Mastering the Posterolateral Approach to the Radial Head
Key Takeaway
Here are the crucial details you must know about Mastering the Posterolateral Approach to the Radial Head. The posterolateral approach to the radial head is a surgical technique for procedures including open reduction, internal fixation of fractures, excision, and prosthetic replacement. This approach to the radial head leverages an internervous plane between the anconeus (radial nerve) and extensor carpi ulnaris (posterior interosseous nerve). Critical landmarks include the lateral humeral epicondyle, and care is taken to avoid posterior interosseous nerve damage.
Posterolateral Approach to the Radial Head
The posterolateral approach to the radial head12 is useful for all surgeries to the radial head. These include open reduction and internal fixation of radial head and neck fractures,13,14 excision of the radial head and insertion of a prosthetic replacement.15,16
Because the incision cannot be extended below the annular ligament without risking damage to the posterior interosseous nerve, avoid extending the incision to the upper part of the radial shaft.
Position of the Patient
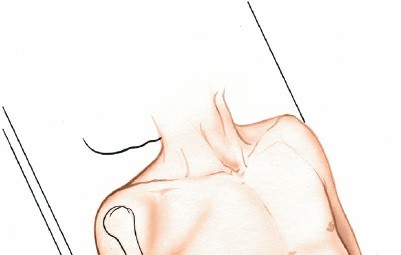
Place the patient supine on the operating table, with the affected arm positioned over the chest. Pronate the forearm.17 Exsanguinate the limb either by applying a soft rubber bandage or an exsanguinator or by elevating it for 3 to 5 minutes. Then, inflate a tourniquet (Fig. 3-38).


Figure 3-38 Position of the patient on the operating table.
Landmarks and Incision
Landmarks
One of the landmarks is the
lateral humeral epicondyle.
To identify the
radial head,
palpate the lateral epicondyle of the humerus, moving the fingers 2.5 cm distally until a depression is detected. The radial head lies deep within this depression. It is palpable through the muscle mass of the wrist extensors. As the forearm is pronated and supinated, movement of the radial head can be felt beneath the surgeon’s fingers. In cases of fracture of the radial head, the normal landmarks are lost because of hemorrhage and swelling. Crepitus at the fracture site often is quite obvious and helpful in placing the incision.
The
olecranon
is the proximal subcutaneous end of the ulna.
Incision
Make a gently curved incision, beginning over the posterior surface of the
lateral humeral epicondyle and continuing downward and medially to a point over the posterior border of the ulna, about 6 cm distal to the tip of the olecranon.
Alternatively, make a 5-cm longitudinal incision based proximally on the lateral humeral epicondyle. This incision follows the skin fold and lies directly over the radial head (Fig. 3-39).
Internervous Plane
The internervous plane lies between the anconeus, which is supplied by the radial nerve, and the extensor carpi ulnaris, which is supplied by the posterior interosseous nerve (Fig. 3-40).


Figure 3-39 Make a longitudinal incision based proximally on the lateral humeral epicondyle.




Figure 3-40 The internervous plane lies between the anconeus (radial nerve) and the extensor carpi ulnaris (posterior interosseous nerve).
Superficial Surgical Dissection
Incise the deep fascia in line with the skin incision. To find the interval between the extensor carpi ulnaris and the anconeus, look distally where the plane is easy to identify; proximally, the two muscles share a common aponeurosis (Fig. 3-41). Detach part of the superior origin of the anconeus as it arises from the lateral epicondyle of the humerus. Then, separate the anconeus and extensor carpi ulnaris muscles, using retractors (Fig. 3-42).
In cases of trauma, there often has been bleeding and contusion in this area, and it is difficult to identify the interval between the extensor carpi ulnaris and anconeus muscles. In this case, it is safe to dissect straight down onto the lateral epicondyle of the humerus, because this structure always can be palpated easily.
Deep Surgical Dissection
Fully pronate the forearm to move the posterior interosseous nerve away from the operative field (see Fig. 3-42,
inset
).
Incise the capsule of the elbow joint longitudinally to reveal the underlying capitulum, the radial head, and the annular ligament. Do not incise the capsule too far anteriorly; the radial nerve runs over the front of the anterolateral portion of the elbow capsule. Do not continue the dissection below the annular ligament or retract vigorously, distally, or anteriorly, because the posterior interosseous nerve lies within the substance of the supinator muscle and is vulnerable to injury (Fig. 3-43).
Dang
Nerves
The posterior interosseous nerve is in no danger as long as the dissection remains proximal to the annular ligament. Pronation of the forearm keeps the nerve as far from the operative field as it possibly can be (see Fig. 3-42,
inset
). To ensure the safety of the nerve, take great care to place the retractors directly on bone and be careful in their placement. Because the posterior interosseous nerve actually may touch the bone of the radial neck, directly opposite the bicipital tuberosity, placing retractors behind it poses a risk.18
The radial nerve is safe as long as the elbow joint is opened laterally and not anteriorly.

Figure 3-41 Find the interval between the extensor carpi ulnaris and the anconeus distally. Proximally, the two muscles merge.


Figure 3-42 Detach the superior origin of the anconeus from the lateral epicondyle, and separate the anconeus and the extensor carpi ulnaris. Pronation of the forearm moves the posterior interosseous nerve medially away from the operative field (
insets
).


Figure 3-43 Incise the joint capsule longitudinally to expose the capitulum and radial head.
How to Enlarge the Approach
Local Measures
For more complete exposure of the lateral half of the distal humerus, extend the superficial dissection by cutting down on the lateral supracondylar ridge. Strip the tissues off subperiosteally both anteriorly and posteriorly to gain access to the distal humerus and to expose the capitulum. Apply a varus force to open up the lateral compartment of the joint. The extension is most useful for fixing fractures internally and for removing loose bodies in the lateral compartment of the elbow (see Anterolateral Approach to the Distal Humerus in Chapter 2).
Extensile Measures
There is no way to extend this approach profitably in any direction.
Posterolateral Approach to the Radial Head
The posterolateral approach to the radial head12 is useful for all surgeries to the radial head. These include open reduction and internal fixation of radial head and neck fractures,13,14 excision of the radial head and insertion of a prosthetic replacement.15,16
Because the incision cannot be extended below the annular ligament without risking damage to the posterior interosseous nerve, avoid extending the incision to the upper part of the radial shaft.
Position of the Patient
Place the patient supine on the operating table, with the affected arm positioned over the chest. Pronate the forearm.17 Exsanguinate the limb either by applying a soft rubber bandage or an exsanguinator or by elevating it for 3 to 5 minutes. Then, inflate a tourniquet (Fig. 3-38).

Figure 3-38
Position of the patient on the operating table.
Landmarks and Incision
### Landmarks
One of the landmarks is the
lateral humeral epicondyle.
To identify the
radial head,
palpate the lateral epicondyle of the humerus, moving the fingers 2.5 cm distally until a depression is detected. The radial head lies deep within this depression. It is palpable through the muscle mass of the wrist extensors. As the forearm is pronated and supinated, movement of the radial head can be felt beneath the surgeon’s fingers. In cases of fracture of the radial head, the normal landmarks are lost because of hemorrhage and swelling. Crepitus at the fracture site often is quite obvious and helpful in placing the incision.
The
olecranon
is the proximal subcutaneous end of the ulna.
Incision
Make a gently curved incision, beginning over the posterior surface of the lateral humeral epicondyle and continuing downward and medially to a point over the posterior border of the ulna, about 6 cm distal to the tip of the olecranon.
Alternatively, make a 5-cm longitudinal incision based proximally on the lateral humeral epicondyle. This incision follows the skin fold and lies directly over the radial head (Fig. 3-39).
Internervous Plane
The internervous plane lies between the anconeus, which is supplied by the radial nerve, and the extensor carpi ulnaris, which is supplied by the posterior interosseous nerve (Fig. 3-40).


Superficial Surgical Dissection
Incise the deep fascia in line with the skin incision. To find the interval between the extensor carpi ulnaris and the anconeus, look distally where the plane is easy to identify; proximally, the two muscles share a common aponeurosis (Fig. 3-41). Detach part of the superior origin of the anconeus as it arises from the lateral epicondyle of the humerus. Then, separate the anconeus and extensor carpi ulnaris muscles, using retractors (Fig. 3-42).
In cases of trauma, there often has been bleeding and contusion in this area, and it is difficult to identify the interval between the extensor carpi ulnaris and anconeus muscles. In this case, it is safe to dissect straight down onto the lateral epicondyle of the humerus, because this structure always can be palpated easily.
Deep Surgical Dissection
Fully pronate the forearm to move the posterior interosseous nerve away from the operative field (see Fig. 3-42,
inset
).
Incise the capsule of the elbow joint longitudinally to reveal the underlying capitulum, the radial head, and the annular ligament. Do not incise the capsule too far anteriorly; the radial nerve runs over the front of the anterolateral portion of the elbow capsule. Do not continue the dissection below the annular ligament or retract vigorously, distally, or anteriorly, because the posterior interosseous nerve lies within the substance of the supinator muscle and is vulnerable to injury (Fig. 3-43).
Dangers
Nerves
The
posterior interosseous nerve
is in no danger as long as the dissection remains proximal to the annular ligament. Pronation of the forearm keeps the nerve as far from the operative field as it possibly can be (see Fig. 342,
inset
). To ensure the safety of the nerve, take great care to place the retractors directly on bone and be careful in their placement. Because the posterior interosseous nerve actually may touch the bone of the radial neck, directly opposite the bicipital tuberosity, placing retractors behind it poses a risk.18
The
radial nerve
is safe as long as the elbow joint is opened laterally and not anteriorly.



For more complete exposure of the lateral half of the distal humerus, extend the superficial dissection by cutting down on the lateral supracondylar ridge. Strip the tissues off subperiosteally both anteriorly and posteriorly to gain access to the distal humerus and to expose the capitulum. Apply a varus force to open up the lateral compartment of the joint. The extension is most useful for fixing fractures internally and for removing loose bodies in the lateral compartment of the elbow (see Anterolateral Approach to the Distal Humerus in Chapter 2).
Extensile Measures
There is no way to extend this approach profitably in any direction.
You Might Also Like