiated to reduce hypertrophic scarring.
- Splinting: Continuation of protective splinting, particularly during sleep or high-risk activities, to prevent undesired joint positions or contractures.
Advanced Phase (6 weeks - 3 months and beyond)
-
Strengthening:
- Gradual introduction of strengthening exercises for grip, pinch, and fine motor dexterity, tailored to the child's developmental stage.
- Use age-appropriate toys and activities to engage the child in functional use of the hand.
-
Functional Training:
- Focus on integrating the hand into bimanual activities and activities of daily living (ADLs).
- Specific tasks to improve dexterity, coordination, and proprioception.
-
Monitoring for Deformity:
- Regular clinical and radiographic follow-up is essential, particularly for preaxial polydactyly, to monitor for recurrent angulation, instability, or growth disturbances.
- Growth modulation may be considered in cases of progressive angular deformity.
- Long-Term Follow-up: Continued follow-up into adolescence is crucial to address any potential issues arising from skeletal growth and to ensure optimal long-term functional and cosmetic outcomes.
Summary of Key Literature / Guidelines
The understanding and management of polydactyly have evolved significantly over the past century, with foundational contributions shaping current practice.
- Historical Context: Early descriptions of polydactyly date back centuries, but systematic classification and surgical approaches gained prominence in the mid-20th century. Adrian Flatt, MD , significantly advanced the understanding of congenital hand anomalies, including polydactyly, through his detailed anatomical studies and surgical principles. Wassel's classification of thumb duplication (published in 1969) remains the gold standard, providing a standardized framework for surgical planning and communication.
-
Preaxial Polydactyly (Thumb):
- Current guidelines emphasize the goals of creating a stable, mobile, and well-aligned thumb with good opposition.
- The ablation-reconstruction technique, often involving a wedge osteotomy at the base of the remaining phalanx and careful collateral ligament reconstruction , is preferred for most Wassel types (especially Type IV). This approach has shown superior functional results compared to the Bilhaut-Cloquet procedure in many cases, as it preserves the interphalangeal joint.
- The Bilhaut-Cloquet procedure is reserved for specific scenarios where both duplicated digits are equally small or hypoplastic, and preservation of length and a strong, though fused, digit is prioritized. Studies have indicated potential for growth arrest and nail deformities with this method.
-
Postaxial Polydactyly (Small Finger):
- Type B: Ligation of rudimentary, non-ossified pediculated nubbins remains the standard for selected cases. Guidelines stress careful examination to rule out underlying skeletal elements to prevent neuroma formation.
- Type A: Surgical excision of the more ulnar digit with reconstruction of the abductor digiti minimi tendon and capsuloligamentous structures is the accepted approach. Focus is on preventing splaying and instability of the retained digit.
- Central Polydactyly: Due to its rarity and complexity, there are no single universally accepted guidelines. Management is highly individualized, often requiring a multidisciplinary team approach and staged reconstruction. Principles include maintaining normal digital length, preserving joint motion, and minimizing scar burden, often through on-top plasty or central ray excision.
- Genetic and Embryological Insights: Advances in molecular biology have identified key genes (e.g., SHH , GLI3 , HoxD genes) and signaling pathways (e.g., ZPA) involved in limb patterning. Understanding these mechanisms provides deeper insight into the etiology of polydactyly and its syndromic associations, informing genetic counseling.
- Outcome Assessment: Long-term follow-up studies are critical. Metrics include functional scores (e.g., DASH, ABILHAND), range of motion, grip strength, aesthetic satisfaction, and incidence of complications like angulation and reoperation rates. Reoperation rates for preaxial polydactyly, particularly for angular deformities or instability, remain a recognized challenge.
In conclusion, the management of preaxial and postaxial polydactyly is an evolving field, guided by established classification systems and a continuous refinement of surgical techniques aimed at achieving optimal functional and aesthetic outcomes for affected individuals.
Clinical & Radiographic Imaging

You Might Also Like