Medial Meniscectomy: A Comprehensive Academic Review of Anatomy, Biomechanics & Surgical Approaches
Key Takeaway
Medial meniscectomy is a surgical procedure to remove irreparable medial meniscal tissue, typically arthroscopically. It's crucial for relieving symptoms like pain and mechanical locking. A deep understanding of medial meniscus anatomy, biomechanics, and vascularity is paramount to preserve as much functional tissue as possible, mitigating long-term risks of osteoarthritis and optimizing patient outcomes.
Optimizing Your Approach for Medial Meniscectomy Success
Introduction & Epidemiology
Meniscal pathology represents a highly prevalent orthopedic condition, frequently leading to pain, mechanical symptoms, and functional impairment of the knee joint. The medial meniscus, due to its anatomical fixation and biomechanical role, is more susceptible to injury than its lateral counterpart. Historically, treatment for symptomatic meniscal tears involved total meniscectomy via an open arthrotomy, which, while alleviating immediate symptoms, was later understood to contribute significantly to accelerated degenerative joint disease and osteoarthritis due to the critical load-bearing and shock-absorbing functions of the meniscus.
The advent of arthroscopic surgery revolutionized meniscal management, shifting the paradigm from total to partial meniscectomy, and subsequently, to meniscal repair where feasible. Arthroscopic partial meniscectomy (APM) is currently considered the gold standard for excising irreparable symptomatic meniscal tissue, aiming to preserve as much functional meniscal tissue as possible while relieving mechanical symptoms. Despite the overwhelming predominance of arthroscopic techniques, the open approach to medial meniscectomy, as detailed in the provided seed content, retains a niche utility in specific scenarios, particularly in regions with limited access to arthroscopic equipment or for highly complex cases that may benefit from direct visualization and manipulation.
Epidemiologically, meniscal tears affect a wide demographic. Traumatic tears are common in younger, active individuals, often associated with sports injuries involving twisting forces on a flexed knee. Degenerative tears, conversely, are more prevalent in older populations, arising from repetitive microtrauma to increasingly brittle meniscal tissue, often in the absence of a distinct traumatic event. The annual incidence of meniscal tears is estimated to be approximately 60-70 cases per 100,000 individuals, with males more frequently affected than females. Medial meniscal tears occur roughly 2-3 times more often than lateral tears. Understanding the nuances of meniscal anatomy, tear patterns, and the appropriate surgical approach is paramount to optimizing patient outcomes and mitigating long-term sequelae.
Surgical Anatomy & Biomechanics
A thorough understanding of the medial meniscus's anatomy and biomechanics is fundamental to successful meniscectomy and the preservation of long-term knee joint health.
Gross Anatomy of the Medial Meniscus
The medial meniscus is a C-shaped, semilunar fibrocartilaginous structure that resides on the medial tibial plateau, acting as an interface between the femoral condyle and the tibial plateau. It is broader posteriorly than anteriorly.
- Anterior Horn: Attaches to the anterior intercondylar area of the tibia, anterior to the attachment of the anterior cruciate ligament (ACL). It is also connected to the lateral meniscus via the transverse ligament in approximately 30-40% of individuals.
- Body: The central portion, relatively immobile due to its firm attachment to the deep fibers of the medial collateral ligament (MCL) and the joint capsule via the coronary (meniscotibial) ligaments. This firm attachment, in contrast to the more mobile lateral meniscus, contributes to its higher incidence of tears, particularly in conjunction with MCL injuries.
- Posterior Horn: The broadest part, attaching firmly to the posterior intercondylar area of the tibia, anterior to the posterior cruciate ligament (PCL) insertion. It also has a strong attachment to the semimembranosus muscle tendon, which exerts a posterior pull on the meniscus during knee flexion, potentially influencing its stability and tear patterns.
Vascularity and Innervation
The peripheral 10-30% of the meniscus receives a direct blood supply from the perimeniscal capillary plexus, derived from the genicular arteries. This "red-red" zone has potential for healing. Moving centrally, the meniscus transitions to a "red-white" zone with diminishing vascularity, and the innermost two-thirds is avascular, known as the "white-white" zone, which has minimal intrinsic healing capacity. This vascular distribution significantly influences the decision between meniscal repair and meniscectomy.
Innervation is provided by articular branches from the tibial and obturator nerves, contributing to proprioception and nociception.
Biomechanics
The menisci perform several critical functions:
- Load Transmission and Shock Absorption: The menisci convert axial compressive loads into circumferential hoop stresses, distributing them over a larger surface area of the articular cartilage. They transmit approximately 50% of the compressive load in extension and up to 85% in 90 degrees of flexion. Total meniscectomy has been shown to increase tibiofemoral contact stresses by 100-200%, leading to accelerated articular cartilage degeneration. Partial meniscectomy also increases contact stresses, albeit to a lesser degree, highlighting the importance of preserving as much viable meniscal tissue as possible.
- Joint Stability: The menisci contribute to secondary stability, particularly in an ACL-deficient knee, and limit anterior-posterior translation of the tibia relative to the femur. The medial meniscus's firm attachment to the MCL contributes to medial knee stability.
- Joint Lubrication and Nutrition: They facilitate the distribution of synovial fluid and chondrocyte nutrition.
- Proprioception: Sensory receptors within the meniscal horns contribute to proprioceptive feedback, aiding neuromuscular control of the knee.
Understanding these biomechanical consequences underscores the imperative to perform the most conservative possible meniscectomy, excising only the irreparable symptomatic portion of the meniscus, to mitigate the risk of post-meniscectomy syndrome and progressive osteoarthritis.
Indications & Contraindications
The decision to proceed with medial meniscectomy is based on a comprehensive assessment of patient symptoms, physical examination findings, imaging, and an understanding of the natural history of meniscal tears. The primary goal is to alleviate mechanical symptoms and pain caused by unstable meniscal tissue that cannot be repaired.
Indications for Medial Meniscectomy
-
Symptomatic Unstable Meniscal Tears:
- Mechanical Symptoms: Locking, catching, recurrent effusions, giving way. These are often the most compelling indications, suggesting an unstable meniscal fragment impinging on joint motion.
- Pain: Persistent, localized joint line pain unresponsive to adequate non-operative management.
- Tear Patterns: Irreparable complex tears, flap tears, radial tears, bucket-handle tears where the displaced fragment is non-reducible or necrotic, and degenerative tears causing mechanical symptoms or significant pain without substantial osteoarthritis.
- Failed Meniscal Repair: Tears that were initially repaired but subsequently failed, resulting in recurrent symptoms.
- Removal of Loose Bodies or Foreign Bodies: While less common for the meniscus itself, the anteromedial approach provides access for removal of intra-articular loose bodies or foreign bodies. As noted in the seed content, "The uses of the anteromedial approach include the following: *** Medial meniscectomy * Partial meniscectomy * Removal of loose bodies * Removal of foreign bodies *".
Contraindications for Medial Meniscectomy
- Asymptomatic Meniscal Tears: Tears discovered incidentally on imaging in the absence of pain or mechanical symptoms.
- Stable Meniscal Tears: Tears that are stable on probing during diagnostic arthroscopy and do not cause mechanical symptoms.
- Tears amenable to repair: Peripheral tears in the red-red or red-white zone, longitudinal tears, and specific radial tears that can be approximated and sutured.
- Significant Osteoarthritis: In cases of advanced tibiofemoral osteoarthritis, meniscal symptoms may be secondary to the arthritic process. Meniscectomy in this setting rarely provides lasting relief and may even accelerate progression. Arthroplasty or osteotomy may be more appropriate considerations.
- Active Infection: Absolute contraindication. Any active infection, local or systemic, must be treated prior to elective surgery.
- Uncorrectable Coagulopathy: Increased risk of bleeding complications.
- Patient Inability to Participate in Rehabilitation: While partial meniscectomy rehabilitation is less intensive than repair, a baseline level of compliance is required for optimal recovery.
Operative vs. Non-Operative Indications
| Indication Category | Operative Management (Meniscectomy/Repair) | Non-Operative Management (Initial/Definitive) |
|---|---|---|
| Meniscal Tears | Symptomatic, mechanically unstable tears (locking, catching, giving way, persistent pain) | Asymptomatic tears, stable tears, minor tears, degenerative tears without mechanical symptoms, tears in avascular zones where repair is contraindicated. |
| Pain Level | Moderate to severe pain, unresponsive to conservative treatment | Mild pain, intermittent pain, pain controlled with activity modification and analgesics. |
| Mechanical Symptoms | Present (locking, catching, pseudolocking) | Absent or easily managed with activity modification. |
| Degenerative Changes | Mild to moderate osteoarthritis without global joint-line pain | Severe tibiofemoral osteoarthritis (consider arthroplasty as definitive treatment). |
| Tear Characteristics | Flap tears, complex tears, radial tears where repair is not feasible, displaced bucket-handle tears, traumatic tears in younger active patients. | Stable peripheral tears, small longitudinal tears (especially in older patients), degenerative tears without mechanical symptoms. |
| Associated Pathology | Loose bodies, foreign bodies causing impingement or symptoms. | No associated pathology requiring surgical intervention. |
| Patient Factors | Active individuals desiring return to sport/high-demand activities, compliant with rehabilitation. | Sedentary individuals, elderly patients, patients with significant comorbidities precluding surgery, non-compliant with rehabilitation. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for optimizing surgical exposure, minimizing complications, and ensuring procedural success, whether via arthroscopic or open technique.
Pre-Operative Assessment
- Clinical Evaluation: A detailed history focusing on the mechanism of injury, onset and nature of symptoms (pain, locking, clicking, effusion), and response to previous conservative measures. Physical examination should thoroughly assess joint line tenderness, range of motion, effusion, and ligamentous stability (Lachman, anterior drawer, posterior drawer, varus/valgus stress tests) to identify any associated injuries.
-
Imaging:
- Plain Radiographs: Weight-bearing anteroposterior, lateral, and Merchant views are essential to assess for existing degenerative changes, osteophytes, and joint space narrowing, which may contraindicate isolated meniscectomy.
- Magnetic Resonance Imaging (MRI): The gold standard for confirming meniscal tears, evaluating tear type and location, and identifying concomitant pathology (ligamentous injuries, chondral lesions, bone bruising).
- Informed Consent: Thorough discussion with the patient regarding the diagnosis, proposed procedure (partial meniscectomy), alternatives (conservative management, repair), potential risks (infection, nerve injury, persistent symptoms, progression of arthritis), and expected rehabilitation course.
Anesthesia
Regional anesthesia (spinal or epidural) with sedation, or general anesthesia, are common choices. A femoral nerve block or adductor canal block may be employed as an adjunct for post-operative pain control.
Patient Positioning
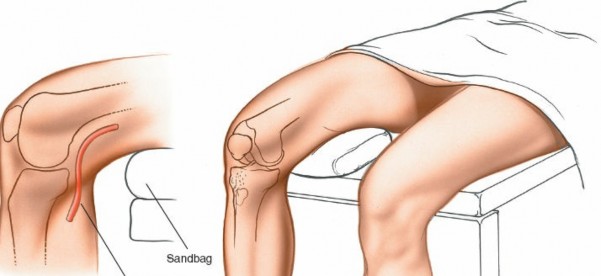
The patient is typically placed in a supine position on the operating table.
- Supine Position: Allows for easy access to the medial compartment of the knee.
- Leg Holder or Bolster: For arthroscopic procedures, a well-padded leg holder often secures the thigh, allowing the lower leg to hang freely. Alternatively, a foam bolster beneath the distal femur permits knee flexion while maintaining stability.
- Flexion Capability for Open Approach: As highlighted in the seed content, for an open medial meniscectomy, "Remove the end of the table so that the knee can be flexed beyond a right angle." This maneuver, often aided by an assistant holding the foot, is crucial for gaining optimal visualization and access to the posterior horn of the medial meniscus. Maintaining the knee in hyperflexion while applying a valgus stress and external rotation of the tibia opens the medial compartment and exposes the posterior structures.
- Tourniquet Application: "Exsanguinate the limb by elevating it for 2 to 5 minutes or by applying a soft rubber bandage. Then, inflate a tourniquet." A pneumatic tourniquet is routinely applied to the proximal thigh after limb exsanguination (either by elevation or Esmarch bandage) to ensure a bloodless field, which is particularly important for direct visualization during an open procedure. Tourniquet pressure should be individualized, typically 50-100 mmHg above systolic blood pressure, and closely monitored to limit ischemia time.
- Limb Preparation: Standard sterile surgical preparation and draping are performed, exposing the entire knee from the mid-thigh to the mid-calf.
- Lighting: "This position requires good lighting so that the meniscus can be seen during surgery. The light must be adjusted continually to keep it shining directly into the depths of the wound. A headlamp is the best light source." This emphasizes the importance of direct and adjustable illumination in an open procedure, which is not as critical with arthroscopic light sources. A surgical headlamp provides focused, shadow-free illumination within the deep confines of an open arthrotomy.
Detailed Surgical Approach / Technique
While arthroscopic partial meniscectomy (APM) is the prevailing standard for medial meniscectomy, the discussion below will first outline the principles of APM, followed by a detailed description of the open medial meniscectomy approach, as emphasized by the seed content, acknowledging its utility in specific contexts.
Arthroscopic Partial Meniscectomy (APM) – The Modern Standard
-
Portal Placement:
- Anterolateral Portal: Primary viewing portal, approximately 1 cm lateral to the patellar tendon, just superior to the joint line.
- Anteromedial Portal: Primary working portal, approximately 1 cm medial to the patellar tendon, just superior to the joint line. A needle is typically used to localize the ideal entry point under arthroscopic visualization to avoid damaging articular cartilage.
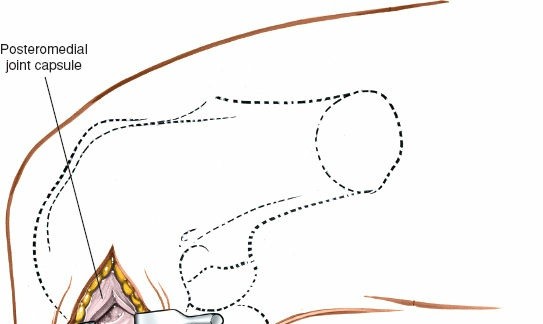
- Posteromedial Portal: An accessory portal, located posterior to the medial collateral ligament (MCL) at the level of the joint line, can be useful for visualization and instrumentation of complex posterior horn tears, particularly those extending into the meniscocapsular junction.
- Diagnostic Arthroscopy: A comprehensive systemic evaluation of all knee compartments (patellofemoral, medial tibiofemoral, lateral tibiofemoral, intercondylar notch) is performed using the arthroscope. This assesses the menisci, articular cartilage, ligaments, and synovium, and identifies any associated pathology.
-
Meniscal Evaluation and Resection:
- The medial meniscus is thoroughly probed to assess tear pattern, stability, and extent. Unstable fragments that cause mechanical symptoms are identified.
- The goal is to resect only the unstable, symptomatic portion of the meniscus while preserving as much healthy meniscal tissue as possible to maintain function.
- Specialized arthroscopic instruments, including basket forceps, meniscus knives, and motorized shavers, are used to excise the torn fragment.
- The remaining meniscal rim is then contoured and smoothed with a shaver to remove any unstable tags or rough edges that could cause continued irritation. The final rim should be stable to probing.
- Closure: Arthroscopic portals are typically closed with a single suture or sterile strips. Sterile dressings are applied.
Open Medial Meniscectomy – The Specific Approach
The open medial meniscectomy, once the standard, is now reserved for scenarios where arthroscopy is unavailable, technically infeasible (e.g., severe arthrofibrosis, large foreign bodies, or specific revision surgeries), or for very large, difficult-to-manage loose bodies. The seed content heavily focuses on this approach.
-
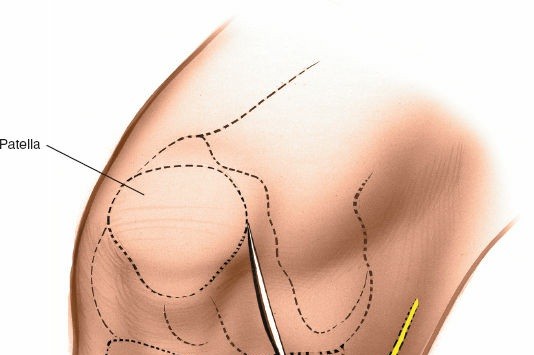
Landmarks and Incision:
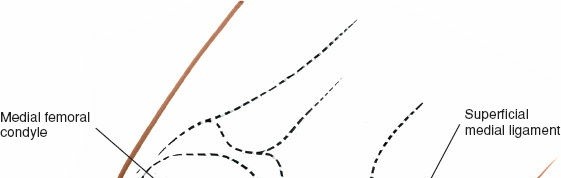
- Landmarks: Palpate the medial joint line, medial epicondyle of the femur, and medial tibial plateau. The saphenous vein and nerve courses superficial and posterior to the medial femoral condyle, requiring careful attention.
-
Incision Options (as per seed content):
- Transverse Skin Incision: "over the joint line; although this limits the view of the knee, it provides better access to the meniscus itself." This may be suitable for isolated, easily accessible mid-body tears.
- Longitudinal or Oblique Incisions: "offer a better view of such other intra-articular structures as the cruciate ligaments." These incisions provide broader exposure and are generally preferred for better visualization of the entire meniscus and other intra-articular structures. A paramedial, slightly curved longitudinal incision, approximately 5-7 cm in length, centered over the joint line, is a common choice. It extends from just above the joint line distally to just below.
- The choice of incision depends on surgeon preference and the specific pathology being addressed.
-
 -

-
Dissection:
- Skin and Subcutaneous Tissue: Incise the skin and subcutaneous tissue. Meticulous hemostasis is maintained.
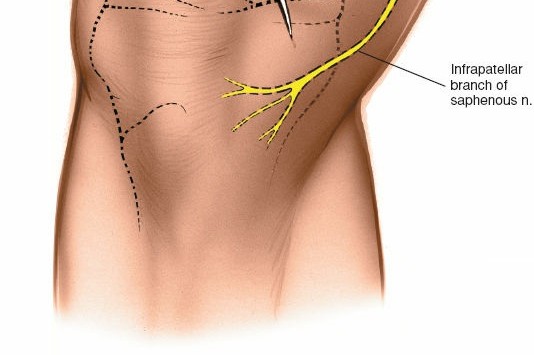
- Saphenous Nerve and Vein: Careful dissection is paramount to identify and protect the infrapatellar branch of the saphenous nerve and the greater saphenous vein, which lie within the subcutaneous fat layer. Retract them carefully.
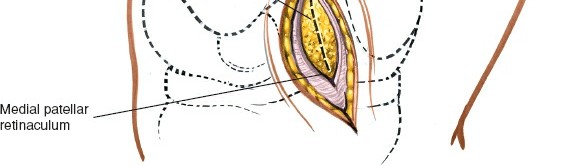
- Deep Fascia: Incise the deep fascia.
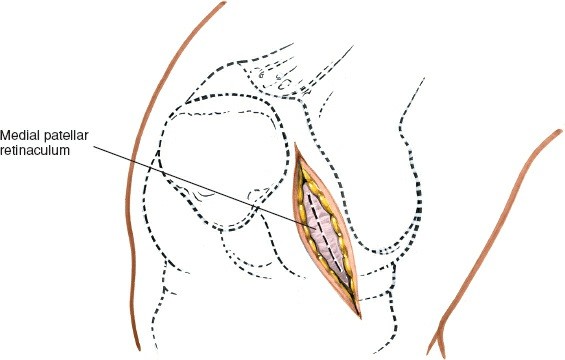
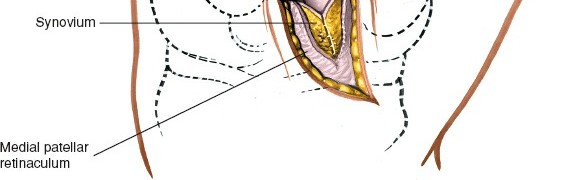
- Joint Capsule: The approach typically involves either a medial parapatellar arthrotomy, splitting the fibers of the vastus medialis obliquus (VMO) longitudinally, or a direct incision of the medial capsule over the joint line, medial to the patellar tendon. For direct access to the medial meniscus, a paramedial capsular incision along the medial border of the patella and extending distally can be made.
-
 -
-
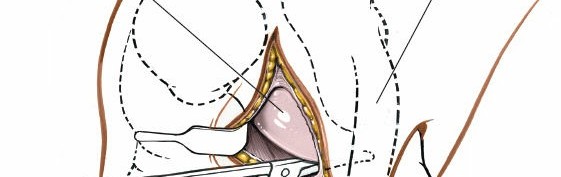
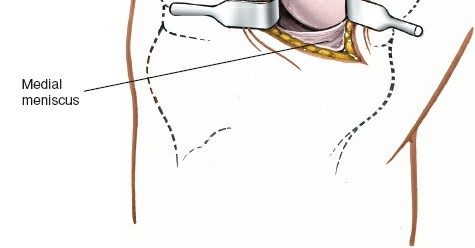
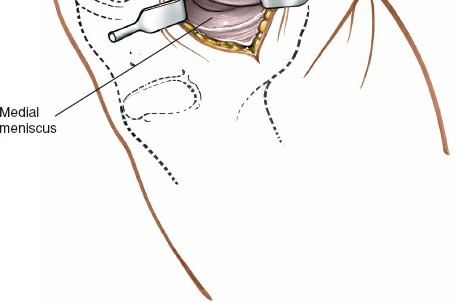
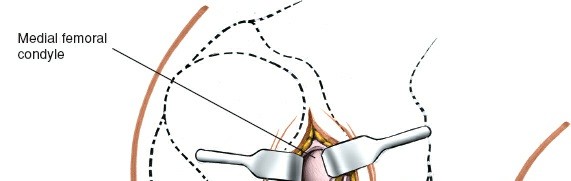
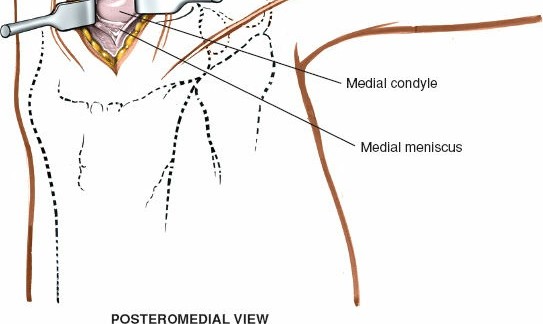
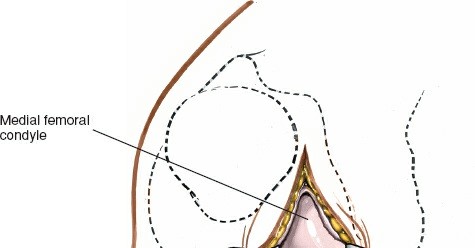
Exposure of the Meniscus:
- Retractors are carefully placed to expose the medial tibiofemoral compartment. Self-retaining retractors may be used, but care must be taken to protect the articular cartilage.
- To improve visualization, the knee is brought into hyperflexion (as per seed content, "beyond a right angle"). This maneuver, combined with external rotation of the tibia and a valgus stress applied to the knee, widens the medial compartment. This allows for improved access to the posterior horn of the medial meniscus.
-
 -

-
Meniscectomy Technique (Partial):
- Inspection: Thoroughly inspect the medial meniscus to identify the tear pattern and assess its stability using a blunt probe.
- Resection: The goal is partial meniscectomy, removing only the unstable, symptomatic fragment. Total meniscectomy is strongly discouraged due to long-term sequelae.
- Specialized meniscal knives (e.g., banana knife, hook knife) are used to make precise cuts, detaching the torn fragment from the stable meniscal rim and meniscocapsular junction.
- Small rongeurs or basket forceps are then used to excise the torn portion.
- The remaining meniscal edge is carefully contoured and smoothed to prevent any residual tags from impinging or causing further irritation.
-
 -
 -
 -
 -
 -
 -
 -
 -
 - "Removal of loose bodies" and "Removal of foreign bodies" are also performed at this stage if identified, utilizing the direct visualization offered by the open approach.
-
Closure:
- Irrigate the joint thoroughly.
- Carefully repair the joint capsule and deep fascia using absorbable sutures. This helps restore joint stability and minimize synovial fluid leakage.
- Close the subcutaneous tissue layer.
- Close the skin with non-absorbable sutures or staples.
- A sterile dressing is applied. Drainage is typically not necessary for uncomplicated partial meniscectomy but may be considered if significant bleeding is encountered or with a larger arthrotomy.
-
 -
 -
Complications & Management
While medial meniscectomy is generally considered a safe procedure, potential complications can arise, requiring prompt recognition and appropriate management.
General Surgical Complications
-
Infection:
- Incidence: Superficial infection (0.5-2%), deep infection (0.1-0.5%).
- Management: Superficial infections often respond to oral antibiotics and local wound care. Deep infections (septic arthritis) are surgical emergencies requiring urgent arthroscopic irrigation and debridement, synovial fluid culture, and targeted intravenous antibiotics.
-
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
- Incidence: DVT (0.1-1%), PE (<0.1%).
- Management: Prophylaxis with early mobilization is standard. Suspected DVT requires ultrasound; PE requires CT angiography. Treatment involves anticoagulation.
-
Nerve Injury:
- Incidence: <1%. Primarily involving the infrapatellar branch of the saphenous nerve, causing paresthesia, numbness, or neuropathic pain in the anteromedial knee.
- Management: Usually temporary. Neuropathic pain may be managed with medications. Rarely, neuroma formation may require surgical excision.
-
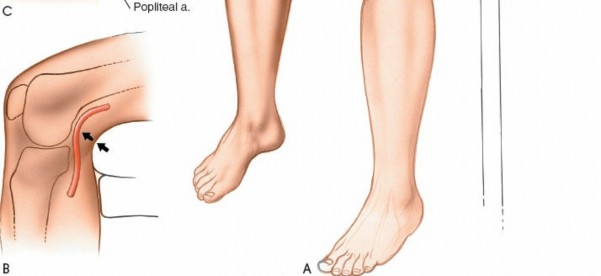
Vascular Injury:
- Incidence: Extremely rare (<0.01%). Damage to the popliteal artery or its branches.
- Management: Urgent vascular surgical consultation and repair.
-
Arthrofibrosis:
- Incidence: Varies, generally low for isolated meniscectomy, higher with concomitant procedures or inflammatory response.
- Management: Intensive physiotherapy, manipulation under anesthesia, or arthroscopic lysis of adhesions.
-
Complex Regional Pain Syndrome (CRPS) / Reflex Sympathetic Dystrophy (RSD):
- Incidence: Rare.
- Management: Early recognition, multidisciplinary pain management, physical therapy, sympathetic blocks.
Meniscectomy-Specific Complications
-
Persistent Symptoms / Incomplete Resection:
- Incidence: Varies widely, depending on original pathology and surgical technique (5-15%). Can result from an unstable meniscal fragment left behind, an undiagnosed concomitant injury, or progression of underlying arthritis.
- Management: Re-evaluation with MRI, diagnostic injections, and potentially revision arthroscopy or other targeted interventions.
-
Meniscal Reteart:
- Incidence: Rare following partial meniscectomy of the same area (0.5-2%). More common if insufficient resection of unstable tissue was performed or a new injury occurs.
- Management: If symptomatic, similar to initial tear management (conservative or revision meniscectomy/repair).
-
Accelerated Articular Cartilage Degeneration / Osteoarthritis:
- Incidence: Long-term risk, universally acknowledged with meniscectomy. Severity correlates with the amount of resected tissue. Known as "post-meniscectomy syndrome."
- Management: Symptomatic management of OA (conservative measures, injections, activity modification). In severe cases, osteotomy or arthroplasty may be considered.
-
Fluid Extravasation (Arthroscopic Specific):
- Incidence: Uncommon with appropriate pump pressures.
- Management: Cease irrigation, external compression, and monitoring. In severe cases, compartment syndrome can occur, requiring fasciotomy.
Complications and Management Table
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Infection | 0.1-2% | Oral/IV antibiotics (superficial); Urgent arthroscopic irrigation & debridement + IV antibiotics (deep/septic arthritis). |
| DVT/PE | 0.1-1% | Early mobilization, anticoagulation, graduated compression stockings (prophylaxis); Anticoagulation (treatment). |
| Nerve Injury (Saphenous Nerve) | <1% | Conservative management (paresthesia); Neuropathic pain medications; rarely surgical excision of neuroma. |
| Vascular Injury | <0.01% | Urgent vascular surgical consultation and repair. |
| Arthrofibrosis | Low | Intensive physical therapy, manipulation under anesthesia, arthroscopic lysis of adhesions. |
| Persistent Symptoms | 5-15% | Diagnostic imaging (MRI), selective injections, revision arthroscopy for residual unstable tissue, addressing concomitant pathology, or conservative management for post-meniscectomy pain/OA. |
| Accelerated OA/Post-Meniscectomy | Universal (long-term) | Conservative management (PT, NSAIDs, injections, bracing), activity modification; potentially osteotomy or arthroplasty in advanced cases. |
| Fluid Extravasation | <1% (arthroscopic) | Cessation of fluid inflow, external compression; rarely fasciotomy for compartment syndrome. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following medial meniscectomy, particularly partial meniscectomy, is typically accelerated compared to meniscal repair, reflecting the stability created by the surgical excision of unstable tissue. The primary goals are to control pain and swelling, restore full range of motion, regain muscle strength and proprioception, and facilitate a safe return to activities.
Phase I: Immediate Post-Operative (Days 0-7)
- Goals: Pain and swelling control, protect healing tissues, initiate early range of motion (ROM), minimize muscle atrophy.
- Weight-Bearing: Full weight-bearing as tolerated (FWBAT) with crutches for balance and comfort is generally permitted immediately after partial meniscectomy.
- Cryotherapy and Compression: Consistent application of ice and compression (e.g., knee brace, elastic bandage) to manage swelling and pain.
- Elevation: Keep the leg elevated above heart level.
- Medication: Analgesics as prescribed.
-
Range of Motion:
- Gentle passive and active-assisted ROM exercises to achieve full extension and progress flexion as tolerated.
- Heel slides, prone knee flexion.
-
Strengthening:
- Quadriceps setting exercises (quad sets).
- Straight leg raises (SLR) in multiple planes.
- Ankle pumps to prevent DVT.
- Gluteal sets.
Phase II: Early Rehabilitation (Weeks 1-6)
- Goals: Restore full, pain-free ROM, improve strength and neuromuscular control, progress weight-bearing tolerance.
- Weight-Bearing: Discontinue crutches once gait is normalized and pain-free.
- Range of Motion: Continue to work towards achieving full knee extension and flexion.
-
Strengthening:
- Progression of closed-chain exercises: mini-squats, wall slides, leg presses.
- Open-chain exercises (e.g., knee extension, hamstring curls) can be introduced cautiously.
- Hip abduction/adduction strengthening.
- Balance and proprioception exercises: single leg stance, wobble board.
- Cardiovascular: Low-impact activities such as stationary cycling, swimming (if incisions are healed), or elliptical training can begin.
Phase III: Advanced Rehabilitation & Return to Activity (Weeks 6-12+)
- Goals: Maximize strength, power, and endurance; restore sport-specific or activity-specific function; gradual return to impact activities.
-
Strength and Power:
- Progress resistance in all exercises.
- Introduce plyometric exercises (e.g., box jumps, hopping) as appropriate.
- Sport-specific drills (e.g., cutting, pivoting, running progressions).
- Agility and Proprioception: Advanced balance and agility drills.
- Return to Activity/Sport: A progressive return-to-sport protocol is followed, ensuring adequate strength, balance, and confidence. This decision is individualized and based on functional testing and the absence of pain or swelling. Typically, return to high-impact sports can be anticipated around 3-6 months, though many patients return to daily activities much sooner.
Considerations for Open vs. Arthroscopic Approaches
While the fundamental rehabilitation principles remain similar, patients undergoing open meniscectomy may initially experience:
*
Increased pain and swelling:
Due to the larger incision and greater tissue dissection.
*
Slower initial ROM progression:
Due to soft tissue healing and potential stiffness.
*
Greater focus on wound care:
Given the larger incision.
However, the functional outcomes for partial meniscectomy, once rehabilitation is complete, are comparable between open and arthroscopic approaches, assuming an appropriate patient selection and surgical technique.
Summary of Key Literature / Guidelines
The understanding and management of meniscal tears have evolved significantly, underpinned by robust clinical research and consensus guidelines.
-
Shift from Total to Partial Meniscectomy: The seminal work by Fairbank (1948) first described the degenerative changes observed post-total meniscectomy, initiating a long-term shift towards meniscal preservation. Subsequent studies, reinforced by biomechanical evidence, consistently demonstrated that total meniscectomy leads to increased tibiofemoral contact pressures and accelerated osteoarthritis, while partial meniscectomy, by preserving viable meniscal tissue, mitigates these long-term risks. Arthroscopic partial meniscectomy (APM) emerged as the preferred technique due to its minimally invasive nature, superior visualization, and faster recovery.
-
APM vs. Conservative Management for Degenerative Tears: Several high-quality randomized controlled trials (RCTs), including the landmark studies by Sihvonen et al. (NEJM 2013, 2016) and Katz et al. (NEJM 2013), have questioned the efficacy of APM for symptomatic degenerative meniscal tears in middle-aged and older patients without mechanical locking. These studies demonstrated no significant difference in functional outcomes between APM and sham surgery or physical therapy alone. This evidence has led to a more conservative approach for degenerative tears, emphasizing non-operative management (physical therapy, NSAIDs, injections) as the first-line treatment, reserving APM for those with clear mechanical symptoms (e.g., true locking, catching) unresponsive to adequate conservative therapy.
-
Indications for Meniscectomy: Current guidelines strongly advocate for meniscal repair over meniscectomy whenever anatomically feasible, particularly for peripheral tears in the vascularized red-red zone. When repair is not indicated or possible, meniscectomy should be as limited as possible, removing only the unstable, symptomatic portion of the meniscus. The goal is to create a stable, smooth meniscal rim, preserving the biomechanical integrity of the remaining structure. The seed content's mention of "partial meniscectomy" is consistent with this modern understanding, even within the context of an open approach.
-
Role of Open Meniscectomy: While arthroscopy is the standard, the open approach, as described in detail in the provided seed content, retains a recognized role in specific circumstances. These include situations where arthroscopy equipment is unavailable, in resource-limited settings, or for highly complex cases such as revision surgeries with severe arthrofibrosis, or the removal of very large loose bodies or foreign bodies that are difficult to manage arthroscopically. The principles of minimizing meniscal resection and protecting neurovascular structures remain paramount, irrespective of the surgical approach.
In conclusion, the contemporary approach to medial meniscectomy is defined by judicious patient selection, a strong emphasis on meniscal preservation (repair over resection), and a preference for minimally invasive arthroscopic techniques. However, a comprehensive understanding of the open approach, including its historical context and specific indications, remains an essential component of the orthopedic surgeon's armamentarium, particularly for those practicing in diverse healthcare environments.
Clinical & Radiographic Imaging

You Might Also Like


