Mastering Athletic Pubalgia: Your Athletic Guide to Recovery
Key Takeaway
We review everything you need to understand about Mastering Athletic Pubalgia: Your Athletic Guide to Recovery. **Athletic pubalgia athletic** refers to a range of chronic groin injuries in athletes, frequently termed sports hernia. This condition involves persistent groin pain caused by a tear in the inguinal floor, often without an obvious hernia. Diagnosis can be challenging due to complex anatomy and coexisting injuries, with symptoms typically lasting months and resisting conservative treatment.
Chapter
28
## Athletic Pubalgia
Jesse C. Botker, Robert F. LaPrade, and David R. Joesting
DEFINITION
1.
Athletic pubalgia refers to a range of groin injuries in athletes. The terms athletic pubalgia and sports hernia sometimes are used interchangeably.
2. Diagnosis of the cause of groin pain is difficult, because the anatomy is complex and two or more injuries may coexist.
1. Intra-abdominal pathology, genitourinary abnormalities, referred lumbosacral pain, and hip joint disorders must first be excluded.
3. Adductor strains are the most common cause of groin pain in athletes.
1. The adductors usually are strained in an eccentric contraction, often one that occurs at the myotendinous junction, but the strain also can occur in the tendon itself or its bony insertion.
2. Other muscles in and around the groin region also can be strained, including the rectus femoris, the sartorius, and the abdominal muscles, as can the conjoint tendon.
4.
Sports hernia is a condition of chronic groin pain that is caused by a tear in the inguinal floor without a clinically obvious hernia.8,12
1. It results in an occult injury that usually is not identified by most examiners. However, with increasing experience, the examiner can feel an abnormal inguinal floor and appreciate abnormal tenderness inside the external ring.
5. In contrast, indirect and direct hernias involve easily palpable defects in the inguinal canal or through the anterior abdominal musculature, respectively.
6. Duration of symptoms typically is months, and pain is resistant to conservative measures.
1.
Osteitis pubis is characterized by symphysis pain and joint disruption and occurs commonly in distance runners and soccer players.
1. It may be difficult to distinguish from adductor strains, and the two conditions may coincide.
2. Stress fractures are rare injuries that result from repetitive cyclic loading of the bone.
1. The pubic rami are the most common location for stress fractures in the pelvis. These fractures are most common in long distance runners.
ANATOMY
3. The anatomy in and around the groin is complex (
FIG 1
), and a thorough understanding of it is crucial in diagnosing the various groin injuries.
1. Thorough knowledge of the origins and insertions is very helpful during examination and palpation of the area.
4. The posterior inguinal wall consists primarily of the transversalis fascia, along with the conjoint tendon, made up of the internal abdominal oblique and transversus abdominis aponeuroses.8

Iliopsoas
Rectus femoris
Adductor longus
Gracilis Sartorius

External oblique muscle
Internal oblique muscle
Transition of the transversus abdominis muscle to
aponeurosis
External inguinal
A ring
Spermatic cord
Transversalis fascia
Deep epigastric vessels
B FIG 1•
Anatomy of the abdominal (
A
) and groin (
B
) musculature.
231

1. The conjoint tendon inserts onto the pubic tubercle and along the iliopubic track.
2. The pubic symphysis is a rigid, nonsynovial, amphiarthro-dial joint consisting of layers of hyaline cartilage encasing a fi-brocartilaginous disc.6
PATHOGENESIS
3. Adductor strains are most commonly seen in soccer or ice hockey players.
1. Most happen acutely, and the patient recalls a sudden intense pain in the groin.
2. Eventually the medial thigh swells and ecchymosis is noted over the next 2 to 3 days.
3. The pain improves when the muscle warms up.
4. Sports hernia is seen in competitive athletes and occasional work injuries and may involve a particular traumatic episode, but most times is insidious and worsens over time with overuse.
1. Patients describe a deep, disabling groin pain.
2. Kicking and endurance running tend to increase the symptoms.
3. Coughing or Valsalva maneuver increases intra-abdominal pressure and can increase tenderness, as can a resisted sit-up.
5. The most likely mechanism for osteitis pubis is that of increased forces placed on the symphysis pubis from the pull of the pelvic musculature or repetitive stress from increased shearing forces.4
1. Some cases of osteitis pubis probably are secondary to or coexist with a sports hernia.
6. Stress fractures of the pubic rami present as an insidious onset of deep pelvic and groin pain that is worsened after high-impact exercises.
1. The pain is worse immediately during and after the activity and improves with rest.
2. These injuries usually occur in conjunction with an acute increase in the intensity of training.
NATURAL HISTORY
7. Acute adductor strains, if not properly rehabilitated, may progress to chronic strains or tendinopathy.
8. Most patients with sports hernia have had a prolonged course of conservative treatment with continued pain and do not get better.17 A hallmark of sports hernias is that patients have less pain when they are inactive and more pain when active.
9. Osteitis pubis is self-limited but may take, on average, about 9 months to heal.5
10. If the stress fracture is not addressed, pain will continue to increase and can be debilitating.
PATIENT HISTORY AND PHYSICAL FINDINGS
11. Patient history is the most important aspect of the evaluation of athletic pubalgia.
12. The patient must be asked for duration of symptoms, any inciting events, relieving and exacerbating factors, and timing of pain.
13. To directly assess for hernia:
1. In men: insert the finger into inguinal ring at level of external opening. Invaginate the loose scrotal skin and gently insert the finger into the external ring (
FIG 2
). Gently feel the inguinal floor and ask the patient to perform the Valsalva maneuver. One can occasionally feel the tear tighten on one’s

FIG 2 • Assessment for inguinal hernia. The finger is inserted into the inguinal ring at the level of the external opening. The loose scrotal skin is invaginated and the finger is gently inserted into the external ring.
fingertip. Apply gentle pressure medially and laterally looking for abnormal asymmetric tenderness.
2. In women: palpate the superior aspect of the labia majora and upward to lateral to the pubic tubercle.
14. The groin is examined using these methods:
1. Straight leg raise: In patients with radicular low back pain, this will reproduce the pain they are having.
2. Palpation of insertion of conjoint tendon: tenderness may increase, and a bulge may be felt by having the patient perform a Valsalva maneuver.
3. Palpation of the adductor tendon: helps to diagnose an adductor strain or tear
4. Groin adduction resistance: helps to diagnose an adductor strain or tear
5. Palpation of the pubic symphysis: characteristic of osteitis pubis
6. Hip range of motion (ROM) may isolate a source of pain arising from the hip.
7. Thomas test: tightness in extension is a sign of a tight iliopsoas muscle.
8. Hip extension against resistance tests the strength of the hip extensors.
9. Hip flexion against resistance: tests the strength of the iliopsoas and may detect a strain or tear of this muscle.
10. Ober’s test: patient inability to lower the upper leg completely to the examination table is pathognomonic of a tight iliotibial band.
IMAGING AND OTHER DIAGNOSTIC STUDIES
15. Radiographs can be helpful in excluding fractures or avul-sions.9
16. Stress fractures usually are not evident on radiographs.
1. Bone scanning or MRI is most sensitive, especially in the early stages.
2. MRI can be used to confirm muscle strain or tears, and partial or complete tendon tears (
FIG 3A
).
1. MRI has been used to detect sports hernias, although it is not always successful.3
3. Dynamic ultrasound has been found, in certain cases, to detect posterior wall defects but is highly operator dependent.16
4. Radiographs, CT scans, and bone scans can rule out other diagnoses; none are reliable in detecting sports hernias.
5. Herniography, which involves an intraperitoneal injection of contrast dye followed by fluoroscopy or radiography, has been shown to identify sports hernias but has limited sensitivity and a substantial risk of perforation in up to 5% of patients.2
6. Osteitis pubis has characteristic radiologic findings, including bone resorption, widening of the pubic symphysis, and irregular contour of articular surfaces or periarticular sclerosis (
FIG 3B
).
1. A bone scan may show increased uptake in the area of the pubic symphysis in osteitis pubis; however, not all patients who have symptoms show an abnormality.13
2. MRI has become increasingly useful in the diagnosis of osteitis pubis. Findings can include bone marrow edema or symphyseal disc extrusion.15
DIFFERENTIAL DIAGNOSIS
7. Groin disruption or strain
8. Osteitis pubis
9. Pelvic stress fractures
10. Indirect and direct hernia
11. Avascular necrosis of the hip
12. Labral tear of the hip
13. Hip osteoarthritis
14. Abdominal muscle tear
15. Lumbar radiculopathy
16. Nerve entrapment
17. Tumors
18. Genitourinary problems
19. Inflammatory bowel disease
20. Endometriosis
21. Pelvic inflammatory disease
NONOPERATIVE MANAGEMENT
1. Acute treatment of adductor strain includes rest, ice, compression, and elevation.
2. The next goal is restoration of ROM and prevention of atrophy. Once the patient can tolerate this, the focus should be to regain strength, flexibility, and endurance.9
3. Nonoperative management of sports hernia includes physical therapy,10 anti-inflammatory drugs, and corticosteroid injections at the site of pain.1
4. Osteitis pubis is a self-limiting condition; therapy should focus on hip ROM, as well as adductor stretching and strengthening.
5. Corticosteroid injection in osteitis pubis is controversial but may be helpful in select populations of athletic pa-tients.11,15
6. Treatment in pelvic stress fractures is straightforward and involves 4 to 6 weeks of rest from the activities aggravating the area.
SURGICAL MANAGEMENT
7. Many approaches have been tried in the surgical management of sports hernias.
8. Tissue repairs require longer rehabilitation and pose a greater risk for recurrence, primarily because of collegenases which are currently being described.
9. Laparoscopic repairs fail too often because they do not deal with the anterior mechanisms of groin pain.
10. Purely anterior repairs fail occasionally because they do not provide adequate posterior support.
11. Mesh repairs are standard.
1. Some mesh repairs fail because the mesh chosen is too heavy and tightly woven.
2. Other mesh repairs fail because of surgical technique (eg, metal tackers, permanent sutures in the periosteum, tight sutures involving nerves and causing necrotic tissue).
3. The most logical and successful repair is the use of two-layered lightweight mesh, which provides both posterior and anterior support and allows normalization of the torn anatomy.





---
A B
### FIG 3 • A. MRI of an adductor tear in a hockey player. There is increased signal at the origin of the adductor tendon near the pubis. B. Characteristic radiograph of osteitis pubis. Notice the bone resorption, widening of the pubic symphysis, and irregular contour of articular surfaces.
Preoperative Planning
1. Preoperative planning involves extreme care to ascertain that the patient really does have the injury for which surgery is being planned. This requires a complete history and physical examination performed by an examiner who understands the pathophysiology of this injury.
2. Imaging is valuable to rule out alternative pathology.
3. Preemptive analgesia is important to reduce postoperative pain and to make the anesthetic experience smoother. Also, local anesthesia is bactericidal, reducing the risk of infection.
1. We suggest 1⁄2% lidocaine with epinephrine and sodium bicarbonate.
Positioning
4. The patient is positioned supine and draped.




---
TECHNIQUES
#### ULTRAPRO HERNIA SYSTEM (JOHNSON & JOHNSON GATEWAY)
Incision, Dissection, and Site Evaluation
1. The incision is made along the path of the inguinal ligament, perhaps 1 cm medial and superior to the ligament. A length of 5 to 6 cm is adequate.
2. Dissection is performed down to the external oblique tying veins. Too much cautery increases the risk of a subcutaneous infection.
3. The external oblique is incised to the external ring, and the fascia is mobilized both medially and laterally.
4. The spermatic cord is carefully evaluated and mobilized, looking for an indirect sac.
5. The inguinal floor is carefully evaluated, looking for a torn transversalis fascia or a torn transversus abdominis.
1. Occasionally, the yellow preperitoneal fat can be seen outlining a tear.
6. The inguinal floor is palpated. The disruption often can be felt.
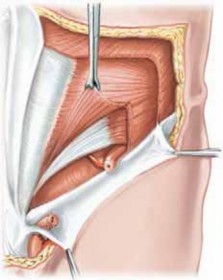
A B C D
TECH FIG 1 • A,B. The anterior pocket is developed under the external oblique to optimize placement of the onlay patch and dissected out laterally to ensure the onlay patch will lie flat. C. After the posterior wall has been opened, visual confirmation is made of location in the preperitoneal space by identifying the yellow preperitoneal fat and by visualizing Cooper’s ligament. D. Then, using the forefinger, sweep circumferentially medial, then lateral to actualize the preperitoneal space.
(continued)


TECHNIQUES E F TECH FIG 1 • (continued) E,F. With the onlay patch grasped down to the connector with sponge forceps, insert the device completely into the defect and deploy the underlay with forceps or finger. (Courtesy of Ethicon Surgery, a Johnson & Johnson company.) Positioning the Patches 1. The preperitoneal space is opened and prepared. Dissection is extended out laterally so the onlay patch will lie flat (TECH FIG 1A,B).
- It should be possible to clearly feel under the rectus, the pubis, Cooper’s ligament, and up along the il-iofemoral vessels ( TECH FIG 1C,D ).
- The posterior (round) patch of the UHSL is positioned in the space that has been prepared ( TECH FIG 1E,F ).
- The transversalis and transversus abdominis are closed around the connector with an absorbable suture tied loosely (an air knot). The technique is evolving, and in the near future, the mesh probably will be attached with tissue glue. Affixing the Patches 7. The onlay patch is attached to the fascia overlying the pubic tubercle, to the internal oblique fascia medially and to the iliopubic track laterally.
- A lateral slit is made in the mesh for the spermatic cord, attaching the mesh to the shelving edge of the inguinal ligament. Excess mesh is trimmed away.
- The mesh should never be tight, and fewer sutures are better than many, as long as the mesh is anatom-ically placed ( TECH FIG 2A–C ).
-
Marcaine is injected thoroughly, and the external oblique, Scarpa’s fascia, and skin are clsoed with an absorbable suture (
TECH FIG 2D,E
).



--- B A TECH FIG 2 • A,B. Sutures are used to fixate the onlay patch over the pubic tubercle (essential) and to the mid-portion of the transverse aponeurotic arch (optional). A slit is created in the onlay patch to accommodate the spermatic cord, and the mesh is sutured to close the slit. C. The spermatic cord comes through the onlay patch. (continued) C
--- PEARLS AND PITFALLS Operate only if the patient has a good mechanism of injury, a good history, and clear indications on physical examination.
Tight sutures, tacks, or tight mesh may cause chronic postoperative pain.
The principle of this surgery (and all abdominal wall hernia surgery) is to normalize the tissue and reinforce the normalized tissue with lightweight, flexible mesh. - If the patient’s pain does not improve with rest, he or she probably does not have a sports hernia.
-
For the best results, both the anterior and posterior mechanisms of pain must be addressed.
PHS coverage of the MPO
Anterior superior iliac spine
Pubic tubercle Direct hernia PHSE depicted Onlay: length – 12.5 cm
width – 5.5 cm Underlay: diameter – 10.0 cm





--- E D TECH FIG 2 • (continued) D. Schematic drawing of where the patch will lie. E. Finished position of the mesh. (Courtesy of Ethicon Surgery, a Johnson & Johnson company.) 13.5 cm
TECHNIQUES POSTOPERATIVE CARE 9. Standard post–inguinal hernia surgery care is advised.
- It is important to emphasize a rapid return to normal non-physical activity (starting the day after surgery) and a progressive incremental return to sports and working out in preparation for sports. This is best accomplished with the help of a trainer.
- The goal of rehabilitation is to establish a full and normal ROM and flexibility followed by incremental increases in re-sistence for strength training.
- Contact athletes should be able to return to competition in 3 to 4 weeks.
- Runners should be running in 2 weeks and golfers golfing in 1 week. OUTCOMES 14. With appropriate indications and surgical technique, success rates in sports hernia repair have been as high as 97% to 100% in high-performance athletes, with success measured as a return to previous levels of performance and freedom from pain.7,14 COMPLICATIONS 15. Recurrence
- Thigh pain in the early postoperative period
- Infection
- Hematoma
- Continued pain**
Scientific References
-
**
- 1. Ashby EC. Chronic obscure groin pain is commonly caused by enthe-sopathy: “tennis elbow” of the groin. Br J Surg 1994;81:1632–1634. [View Source / PubMed]
- 2. Calder F, Evans R, Neilson D. Value of herniography in the management of occult hernia and groin pain in adults. Br J Surg 2000;87: 824–825. [View Source / PubMed]
- 3. Ekberg O, Sjoberg S, Westlin N. Sports-related groin pain: evaluation with MR imaging. Eur Radiology 1996;6:52–55. [View Source / PubMed]
- 4. Fricker P. Osteitis pubis. Sports Med Arthroscopy Rev 1997;5: 305–312. [View Source / PubMed]
- 5. Fricker P, Taunton J, Ammann W. Osteitis pubis in athletes. Infection, inflammation or injury? Sports Med 1991;12:266–279. [View Source / PubMed]
- 6. Gamble J, Simmons S, Freedman M. The symphysis pubis: anatomic and pathologic considerations. Clin Orthop Relat Res 1986;203: 261–272. [View Source / PubMed]
- 7. Genitsaris M, Goulimaris I, Sikas N. Laparoscopic repair of groin pain in athletes. Am J Sports Med 2004;32:1238–1242. [View Source / PubMed]
- 8. Hackney RG. The sports hernia: a cause of chronic groin pain. Br J Sports Med 1993;27:58–62. [View Source / PubMed]
- 9. Holmich P. Adductor related groin pain in athletes. Sports Med Arthroscopy Rev 1997;5:285–291. [View Source / PubMed]
- 10. Holmich P, Uhrskou P, Ulnits L, et al. Effectiveness of active physical training as treatment for longstanding adductor-related groin pain in athletes. The Lancet 1999;353:439–443. [View Source / PubMed]
- 11. Holt M, Keene J, Graf B, et al. Treatment of osteitis pubis in athletes. Results of corticosteroid injections. Am J Sports Med 1995;23: 601–606. [View Source / PubMed]
- 12. Joesting DR. Diagnosis and treatment of sportsman’s hernia. Curr Sports Med Rep 2002;1:121–124. [View Source / PubMed]
- 13. Karlsson J, Jerre R. The use of radiography, magnetic resonance, and ultrasound in the diagnosis of hip, pelvis, and groin injuries. Sports Med Arthroscopy Rev 1997;5:268–273. [View Source / PubMed]
- 14. Meyers WC, Foley DP, Garrett WE, et al. Management of severe lower abdominal or inguinal pain in high-performance athletes. Am J Sports Med 2000;28:2–8. [View Source / PubMed]
- 15. O’Connell M, Powell T, McCaffrey N. Symphyseal cleft injection in the diagnosis and treatment of osteitis pubis in athletes. Am J Roentgenol 2002;179:955–959. [View Source / PubMed]
- 16. Orchard JW, Read JW, Neophyton J. Groin pain associated with ultrasound finding of inguinal canal posterior wall deficiency in Australian Rules footballers. Br J Sports Med 1998;32:134–139. [View Source / PubMed]
- 17. Taylor DC, Meyers WC, Moylan JA. Abdominal musculature abnormalities as a cause of groin pain in athletes. Inguinal hernias and pubalgia. Am J Sports Med 1991;19:239–242. [View Source / PubMed]
You Might Also Like


