Anterior Approach to Pubic Symphysis: Surgical Anatomy, Biomechanics & Fixation
Key Takeaway
The anterior approach to the pubic symphysis is a foundational orthopedic trauma technique. It's primarily used for direct visualization, reduction, and internal fixation of unstable symphyseal disruptions and displaced superior pubic ramus fractures. It also aids in biopsy/resection of neoplastic processes or debridement of infections, restoring pelvic stability and function.
Anterior Approach to the Pubic Symphysis: Your Surgical How-To Guide
Introduction & Epidemiology
The pubic symphysis, a non-synovial fibrocartilaginous joint, forms the anterior component of the pelvic ring. Its structural integrity is critical for pelvic stability, transmitting loads from the axial skeleton to the lower extremities, and resisting shear and rotational forces. While possessing limited intrinsic motion, its stability is paramount for normal ambulation and weight-bearing.
Injuries to the pubic symphysis typically result from high-energy trauma, often associated with other pelvic ring disruptions. Common mechanisms include anterior-posterior compression (APC) forces, lateral compression (LC), or vertical shear (VS) injuries, as categorized by the Young-Burgess classification. In APC-II and APC-III injuries, significant symphyseal diastasis occurs, often accompanied by disruption of the anterior sacroiliac ligaments and potentially the posterior sacroiliac complex. Vertical shear forces, often from falls or motor vehicle collisions, can result in complete disruption of the symphysis and unilateral or bilateral sacroiliac joint injuries. Less common etiologies include peripartum symphyseal diastasis (SPD), chronic osteomyelitis, stress fractures, and tumor involvement.
The anterior approach to the pubic symphysis is a foundational technique in orthopedic trauma surgery, primarily employed for direct visualization, reduction, and internal fixation of unstable symphyseal disruptions and displaced fractures of the superior pubic ramus. Its utility extends to the biopsy or resection of neoplastic processes and debridement of infectious foci affecting the pubic symphysis. Given the high-energy nature of these injuries, associated systemic morbidities and potential urogenital injuries necessitate thorough pre-operative assessment and multidisciplinary care.
Surgical Anatomy & Biomechanics
Surgical Anatomy
The pubic symphysis is formed by the articulation of the two pubic bones, united by a dense fibrocartilaginous disc and reinforced by robust ligaments.
- Pubic Symphysis Joint: A true fibrocartilaginous joint with a central cleft that can expand, particularly in females during childbirth. It is surrounded by strong ligamentous structures.
-
Ligamentous Structures:
- Superior Pubic Ligament: Connects the pubic crests superiorly, providing significant anti-shear stability.
- Inferior Pubic (Arcuate) Ligament: A thick, arch-shaped ligament bridging the inferior aspect of the symphysis, contributing to both stability and forming the superior boundary of the urogenital hiatus.
- Anterior and Posterior Pubic Ligaments: These are less distinct and blend with the periosteum, offering less intrinsic stability compared to the superior and inferior ligaments but reinforcing the joint capsule.
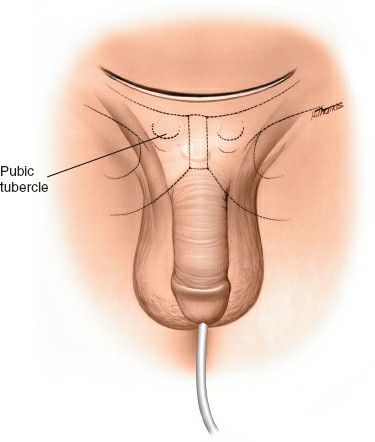
- Bony Landmarks: The pubic crests, pubic tubercles, and superior pubic rami are critical palpable and visual landmarks for surgical orientation.
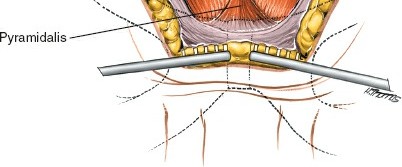
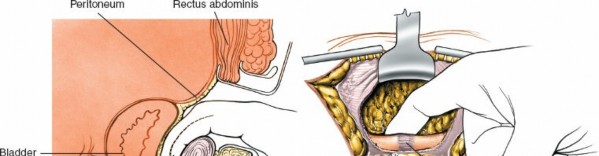
- Musculature: The rectus abdominis muscles originate from the pubic crests and symphysis. The pyramidalis muscle, when present, lies anterior to the rectus abdominis. These muscles must be reflected or split during the anterior approach.
-
Neurovascular Structures:
- Superficial Epigastric Vessels: Typically encountered in the subcutaneous layer, requiring ligation or cauterization.
- Inferior Epigastric Vessels: Located deep to the rectus abdominis, these vessels typically run lateral to the operative field but must be protected during lateral retraction.
- Corona Mortis (Aberrant Obturator Artery/Vein): An anatomical variant, where an aberrant obturator artery arises from the inferior epigastric artery or external iliac artery and crosses the superior pubic ramus near the symphysis to reach the obturator foramen. Venous variants are also common. Injury to these vessels can lead to severe hemorrhage and must be anticipated and carefully managed.
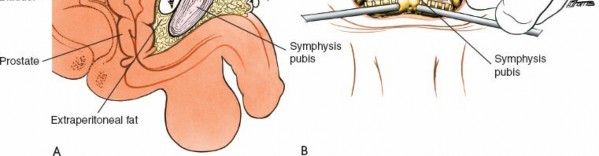
- Bladder and Urethra: These structures lie immediately posterior and inferior to the pubic symphysis, within the retropubic space (of Retzius). The bladder must be empty and protected throughout the dissection. A Foley catheter is essential.
- Spermatic Cord/Round Ligament: These structures exit the deep inguinal ring and traverse the inguinal canal, superior and lateral to the pubic symphysis. Care must be taken during lateral retraction to avoid injury.
- Ilioinguinal and Genitofemoral Nerves: These nerves are located more superior and lateral to the primary operative field but can be at risk with extensive lateral dissection or enthusiastic retraction.
Biomechanics
The pubic symphysis, along with the sacroiliac joints, forms a key ring structure critical for transferring loads between the axial and appendicular skeletons. Its integrity is fundamental to ambulation, weight-bearing, and maintaining pelvic dimensions.
- Load Transmission: Under normal physiological loading, the symphysis distributes forces, acting as a crucial anterior tension band for the pelvic ring.
- Stability Mechanisms: The strong superior and inferior ligaments resist vertical and rotational shear forces. The fibrocartilaginous disc absorbs compressive loads.
-
Failure Patterns:
- Anterior-Posterior Compression (APC): External rotation forces, often leading to symphyseal widening (diastasis) and disruption of anterior sacroiliac ligaments.
- Vertical Shear (VS): High-energy trauma causing complete disruption of the symphysis, sacrospinous and sacrotuberous ligaments, and posterior sacroiliac complex, leading to superior displacement of the hemipelvis. These injuries are inherently unstable and require robust fixation of both anterior and posterior pelvic rings.
- Restoration of anatomical alignment and rigid internal fixation of the pubic symphysis are vital for re-establishing the structural integrity of the pelvic ring, facilitating early mobilization, and minimizing long-term sequelae such as chronic pain, gait disturbance, and nonunion.
Indications & Contraindications
Indications for the Anterior Approach to the Pubic Symphysis
The anterior approach is primarily indicated for addressing pathology directly involving the pubic symphysis or adjacent structures amenable to anterior fixation.
-
Traumatic Disruptions:
- Symphyseal Diastasis: Typically, greater than 2.5 cm on AP pelvic radiographs, or greater than 1 cm with evidence of posterior instability (e.g., APC-II/III, VS injuries).
- Displaced Fractures of the Superior Pubic Ramus: When associated with symphyseal instability or requiring direct reduction and fixation through an anterior approach.
- Open Pelvic Fractures: Involving the symphysis, requiring debridement and stabilization.
- Chronic Instability/Malunion: Post-traumatic symphyseal dysfunction leading to chronic pain or gait abnormalities, refractory to conservative management.
-
Non-Traumatic Conditions:
- Chronic Osteomyelitis: For debridement, sequestrectomy, and saucerization of infected bone, and potentially culture-directed antibiotic bead placement.
- Tumors: For biopsy or en bloc resection of primary or metastatic tumors involving the pubic symphysis.
- Peripartum Symphyseal Diastasis (SPD): In severe cases (>4 cm or persistent pain/disability despite conservative measures) requiring surgical stabilization.
Contraindications
-
Absolute Contraindications:
- Active, Uncontrolled Local Infection: Deep infection precluding hardware implantation. In such cases, external fixation may be used as a temporizing measure following debridement.
- Medically Unstable Patient: If the patient cannot tolerate general anesthesia or significant blood loss.
-
Relative Contraindications:
- Severe Local Soft Tissue Compromise: Including burns, extensive degloving injuries, or necrosis that would jeopardize wound healing and increase infection risk.
- Previous Surgery with Scarring: May make dissection more challenging, but not prohibitive.
- Concomitant Critical Comorbidities: Requiring optimization before elective or semi-elective surgery.
Operative vs. Non-Operative Indications
| Indication Type | Operative Management | Non-Operative Management |
|---|---|---|
| Traumatic Pelvic | Symphyseal diastasis > 2.5 cm | Symphyseal diastasis < 2.5 cm (without evidence of posterior instability) |
| Injury | Symphyseal diastasis > 1 cm with signs of posterior pelvic ring instability (e.g., APC-II, APC-III, VS injuries) | Stable pubic ramus fractures without symphyseal involvement |
| Open pelvic fractures involving symphysis | Medically unfit patient where benefits of surgery do not outweigh risks | |
| Malunion/Nonunion with persistent pain or functional impairment | Peripartum symphyseal diastasis with mild symptoms or initial good response to conservative measures | |
| Infection | Chronic osteomyelitis of the pubic symphysis requiring debridement and potential hardware placement (after infection control) | Initial management of acute pubic symphysis infection (e.g., intravenous antibiotics) prior to surgical debridement, or minor localized infection without significant bone involvement. |
| Tumor | Biopsy or surgical resection of tumors involving the pubic symphysis, requiring reconstruction | Palliative care for metastatic disease not amenable to surgical resection, or cases where systemic therapy is the primary treatment. |
| Peripartum Diastasis | Severe, persistent SPD (>4 cm diastasis or debilitating pain/instability refractory to prolonged conservative management), particularly with objective instability. | Initial management for most cases of SPD: rest, pelvic binder, physical therapy, pain management, activity modification. |
Pre-Operative Planning & Patient Positioning
Comprehensive pre-operative planning is crucial for successful outcomes and mitigating complications, especially given the complex anatomy and potential for associated injuries.
Pre-Operative Planning
-
Imaging Review:
- Plain Radiographs: AP, inlet, and outlet views of the pelvis are standard to assess the degree of symphyseal diastasis, ramus fractures, and initial assessment of posterior pelvic ring integrity.
- Computed Tomography (CT) Scan: Essential for detailed assessment of all pelvic fractures, including comminution, displacement, and articular involvement. 3D reconstructions are invaluable for visualizing complex fracture patterns and planning implant trajectory.
- Magnetic Resonance Imaging (MRI): Indicated for suspected soft tissue injuries (e.g., sacroiliac ligament disruption not clearly seen on CT), avulsion injuries, osteomyelitis, or tumor workup.
-
Urologic Assessment:
Given the close proximity of the bladder and urethra, and the high incidence of urologic injury (up to 20% in severe pelvic ring disruptions), a urologic assessment is imperative.
- Retrograde Urethrogram: Should be performed in males with suspected urethral injury (e.g., blood at the meatus, high-riding prostate, scrotal/perineal hematoma).
- Cystogram: Recommended if bladder injury is suspected.
- Urethral Catheterization: A Foley catheter must be inserted prior to surgery to decompress the bladder and facilitate its protection during dissection. A full bladder will significantly impede surgical exposure and increase the risk of iatrogenic injury.
- Hemodynamic Status & Resuscitation: For trauma patients, ensure hemodynamic stability. Address any hypovolemia or coagulopathy. Cross-matched blood products should be readily available.
- Antibiotic Prophylaxis: Administer broad-spectrum intravenous antibiotics pre-incision, following hospital protocol for open fractures or major orthopedic surgery.
-
Equipment Preparation:
- Standard pelvic trauma set, including reduction clamps (e.g., Verbrugge, Farabeuf), large bone forceps, and possibly a pelvic C-clamp if needed for reduction.
- Appropriate plating system: 3.5 mm reconstruction plates, dedicated symphyseal plates (locking or non-locking), various screw lengths.
- Fluoroscopy (C-arm) with AP, inlet, and outlet views readily obtainable.
- Surgical drains for closure.
Patient Positioning
- Position: The patient is placed supine on the operating table.
- Table Considerations: A radiolucent table is preferred to allow unrestricted fluoroscopic imaging.
- Padding: Ensure adequate padding for all pressure points (heels, sacrum, elbows, head) to prevent pressure sores or nerve palsies.
- Imaging Access: Position the patient to allow clear AP, inlet, and outlet fluoroscopic views of the pelvis without repositioning. The C-arm should be draped and available.
- Draping: A wide surgical field is prepared and draped from the nipples to the mid-thigh, including both lower extremities, to allow for potential traction, manipulation, or extension of the approach if needed.
Detailed Surgical Approach / Technique
The anterior approach provides excellent direct visualization of the pubic symphysis, facilitating anatomical reduction and stable internal fixation.
Landmarks and Incision
Landmarks:
The superior pubic ramus, pubic tubercles, and pubic crests are typically palpable, even in many obese patients. In cases of symphyseal rupture, the diastasis may be palpable as a distinct gap. The midline is identified, extending caudally from the umbilicus.
Incision:
The preferred incision is a low transverse (Pfannenstiel) incision. This approach offers excellent cosmesis and allows for broad exposure of the rectus sheath.
* Make a curved incision, approximately 10-15 cm in length, centered about 1-2 cm superior to the palpable pubic symphysis (or gap). The lateral extent should allow for adequate retraction without excessive tension on the skin.
*
Superficial Dissection
- Skin and Subcutaneous Tissue: Incise the skin and subcutaneous fat.
- Superficial Vessels: Identify and carefully ligate or cauterize the superficial epigastric vessels encountered in the subcutaneous layer.
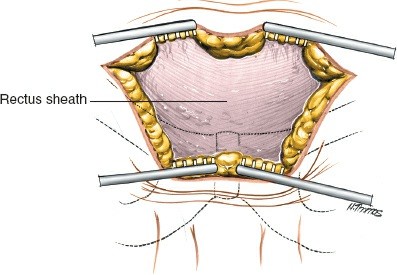
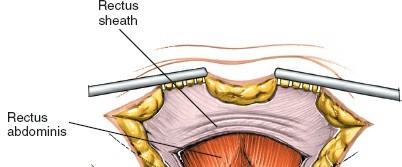
- Anterior Rectus Sheath: Dissect down to expose the anterior rectus sheath.
Internervous Plane
The seed content correctly states, "An internervous plane is not available for use in this approach." This is due to the direct nature of the approach through the midline muscular and fascial structures. Instead, this is an extraperitoneal, intermuscular/intramuscular approach. The rectus abdominis muscles are either split longitudinally or detached from the pubis and reflected.
Deep Dissection & Exposure
- Incise Anterior Rectus Sheath: Make a transverse incision through the anterior rectus sheath, approximately 1-2 cm proximal to its insertion on the pubic crests. This incision can be extended laterally as needed.
-
Rectus Abdominis Muscle:
- Option 1 (Midline Split): The rectus abdominis muscles can be bluntly or sharply separated in the midline. The pyramidalis muscle, if present, is either split or elevated. This is often preferred for direct midline access.
- Option 2 (Detachment): The rectus abdominis muscles can be subperiosteally elevated from their pubic attachments, allowing superior retraction. This provides wider access to the pubic rami laterally.
-
Retraction:
Retract the rectus abdominis muscles superiorly and laterally.
-
(Depicts muscle dissection and retraction)
-
- Posterior Rectus Sheath and Transversalis Fascia: Incise the posterior rectus sheath and transversalis fascia just superior to the symphysis. This exposes the preperitoneal space (Space of Retzius).
-
Enter Space of Retzius:
Carefully perform blunt dissection within the Space of Retzius. The primary goal is to sweep the peritoneum and bladder superiorly and posteriorly. This maneuver must be performed with extreme caution.
- Bladder Protection: The indwelling Foley catheter ensures the bladder is decompressed and small, reducing the risk of injury. Continually palpate the catheterized bladder during dissection to ensure it remains out of the field.
- Corona Mortis: Actively identify and protect the corona mortis (aberrant obturator artery/vein) if present, which may bridge the superior pubic ramus. Its injury can lead to significant hemorrhage. Ligation is an option if necessary, but careful dissection around it is preferred.
-
(Illustrates exposure of the symphysis, with careful attention to vital structures)
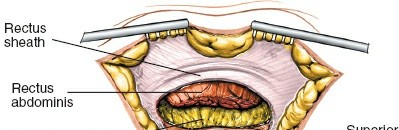
- Exposure of Symphysis and Rami: Continue dissection to adequately expose the anterior surface of the pubic symphysis and the medial portions of the superior pubic rami. Clear any hematoma or debris from the fracture site.
Fracture Reduction
- Debridement: Remove any interposed soft tissue (e.g., bladder, peritoneum, fibrous tissue) from the symphyseal gap.
-
Temporary Reduction:
- External Compression: For anterior-posterior compression injuries, direct manual compression or a pelvic C-clamp can be used to approximate the pubic rami.
- Pointed Reduction Clamps: Verbrugge or Farabeuf clamps applied directly to the pubic bodies provide excellent control for reduction.
- Leverage: Large bone hooks or Schanz pins temporarily inserted into the pubic bodies can provide leverage for reduction.
- Distraction/Translation: For vertical shear injuries, the hemipelvis may need to be distracted and translated inferiorly before compression. This can often be achieved with careful manipulation of the ipsilateral lower extremity by an assistant.
-
Confirm Reduction:
Assess reduction visually, by palpation (absence of symphyseal gap), and critically, with fluoroscopy. Obtain true AP, inlet, and outlet views. Anatomical reduction is the goal, aiming for diastasis < 1 cm, and minimal vertical translation.
-
(Demonstrates a reduction maneuver, potentially with clamps or instruments)
-
Internal Fixation
-
Plate Selection:
- Standard: A 3.5 mm reconstruction plate is commonly used. Contour the plate to the anterior surface of the pubic symphysis, typically with 2-3 holes on each side.
- Dedicated Symphyseal Plates: Modern low-profile, pre-contoured symphyseal plates are available, often with locking screw options, which can improve stability, especially in osteoporotic bone.
- Double Plating: For highly unstable injuries (e.g., vertical shear with significant posterior disruption), double plating (one plate anterior, one plate superior) may offer enhanced rotational and vertical stability, though it requires more extensive exposure and carries a higher risk of hardware prominence.
-
Plate Application:
- Position the contoured plate centrally over the symphysis.
- Secure the plate temporarily with K-wires or plate-holding forceps.
- Drill and insert bicortical screws. Ensure adequate screw length for bicortical purchase while avoiding intrapelvic penetration. Intraoperative fluoroscopy in both AP and inlet/outlet views is critical to confirm screw position and length, avoiding injury to the bladder or neurovascular structures.
-
(Shows application of a plate with screws) -
(Another view of plate fixation) -
(Could be a detail of screw placement or deep fixation)
- Addressing Ramus Fractures: If concomitant superior pubic ramus fractures are present, they can often be reduced and fixed with lag screws or small fragment plates through a slight extension of the same anterior approach.
Closure
- Irrigation and Hemostasis: Copiously irrigate the wound and achieve meticulous hemostasis, paying particular attention to the retropubic space.
- Drain Placement: A suction drain (e.g., Jackson-Pratt) is often placed in the retropubic space to evacuate hematoma and seroma, reducing the risk of infection.
- Rectus Abdominis Reapproximation: If the rectus muscles were separated in the midline, reapproximate them with absorbable sutures. If they were detached from the pubic crests, they can be reattached or allowed to scar down.
- Anterior Rectus Sheath Closure: Close the anterior rectus sheath meticulously with strong, absorbable or non-absorbable sutures. This is a critical layer for preventing hernia and providing abdominal wall integrity.
-
Subcutaneous and Skin Closure:
Close the subcutaneous layers and skin in a standard fashion.
-
(Likely showing the final wound closure or a critical step in deep closure)
-
Complications & Management
Despite meticulous surgical technique, complications can arise, ranging from minor issues to life-threatening events. Prompt recognition and appropriate management are crucial.
Intraoperative Complications
-
Hemorrhage:
- Cause: Injury to the extensive venous plexus in the Space of Retzius, superior/inferior epigastric vessels, or the corona mortis (aberrant obturator artery/vein).
- Management: Direct pressure, bipolar cautery, meticulous ligation, topical hemostatic agents. In severe cases, consider embolization by interventional radiology.
-
Urologic Injury:
- Cause: Direct trauma to the bladder or urethra during dissection, especially if the bladder is full or unprotected, or from misplaced screws.
- Management: Immediate consultation with urology. Intraoperative repair, often requiring prolonged urethral catheterization or suprapubic cystostomy.
-
Peritoneal Violation:
- Cause: Overly aggressive superior/posterior dissection into the peritoneal cavity.
- Management: Meticulous repair of the peritoneal tear. Document carefully. Usually does not require further intervention unless bowel injury is suspected.
-
Neurovascular Injury:
- Cause: Rare, but can involve obturator nerve/vessels (with extensive lateral screw placement or dissection), or ilioinguinal/genitofemoral nerves (with excessive lateral dissection/retraction).
- Management: Prevention through careful dissection and imaging. If identified, primary repair (for vessels) or careful neurolysis (for nerves).
-
Malreduction:
- Cause: Inadequate visualization, failure to clear interposed soft tissue, insufficient reduction maneuvers, or misinterpretation of fluoroscopic images.
- Management: Re-attempt reduction with different clamps or maneuvers. Ensure all views (AP, inlet, outlet) confirm anatomical alignment before definitive fixation.
Postoperative Complications
-
Infection:
- Incidence: Varies, but can be significant in open fractures or prolonged procedures.
- Management: Superficial infections may respond to wound care and antibiotics. Deep infections often require surgical debridement, intravenous antibiotics, and potentially hardware removal (usually after fracture union).
-
Hematoma/Seroma:
- Cause: Inadequate hemostasis, extensive dead space.
- Management: Small ones may resolve spontaneously. Large or symptomatic collections may require aspiration or surgical evacuation. Prophylactic drains can reduce incidence.
-
Thromboembolic Events (DVT/PE):
- Incidence: High in pelvic trauma.
- Management: Prophylactic anticoagulation per institutional guidelines. Early mobilization.
-
Urinary Retention/Dysfunction:
- Cause: Postoperative pain, nerve irritation, or temporary bladder dysfunction.
- Management: Temporary catheterization. Urologic consultation if prolonged.
-
Nonunion/Malunion:
- Incidence: Higher with inadequate reduction or unstable fixation.
- Management: Conservative management for asymptomatic cases. Symptomatic nonunion may require revision surgery, bone grafting, and potentially additional posterior fixation.
-
Hardware Failure:
- Cause: Excessive load on the implant due to inadequate reduction, nonunion, or patient non-compliance with weight-bearing restrictions.
- Management: Revision surgery with stronger fixation, addressing any underlying nonunion.
-
Chronic Pain:
- Cause: Persistent instability, hardware prominence, symphysitis, nerve irritation, or post-traumatic arthritis.
- Management: Conservative measures (analgesia, physical therapy). Hardware removal (if prominent). Fusion of the symphysis for intractable pain due to nonunion or arthritis.
-
Heterotopic Ossification (HO):
- Cause: Inflammation and soft tissue trauma.
- Management: Prophylaxis with NSAIDs or radiation post-operatively in high-risk patients. Symptomatic HO may require surgical excision after maturation.
Table of Common Complications and Management Strategies
| Complication | Incidence (Approx.) | Salvage/Management Strategies |
|---|---|---|
| Intraoperative Hemorrhage | 5-15% (severe) | Direct pressure, bipolar cautery, ligatures; topical hemostatics (e.g., Surgicel, Gelfoam); assess for corona mortis injury; interventional radiology embolization for persistent bleeding. |
| Urologic Injury | 2-20% (pelvic trauma) | Intraoperative urology consultation; primary repair of bladder/urethra injury; prolonged Foley catheterization or suprapubic cystostomy. |
| Malreduction | Varies | Re-attempt reduction with different instruments (e.g., Verbrugge clamps, pelvic C-clamp); meticulous debridement of interposed tissue; intraoperative fluoroscopy in multiple planes (AP, inlet, outlet) for confirmation. |
| Surgical Site Infection | 1-5% (deep) | Superficial: wound care, oral antibiotics. Deep: surgical debridement, irrigation, IV antibiotics, cultures; consider hardware retention if union achieved, or removal if nonunion/persistent infection. |
| Hematoma/Seroma | 5-10% | Observation for small collections; aspiration for symptomatic/large collections; surgical evacuation if tense, expanding, or infected. Prophylactic drain placement can reduce incidence. |
| DVT/PE | 10-30% (clinical DVT) | Pharmacologic prophylaxis (LMWH, fondaparinux) per institutional protocol; mechanical prophylaxis (sequential compression devices); early mobilization; screening duplex ultrasound if symptoms arise; therapeutic anticoagulation for confirmed DVT/PE. |
| Nonunion/Malunion | 5-10% | Asymptomatic: observation. Symptomatic: revise fixation, autologous bone grafting (e.g., iliac crest), potential posterior fixation if instability persists, or symphysis fusion for chronic pain. |
| Hardware Failure | 5-15% | Remove failed hardware; revise fixation with stronger construct (e.g., double plating, locking plate); address underlying nonunion or instability; consider posterior fixation. |
| Chronic Pain (Hardware Prominence) | 10-20% | Initial conservative management (NSAIDs, physical therapy); elective hardware removal typically 12-18 months post-op, after radiological union is confirmed. |
| Heterotopic Ossification | 10-20% (radiographic) | Prophylaxis with NSAIDs (e.g., indomethacin) or single-dose radiation in high-risk patients. Symptomatic HO: surgical excision after maturation (usually >6-12 months post-onset) if impacting function. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is integral to achieving optimal functional outcomes following anterior symphyseal fixation. The protocols are guided by the stability of fixation and the presence of any concomitant posterior pelvic ring injuries.
Early Post-Operative Phase (Days 0-2 weeks)
- Pain Management: Multimodal analgesia (opioids, NSAIDs, acetaminophen, nerve blocks) to facilitate early mobilization.
-
Weight-Bearing:
- Stable Fixation (Isolated Symphysis or well-reduced APC-II/III with adequate posterior fixation): Touch-down weight-bearing (TDWB) or protected weight-bearing (PWB) with crutches or a walker. Progressive weight-bearing may be initiated as comfort allows and based on surgeon preference.
- Less Stable Fixation (e.g., VS injuries, incomplete posterior fixation): Strict non-weight-bearing (NWB) on the affected side, or bilateral NWB if needed, for 6-8 weeks.
-
Mobilization:
- Out of Bed: Encourage sitting and standing activities as tolerated, usually within 24-48 hours post-surgery.
- Transfers: Assist with bed mobility and transfers.
- Activities of Daily Living (ADLs): Initiate supervised ADL training.
-
Physical Therapy:
- Gentle Range of Motion (ROM): Initiate gentle hip and knee ROM exercises (flexion, extension, abduction, adduction within pain limits).
- Breathing Exercises: Deep breathing and incentive spirometry to prevent pulmonary complications.
- Pelvic Floor Exercises: Gentle activation of pelvic floor muscles may begin if pain permits.
Intermediate Phase (2-8 weeks)
-
Weight-Bearing Progression:
- Gradual progression from TDWB/PWB to partial weight-bearing (PWB) and then full weight-bearing (FWB) over several weeks, guided by clinical pain, radiographic signs of healing, and the stability of the overall pelvic ring fixation.
-
Physical Therapy:
- Strengthening: Initiate isometric strengthening of hip abductors, adductors, and core musculature. Avoid excessive shear forces across the pelvis.
- Flexibility: Continue with gentle stretching to maintain hip and knee flexibility.
- Gait Training: Progress from assistive devices to independent ambulation as strength and confidence improve.
- Pelvic Stability: Specific exercises to improve lumbopelvic stability.
- Activity Modification: Avoid activities that place high stress on the pelvic ring (e.g., running, jumping, heavy lifting, twisting).
Advanced Phase (8 weeks – 6 months)
- Weight-Bearing: Full weight-bearing should be achieved by this stage, assuming radiographic evidence of healing.
-
Physical Therapy:
- Progressive Strengthening: Advance to dynamic strengthening exercises for core, hip, and lower extremity muscles.
- Proprioception and Balance: Incorporate exercises to improve balance and coordination.
- Functional Training: Tailored exercises to meet specific occupational or recreational demands.
-
Return to Activity:
- Low-Impact Activities: Gradually introduce low-impact activities like cycling or swimming.
- Return to Work: Depending on job demands, a staged return to work may be possible.
- High-Impact Sports: Return to high-impact or contact sports is generally deferred until 6 months or longer, and only after complete radiographic union and full strength/proprioception have been achieved.
Long-Term Follow-up (6 months+)
- Radiographic Assessment: Monitor for signs of hardware failure, nonunion, or post-traumatic changes.
-
Hardware Removal:
- Considered typically 12-18 months post-op if the patient is symptomatic (e.g., hardware prominence, chronic pain) or if the hardware is in an area of potential irritation. Not routinely removed if asymptomatic.
- Prior to removal, confirm radiographic union of the symphysis.
- Continued Activity: Encourage maintenance of an active lifestyle. Address any residual pain or functional limitations.
Summary of Key Literature / Guidelines
The management of pubic symphysis injuries has evolved significantly, guided by a robust body of literature and classification systems.
Classification Systems
- Tile Classification: Categorizes pelvic ring injuries based on mechanical stability. Symphyseal disruptions often fall under partially stable (B-type, rotational instability) or unstable (C-type, combined rotational and vertical instability) injuries.
- Young-Burgess Classification: Based on injury mechanism and vector. Symphyseal diastasis is characteristic of Anterior-Posterior Compression (APC-II and APC-III) injuries. Vertical Shear (VS) injuries also involve symphyseal disruption alongside complete posterior pelvic ring failure. These classifications dictate the need for anterior and often concomitant posterior fixation.
Optimal Fixation Strategies
- Single vs. Double Plating: While single anterior plating with a 3.5 mm reconstruction plate has historically been standard for symphyseal diastasis, several studies, particularly in biomechanical analyses and for vertical shear injuries, suggest that double plating (anterior and superior) may provide superior rotational and vertical stability. However, double plating carries a higher risk of hardware prominence and surgical morbidity. The decision depends on the injury pattern, bone quality, and surgeon preference.
- Locking vs. Non-Locking Plates: Locking plates offer fixed-angle constructs, which can be advantageous in osteoporotic bone or complex comminuted fractures by providing angular stability and potentially reducing pull-out strength issues. However, standard non-locking reconstruction plates remain highly effective in good bone quality with proper contouring and bicortical screw purchase.
- Concomitant Posterior Fixation: It is a well-established principle that for unstable pelvic ring injuries (Tile C, Young-Burgess APC-III, VS), isolated anterior fixation is insufficient. Stable posterior pelvic ring fixation (e.g., sacroiliac screw fixation, iliosacral plating, sacral bar, or transiliac plating) is paramount to re-establish overall pelvic stability and prevent hardware failure and nonunion of the symphysis.
Role of External Fixation
External fixation can serve as a valuable temporary measure for rapid stabilization of hemodynamically unstable pelvic trauma patients or for definitive management in cases of gross contamination or extensive soft tissue injury where internal fixation is contraindicated. It can also be used as an adjunct to internal fixation.
Outcomes
High rates of union and good functional outcomes are generally achieved with anatomical reduction and stable internal fixation of the pubic symphysis, especially when combined with appropriate posterior fixation for unstable injuries. Persistent pain, gait disturbances, and sexual dysfunction are potential long-term complications, highlighting the importance of meticulous surgical technique and comprehensive rehabilitation.
Evolving Concepts
Minimally invasive approaches to symphyseal fixation are being explored, though the direct open anterior approach remains the gold standard for most complex traumatic disruptions due to superior visualization and reduction capabilities. Advances in implant design and personalized surgical planning through 3D printing and intraoperative navigation continue to refine techniques and improve precision.
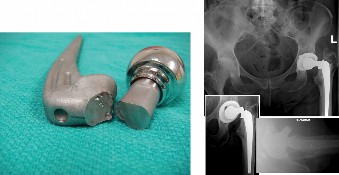
Clinical & Radiographic Imaging
You Might Also Like