Innovative Auxiliary Screw Technique: Preventing IMN Failure in Intertrochanteric Fractures
Key Takeaway
The innovative auxiliary screw technique prevents IMN failure in intertrochanteric fractures by precisely eliminating the anterior cortical gap. This ensures robust bone-to-bone contact, reducing lag screw shear stress. It prevents cutout and excessive sliding, significantly enhancing fixation stability, improving surgical success and patient outcomes.
Introduction & Epidemiology
股骨转子间骨折(Intertrochanteric Fractures, ITFs)是老年人群常见的髋部骨折类型,通常由低能量跌倒引起,但也可见于年轻患者的高能量损伤。随着全球人口老龄化,ITFs 的发病率持续上升,已成为一个重大的公共卫生问题,给患者、家庭和社会带来了沉重的负担。流行病学数据显示,ITFs 的一年期死亡率高达15-30%,显著高于同年龄段无骨折人群,且术后常伴随功能受限、生活质量下降等问题。这种高发病率和高致死率不仅对个体健康构成威胁,也给医疗系统带来了巨大的经济和社会压力。根据AO/OTA分类,ITFs主要分为31-A1(稳定型)、31-A2(不稳定型)和31-A3(极不稳定型)三类,其中不稳定型和极不稳定型骨折占比较高,且预后相对较差。AO/OTA 31-A1 fractures are typically stable with an intact posteromedial cortex, while 31-A2 fractures are inherently unstable due to posteromedial comminution, and 31-A3 fractures, characterized by reverse obliquity or compromise of the lateral femoral wall, represent the most unstable patterns, often associated with higher failure rates.
手术治疗是移位性转子间骨折的标准治疗方法,旨在实现早期活动、减少卧床相关并发症并最大限度地恢复功能。历史上,治疗方法从早期的牵引、外固定架到动力髋螺钉(Dynamic Hip Screw, DHS)逐渐演变。DHS在稳定型骨折中取得了良好的效果,但其在不稳定型骨折中生物力学不足,易导致内翻塌陷和螺旋滑动。目前,髓内钉(Intramedullary Nail, IMN)系统因其生物力学优势、微创特性以及在不稳定骨折中提供更优稳定性,已成为治疗 ITFs 的主要内固定方式。髓内钉系统通过将载荷更靠近股骨的机械轴心,减少了力臂,从而降低了内固定失效的风险,特别适用于不稳定型转子间骨折(如AO/OTA 31-A2和31-A3型)。
尽管髓内钉的应用日益普及,但其术后并发症,如螺钉切出(cutout)、螺钉过度滑动(excessive sliding)、Z效应/反Z效应以及内固定失效,仍是临床面临的挑战。不稳定型转子间骨折内固定手术的总体失败率在3%至12%之间,严重影响患者预后并导致二次手术。大量研究指出, 复位质量不良是导致内固定失效的独立危险因素 。具体而言,闭合复位过程中,尽管在AP位透视下可能显示复位满意,但侧位透视时常发现骨折端仍存在前侧骨皮质断裂或分离,即 “前侧骨皮质间隙”或“前内侧皮质缺损” 。这种残余的移位极易导致术后内固定承受异常应力而失效,表现为螺钉在松质骨中滑动或切割股骨头。这种前皮质间隙 allows for anterior toggling and micromotion of the proximal fragment, particularly during weight-bearing and hip flexion, placing undue shear stress on the lag screw and increasing the risk of cutout. For elderly patients with osteoporotic bone, the integrity of the cortical shell is paramount for stable fixation. To overcome this critical limitation, we propose an innovative auxiliary screw technique, designed to provide additional stability and precise reduction control by directly addressing and eliminating the residual anterior cortical gap during closed reduction, thereby significantly enhancing surgical success rates, mitigating complications, and precluding the inherent risks of lag screw sliding and fixation failure.
Surgical Anatomy & Biomechanics
股骨近端解剖
股骨近端是转子间骨折发生的部位,其复杂的解剖结构与生物力学特性对手术策略及预后具有决定性影响。
*
骨性结构:
股骨近端包括股骨头、股骨颈、大转子和小转子。转子间线(anterior intertrochanteric line)连接大转子与小转子,而转子间嵴(posterior intertrochanteric crest)则位于后方。转子间骨折通常发生在这两条线之间。股骨颈由骨密质包绕松质骨,股骨头完全由松质骨构成。股骨近端骨质疏松时,骨小梁的吸收导致骨强度显著下降,特别是位于股骨颈的Ward's三角区,其骨密度最低。This region, located in the superolateral aspect of the femoral neck, is characterized by sparse trabeculae and is highly susceptible to collapse in osteoporotic bone, particularly under shear forces. The medial calcar region, conversely, is a dense load-bearing structure providing crucial support for the femoral head and neck, and its integrity is vital for stable fixation.

-
肌肉附着与致畸力: 大转子上附着臀中肌和臀小肌,小转子上附着髂腰肌。这些肌肉的牵拉在骨折发生后导致特有的移位模式:近端骨折块(股骨头-颈-大转子复合体)通常处于 外旋和屈曲位 (由髂腰肌牵拉小转子),而远端骨折块则表现为内收和短缩。具体而言,髂腰肌的强大牵拉导致小转子连同股骨头-颈复合体发生屈曲和外旋,而臀肌的牵拉则可能导致大转子部位的移位。股骨干在重力作用下常表现为内收和向近端移位,导致肢体短缩。这种典型的移位模式是闭合复位时需要克服的主要障碍。

-
股骨头血供: 股骨头的主要血供来源于旋股内侧动脉(medial circumflex femoral artery, MCFA)的终末支,通过股骨颈后上和后下方的囊外动脉环以及随圆韧带走行供应的血管进入股骨头。虽然转子间骨折通常不直接损伤股骨头血供,但严重的移位和髓内钉置入过程中对股骨颈内侧皮质的过度牵拉或血管损伤,理论上仍可能影响血供,尽管股骨头坏死在ITFs中远不如股骨颈骨折常见。
生物力学特性
髓内钉(IMN)系统在不稳定型转子间骨折中的生物力学优势主要体现在其将载荷传递至股骨的机械轴线附近,从而减少了力臂,降低了内固定失效的风险。与DHS等髓外固定系统相比,IMN的力臂更短,弯曲应力更小,尤其在承受垂直载荷时表现出更优的抗内翻塌陷能力。
然而,髓内钉固定仍然面临挑战,特别是当复位质量不佳时。
“前侧骨皮质间隙”或“前内侧皮质缺损”
是导致内固定失效的关键生物力学因素。即使在AP位透视下骨折复位看似理想,侧位透视下若存在前皮质间隙,则意味着股骨头-颈的近端骨块与股骨干的远端骨块在前侧皮质上未能实现骨-骨接触。这种间隙的存在使得髓内钉的拉力螺钉(cephalomedullary lag screw)在股骨头内的松质骨中承受额外的剪切力。在患者早期负重和活动过程中,近端骨块会在前皮质间隙处发生“打折”或“轴向旋转”样运动,导致拉力螺钉反复切割股骨头松质骨,最终导致螺钉切出(cutout)。这种不稳定的状态也增加了螺钉过度滑动、Z效应/反Z效应及整体内固定失效的风险。


理想的复位应实现骨折端的解剖或近解剖复位,特别是内外侧及前后侧皮质的良好对合,以实现负重区的骨-骨接触,将应力从内固定器械传导至骨骼本身,从而最大程度地利用骨折块自身的支撑能力。前皮质间隙的存在破坏了这种重要的骨-骨接触,使得内固定器械承受所有载荷,特别是在骨质疏松的患者中,极易导致医源性松质骨骨折或螺钉移位。拉力螺钉的尖-顶距(Tip-Apex Distance, TAD)也是评估生物力学稳定性的关键指标。TAD值过大(通常>25mm)意味着螺钉在股骨头内固定不牢,增加了切出风险。然而,即使TAD值理想,若存在前皮质间隙,内固定的整体稳定性仍会显著受损。
Indications & Contraindications
Indications
Surgical management is generally indicated for most displaced intertrochanteric fractures to facilitate early mobilization, reduce complications associated with prolonged bed rest, and restore functional independence.
-
Displaced Intertrochanteric Fractures (AO/OTA 31-A1, A2, A3):
The primary indication for surgical fixation.
- Stable fractures (31-A1): While DHS may be considered, IMN offers superior biomechanics and increasingly preferred, especially in osteoporotic bone.
- Unstable fractures (31-A2, A3): IMN is the implant of choice due to its load-sharing characteristics closer to the mechanical axis, providing better stability against varus collapse and rotation. This includes fractures with significant posteromedial comminution, reverse obliquity, or lateral wall compromise.
- Pathological Fractures: Due to metastatic disease or primary bone tumors involving the intertrochanteric region.
- Impending Pathological Fractures: Prophylactic nailing to prevent fracture in cases of extensive lytic lesions.
- Failed Non-Operative Management: Rarely, for non-displaced fractures that subsequently displace.
- Polytrauma Patients: IMN allows for early stabilization, facilitating overall patient management.
- Patients requiring early mobilization: To prevent complications such as DVT, pneumonia, and pressure ulcers, particularly in the elderly.
Contraindications
While surgical fixation is broadly indicated, certain patient- and fracture-specific factors may contraindicate or necessitate a cautious approach.
-
Absolute Contraindications:
- Active Local or Systemic Infection: Increases the risk of deep surgical site infection and osteomyelitis.
- Severe Open Fractures (Gustilo Type III B/C): Requires extensive debridement and management of soft tissue defects before definitive fixation.
- Irreparable Vascular Injury: Uncontrolled vascular damage necessitating limb salvage.
- Prohibitive Medical Comorbidities: Patients with severe, uncontrolled medical conditions (e.g., acute myocardial infarction, uncontrolled sepsis) for whom the risks of general anesthesia and surgery outweigh the benefits.
- Non-Ambulatory Status Prior to Fracture: For patients with no realistic potential for ambulation, non-operative management may be considered if pain can be controlled.
-
Relative Contraindications:
- Extremely Severe Comminution: Where no adequate purchase for fixation can be achieved (very rare with modern IMN systems).
- Severe Osteopenia/Osteoporosis: While often an indication for IMN due to its stability, extreme bone fragility can challenge screw purchase, necessitating adjunctive techniques or cement augmentation.
- Patients with limited life expectancy and minimal pain: Non-operative care may be chosen after shared decision-making.
Operative vs. Non-Operative Indications
| Indication Type | Operative Management (IMN) | Non-Operative Management |
|---|---|---|
| Fracture Pattern | Almost all displaced ITFs (AO/OTA 31-A1, A2, A3) | Undisplaced, stable ITFs (rare) |
| Unstable ITFs (31-A2, 31-A3) | ||
| Reverse obliquity fractures | ||
| Subtrochanteric extension | ||
| Pathological fractures | ||
| Patient Factors | Medically fit for surgery | Medically unstable (absolute contraindication to surgery) |
| Desired early mobilization and functional recovery | Non-ambulatory prior to fracture, low functional demand | |
| Patients with extremely limited life expectancy where palliation is primary goal |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is crucial for optimizing surgical outcomes and minimizing complications in intertrochanteric fracture fixation with an intramedullary nail.
Pre-Operative Planning
-
Patient Assessment:
- Medical Comorbidities: Comprehensive review of systemic health, including cardiovascular, pulmonary, renal, and endocrine status. Optimize pre-existing conditions.
- Medication Review: Identify antiplatelet agents, anticoagulants, or other medications that may require temporary cessation or adjustment.
- Nutritional Status: Assess for malnutrition, common in elderly patients, which can impair wound healing and increase infection risk.
- Functional Status: Document pre-injury ambulatory status, use of assistive devices, and cognitive function to establish realistic post-operative goals.
- Anesthesia Consultation: Evaluate patient for suitability for regional (spinal/epidural) or general anesthesia.
-
Imaging Analysis:
- Radiographs: Obtain AP and lateral views of the affected hip and femur. A full-length femur AP view is often beneficial to assess the entire femoral shaft and canal anatomy for nail length and diameter selection. Consider contralateral hip radiographs for templating in cases of significant deformity or hardware if IMN placement is anticipated.
- CT Scan: Reserved for highly complex fracture patterns, significant comminution, or for identifying subtle articular involvement, although typically not required for standard ITFs.
- Evaluation of Fracture Characteristics: Identify fracture type (AO/OTA), degree of comminution (especially posteromedial and lateral wall integrity), and magnitude of displacement (shortening, varus, rotation).
-
Implant Selection & Templating:
- Nail Length and Diameter: Based on patient height, femoral canal dimensions (assessed from radiographs), and fracture pattern. Long nails are preferred for unstable fractures, subtrochanteric extension, or concerns for distal fracture propagation. Short nails are generally sufficient for stable fractures confined to the trochanteric region.
- Cephalomedullary Screw Type: Static vs. dynamic locking, single vs. dual screws. The choice depends on surgeon preference and implant system, with single lag screw systems being most common.
- Tip-Apex Distance (TAD): The ideal position of the lag screw in the femoral head should be templated. The TAD, measured on both AP and lateral radiographs, should ideally be <25mm to minimize cutout risk. The lag screw should be centered or slightly inferior-central on the AP view and central on the lateral view.
- Auxiliary Screw Planning: If the innovative auxiliary screw technique is planned, consider its trajectory. It will typically be placed inferior and anterior to the main lag screw, bridging the anterior cortical gap. Its entry point and length should be estimated to achieve firm purchase in both proximal and distal fragments without impinging on the main lag screw or violating articular cartilage.
-
Prophylaxis:
- Antibiotics: Administer intravenous broad-spectrum antibiotics within 60 minutes prior to incision.
- Thromboembolism Prophylaxis: Initiate DVT prophylaxis (pharmacological and/or mechanical) pre-operatively and continue post-operatively.
Patient Positioning
The standard position for IMN fixation of ITFs is supine on a fracture table. This positioning facilitates closed reduction and allows for adequate fluoroscopic imaging in both AP and lateral planes.

-
Fracture Table Setup:
- The patient is transferred to the fracture table. The affected leg is placed in the traction boot with appropriate padding.
- The contralateral leg is placed in a well-padded boot or on a leg holder, abducted and flexed to allow unrestricted C-arm access.
- The perineal post should be well-padded and positioned to provide counter-traction against the uninjured side.
- Ensure the patient's torso is centered on the table and secured with chest and pelvic straps.
-
Fluoroscopic Access:
- Verify C-arm mobility to obtain true AP and lateral views of the hip and entire femur.
- The C-arm should be positioned parallel to the fracture table for AP views and perpendicular for lateral views. The image intensifier should be draped sterilely.
-
Reduction Preparation:
- Apply gentle longitudinal traction to achieve length restoration and disimpact the fracture fragments.
- Adjust rotation (typically internal rotation) and abduction/adduction to align the femoral neck axis with the shaft.
- The goal is to achieve the best possible closed reduction on fluoroscopy, both AP and lateral. Special attention should be paid to the anterior cortical profile on the lateral view.
-
Sterile Preparation:
- Prepare and drape the surgical field from the mid-abdomen to the mid-calf on the affected side, ensuring wide exposure around the greater trochanter and distal femur.
Detailed Surgical Approach / Technique
The goal of surgical management for intertrochanteric fractures with an intramedullary nail is to achieve stable fixation, facilitating early weight-bearing and functional recovery. The innovation of the auxiliary screw technique specifically addresses the challenge of inadequate anterior cortical reduction, a critical determinant of fixation stability.
1. Reduction Techniques
Optimal reduction is paramount. The typical displacement of the proximal fragment involves flexion, external rotation, and varus, while the distal fragment is often adducted and shortened.
*
Closed Reduction Maneuvers:
*
Traction:
Longitudinal traction is applied via the fracture table to restore leg length and disimpact the fracture.
*
Internal Rotation:
Counteracts the external rotation of the proximal fragment. This often requires significant force.
*
Abduction:
Corrects any varus deformity and aligns the femoral neck axis with the shaft.
*
Flexion/Extension:
Adjusting hip flexion can help align the fragments, especially in comminuted patterns.
* Fluoroscopic guidance (AP and lateral views) is essential to confirm reduction. The AP view assesses length and varus/valgus alignment, while the lateral view is crucial for rotational alignment and detecting the
anterior cortical gap
.

-
Addressing the Anterior Cortical Gap: Despite satisfactory AP reduction, the lateral view often reveals a persistent anterior cortical gap or step-off. This signifies inadequate reduction of the anterior femoral neck/head to the anterior shaft cortex. This gap represents a biomechanical instability, allowing for toggling of the proximal fragment and excessive shear forces on the lag screw.

-
Limited Open Reduction: If closed reduction fails to adequately address the anterior cortical gap or other significant displacement, limited open reduction may be necessary. This can involve using bone hooks, reduction clamps, or a pointed reduction clamp percutaneously through a small incision to manipulate fragments and achieve better apposition.
2. Standard Intramedullary Nail Insertion
Once the best possible reduction is achieved, the standard IMN procedure is initiated.
*
Incision and Entry Point:
A longitudinal skin incision (typically 3-5 cm) is made proximally from the tip of the greater trochanter. The gluteus medius is split longitudinally, and a starting awl or drill creates an entry point at the tip or slightly medial to the tip of the greater trochanter, in line with the femoral canal.
*
Guidewire Insertion:
A guidewire is advanced down the femoral canal under fluoroscopic guidance, ensuring it is centered in both AP and lateral views.
*
Reaming (if necessary):
The proximal femur is reamed over the guidewire to the appropriate diameter for the chosen nail.
*
Nail Insertion:
The intramedullary nail is gently inserted over the guidewire. Confirm proper seating of the nail and absence of fracture distraction or loss of reduction.
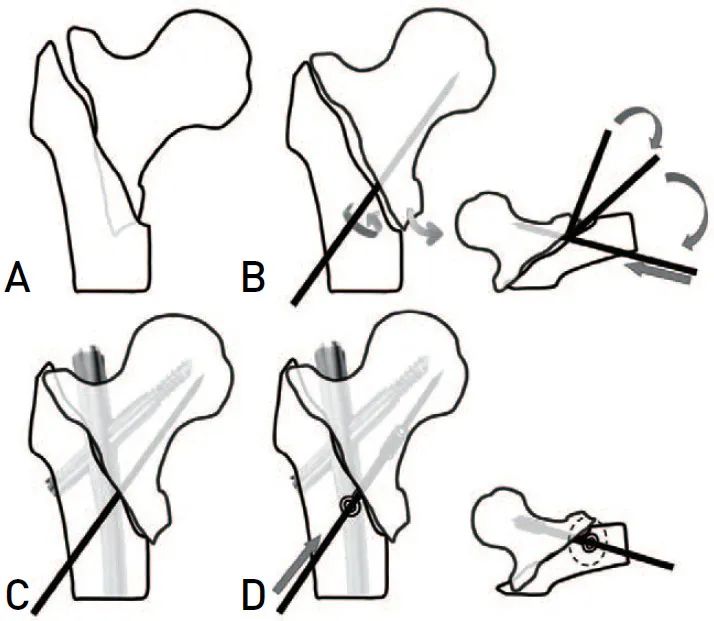
3. The Innovative Auxiliary Screw Technique to Address the Anterior Cortical Gap
This is the critical step to prevent fixation failure due to residual anterior cortical instability.
*
Identification of the Residual Gap:
After initial nail insertion and with the best possible reduction achieved by traditional maneuvers, carefully review the lateral fluoroscopic view. A persistent anterior cortical step-off or gap is the target for this technique. The main cephalomedullary lag screw guidewire can be inserted at this stage, but the screw itself is usually inserted after the auxiliary screw.
-
Auxiliary Screw Placement Strategy:
- Entry Point Determination: Under fluoroscopic guidance (both AP and lateral), identify a percutaneous entry point for the auxiliary screw. This point is typically inferior and anterior to the planned trajectory of the main cephalomedullary lag screw (which is inserted through the nail). The entry point should allow for a trajectory that crosses the anterior cortical gap from the distal fragment into the proximal fragment's anterior cortex. Care must be taken to avoid the main lag screw path and the articular surface.
- Mini-Incision and Drill Hole: A small (e.g., 1-2 cm) incision is made at the identified entry point. A drill bit (e.g., 2.5mm or 3.2mm) is used to create a pilot hole, ensuring it crosses the anterior cortical gap. The drill should engage both the distal fragment's anterior cortex and the proximal fragment's anterior cortex. This is done under meticulous fluoroscopic control to ensure correct trajectory and depth.
-
Screw Insertion:
A fully threaded cortical screw (e.g., 3.5mm or 4.0mm) is then inserted through the pilot hole. The screw should be long enough to achieve bicortical purchase or robust cancellous purchase in the femoral head/neck and unicortical purchase in the anterior cortex of the distal fragment, effectively
compressing
the anterior cortical defect. As the screw is tightened, its primary function is to draw the anterior cortices of the proximal and distal fragments into firm apposition, thereby closing the gap and enhancing rotational and axial stability.

- Mechanism of Action: This auxiliary screw acts as a direct reduction aid and a buttress. It prevents anterior toggling of the proximal fragment, provides crucial interfragmentary compression across the anterior cortical defect, and significantly reduces the shear forces on the main cephalomedullary lag screw. This creates a more stable construct that can better withstand early weight-bearing and functional stresses, particularly in osteoporotic bone.
-
Verification of Gap Closure: After the auxiliary screw is inserted and tightened, re-evaluate reduction on both AP and lateral fluoroscopic views. The anterior cortical gap should now be eliminated or markedly reduced. This is a critical success criterion for the auxiliary screw technique.

-
AP view showing auxiliary screw in situ.

- Lateral view showing auxiliary screw in situ and improved anterior cortical alignment.
-
AP view showing auxiliary screw in situ.
4. Cephalomedullary Lag Screw Insertion
- Guidewire Placement: A guidewire for the cephalomedullary lag screw is inserted through the targeting device of the IMN. Ensure optimal position in the femoral head: central or slightly inferior-central on AP view, and central on lateral view, with a TAD <25mm. The auxiliary screw should not interfere with the optimal placement of the lag screw.
- Reaming and Screw Insertion: Ream over the guidewire to the appropriate depth, followed by insertion of the lag screw. Apply controlled impaction if the nail design allows for dynamic compression.
- Distal Locking: Once the proximal fixation is complete, distal locking screws are inserted through the targeting device to provide rotational stability and prevent distal migration of the nail. The number and configuration (static/dynamic) of distal screws depend on the implant system and fracture pattern.
5. Final Assessment and Wound Closure
-
Final Fluoroscopy:
Obtain comprehensive AP and lateral fluoroscopic images of the entire construct to confirm optimal implant position, reduction, and absence of iatrogenic fractures.

- Pre-operative vs. Post-operative comparison with auxiliary screw demonstrating reduction and fixation.
- Wound Irrigation: Thoroughly irrigate the surgical sites.
- Closure: Close the fascial layers, subcutaneous tissue, and skin in a standard layered fashion. Apply sterile dressings.
Complications & Management
Despite advancements in surgical techniques and implants, intertrochanteric fractures treated with intramedullary nails are still associated with a spectrum of complications. The auxiliary screw technique aims to specifically mitigate some of the most detrimental failures.
Common Complications and Management
| Complication | Incidence | Etiology | Management |
|---|---|---|---|
| Screw Cutout | 3-12% | Poor reduction (especially anterior cortical gap), high TAD (>25mm), inadequate implant placement (superior-posterior), severe osteoporosis, early aggressive weight-bearing on unstable construct. | Primary prevention via auxiliary screw technique. If occurred: Revision IMN (if bone stock allows), hemiarthroplasty or total hip arthroplasty (THA) in young/active patients, Girdlestone resection arthroplasty in low-demand patients. |
| Excessive Lag Screw Sliding | 5-10% | Inadequate reduction, unstable fracture pattern, poor bone quality, premature weight-bearing, poor engagement of the lag screw within the femoral head. | If significant sliding leading to shortening/malunion: Revision fixation with bone grafting, conversion to THA. Minor sliding without functional deficit may be observed. |
| Nonunion | <5% | Poor reduction, significant comminution, distraction at fracture site, infection, compromised biology, inadequate fixation stability. | Debridement, revision fixation with bone grafting (autograft/allograft), plate augmentation, or conversion to THA depending on patient factors and bone stock. |
| Malunion (Varus, Shortening, Rotation) | Varies, up to 10-20% | Inadequate reduction (especially rotational), failure to maintain reduction intraoperatively, implant failure, excessive collapse. | Asymptomatic malunion may be observed. Symptomatic malunion (pain, gait disturbance, leg length discrepancy, functional limitation) may require corrective osteotomy or THA. |
| Z-effect/Reverse Z-effect | <5% | Specific to dual-screw cephalomedullary nails; occurs when one screw migrates superiorly and the other inferiorly (Z-effect) or vice-versa (reverse Z-effect). | Revision to a single-screw IMN or conversion to THA. |
| Periprosthetic Fracture | 1-3% | Stress riser at nail tip (distal or proximal), inadequate nail length, high energy trauma, removal of implant. | Open reduction and internal fixation with plates and screws around the nail, or revision to a longer nail depending on fracture location and morphology. |
| Infection | 1-5% | Surgical site contamination, patient comorbidities (diabetes, malnutrition), prolonged operative time, poor sterile technique. | Early: Surgical debridement, pulsed lavage, IV antibiotics, implant retention if stable. Late/Chronic: Implant removal, debridement, IV antibiotics, Girdlestone resection or two-stage THA. |
| Deep Venous Thrombosis (DVT) / Pulmonary Embolism (PE) | 10-30% (DVT), 1-5% (PE) | Immobility, surgical trauma, hypercoagulable state. | Prophylactic anticoagulation is standard. If occurred: Therapeutic anticoagulation, IVC filter in select cases. |
| Trochanteric Pain | Up to 20% | Nail prominence, irritation of the greater trochanteric bursa or gluteal tendons, soft tissue impingement. | Conservative management (NSAIDs, physiotherapy, injections). If persistent and debilitating: Implant removal after fracture healing (typically 12-18 months post-op). |
| Avascular Necrosis (AVN) of Femoral Head | Rare | Direct vascular injury during surgery, severe fracture displacement with disruption of blood supply (less common in ITFs than femoral neck fractures). | Conservative management in early stages. Core decompression, osteotomy, or joint replacement (THA) for advanced stages. |
-
Screw Cutout: This remains the most devastating mechanical complication. It signifies failure of the lag screw to hold within the femoral head, leading to its protrusion into the joint. Cutout is directly addressed by the auxiliary screw technique, which aims to provide immediate and sustained interfragmentary compression across the anterior cortical defect, thus preventing the toggling and shearing forces that typically initiate cutout.

-
Z-effect/Reverse Z-effect: While less common with modern single-screw IMNs, this phenomenon can occur in systems utilizing two separate screws for femoral head fixation. It indicates differential migration of the screws due to unstable fixation.

-
Other Complications: Malunion, particularly in varus, shortening, or rotation, can significantly impact gait and function. Nonunion, though infrequent, necessitates revision surgery. Periprosthetic fractures are a concern, often occurring at the tips of the nail or in osteoporotic bone. Infection, DVT/PE, and trochanteric pain are general surgical risks requiring diligent prophylactic and management strategies.

Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is integral to achieving optimal functional outcomes and preventing secondary complications. Protocols are tailored to individual patient factors, fracture stability, bone quality, and the security of fixation. The enhanced stability offered by the auxiliary screw technique often permits more aggressive early mobilization.
Immediate Post-Operative Period (Day 0-7)
- Pain Management: Administer multimodal analgesia to control pain effectively, facilitating early mobilization.
- Deep Venous Thrombosis (DVT) Prophylaxis: Continue pharmacological and mechanical prophylaxis (e.g., sequential compression devices).
-
Early Mobilization:
- Out of Bed: Encourage sitting at the bedside or in a chair within 24 hours of surgery.
-
Weight-Bearing:
- Weight-Bearing as Tolerated (WBAT): This is the goal for most patients treated with IMN and the auxiliary screw technique, given the anticipated stable fixation and bone-to-bone contact. WBAT allows for immediate partial or full weight-bearing based on patient comfort and tolerance.
- Touch-Down Weight Bearing (TDWB) / Partial Weight Bearing (PWB): May be prescribed for highly comminuted or extremely unstable fractures, severe osteoporosis, or if intraoperative stability was suboptimal. PWB typically involves 25-50% body weight.
- Assistive Devices: Patients are instructed in the safe use of a walker or crutches.
-
Physical Therapy (PT):
- Range of Motion (ROM): Initiate gentle active and passive ROM exercises for the hip, knee, and ankle on the operated side.
- Strengthening: Begin isometric quadriceps and gluteal muscle contractions.
- Gait Training: Supervised gait training with appropriate weight-bearing precautions.
- Wound Care: Monitor surgical wound for signs of infection or hematoma. Dressing changes as per protocol.
Sub-Acute Rehabilitation (Week 2 - Month 3)
- Progression of Weight-Bearing: Gradually advance weight-bearing as tolerated, transitioning from PWB to WBAT if initially restricted. Radiographic signs of healing (e.g., callus formation) at 6-8 weeks can guide progression.
-
Intensified PT Program:
- Strengthening: Progress to active-assisted and active resistive exercises for hip abductors, adductors, flexors, extensors, and knee musculature.
- Balance and Proprioception: Incorporate exercises to improve balance and coordination, crucial for fall prevention.
- Functional Training: Focus on activities of daily living (ADLs) such as stair climbing, getting in/out of bed, and transferring.
- Discharge Planning: Assess home environment for safety and identify needs for adaptive equipment or home health services.
Long-Term Rehabilitation (Month 3 - Month 12+)
- Full Weight-Bearing: Most patients should be on full weight-bearing by 3 months post-op, or when radiographic union is confirmed.
- Advanced Strengthening and Conditioning: Continue a progressive strengthening program to regain full muscle strength and endurance.
- Return to Activity: Gradually return to recreational activities, avoiding high-impact sports until complete union and full strength are achieved, typically after 6-12 months.
- Fall Prevention: Reinforce fall prevention strategies, including home modifications, regular exercise, and medication review.
Follow-up Schedule
- 2 Weeks: Clinical wound check, suture/staple removal.
- 6 Weeks: Clinical assessment, AP and lateral radiographs to assess early healing and implant stability.
- 3 Months: Clinical and radiographic review to confirm progressive union.
- 6 Months: Clinical and radiographic review, assess functional recovery.
- 12 Months: Final clinical and radiographic assessment. Consider implant removal if symptoms related to the implant are present and the fracture is fully healed.
The adoption of the auxiliary screw technique, by optimizing initial reduction and providing enhanced stability, allows for earlier and more confident progression to weight-bearing as tolerated, potentially shortening rehabilitation times and improving overall patient satisfaction and functional recovery.
Summary of Key Literature / Guidelines
The management of intertrochanteric fractures has evolved significantly, with intramedullary nailing (IMN) now widely regarded as the gold standard for unstable patterns. This position is supported by numerous studies demonstrating IMN's biomechanical superiority over extramedullary devices like the Dynamic Hip Screw (DHS) in unstable fractures (AO/OTA 31-A2 and 31-A3), primarily due to its central load-sharing mechanism and shorter lever arm, which reduces bending moments and minimizes varus collapse.
Key Literature Insights:
- IMN vs. DHS: Meta-analyses and randomized controlled trials consistently show that IMN is associated with lower rates of implant failure, reoperation, and better functional outcomes for unstable ITFs compared to DHS. For stable ITFs (AO/OTA 31-A1), both implants can achieve good results, but IMN is often preferred due to its less invasive approach and potential for faster rehabilitation.
- Importance of Reduction Quality: A recurrent theme across the literature is the critical impact of reduction quality on outcomes. Studies by Baumgaertner et al. (1995) established the concept of Tip-Apex Distance (TAD), demonstrating that a TAD > 25mm significantly increases the risk of lag screw cutout. Subsequent research has reinforced that poor reduction, particularly in the frontal and sagittal planes, is an independent risk factor for mechanical failure, regardless of implant type.
- The "Anterior Cortical Gap" Problem: Specific attention has been drawn to the challenge of achieving anatomical reduction of the anterior cortex. While AP radiographs may appear satisfactory, lateral views often reveal a persistent anterior cortical gap or step-off. This residual displacement compromises rotational stability and exposes the cephalomedullary screw to excessive shear forces, leading to cutout, especially in osteoporotic bone. Early work by investigators like Kaufer (1980) highlighted the biomechanical significance of the posteromedial cortex, but increasingly the anterior cortical integrity is recognized as equally vital for a truly stable construct, preventing anterior-posterior toggling. Techniques to address this have been explored, ranging from open reduction with direct clamps to specific reduction maneuvers, yet a universally adopted, simple, and effective percutaneous solution has been lacking.
- Adjunctive Fixation Techniques: Various adjunctive techniques have been proposed to enhance stability in comminuted or unstable ITFs, including cement augmentation of the lag screw, adjunctive screws for lateral wall reconstruction, or using a second cephalic screw in specific nail designs. While these can improve stability in select cases, they often add complexity, cost, or are not specifically designed to address the biomechanical instability caused by the anterior cortical gap.
- Failure Rates and Prognosis: Despite advances, overall failure rates for unstable ITFs fixed with IMN remain between 3-12%, primarily due to mechanical complications like cutout and excessive sliding. These failures are particularly devastating for elderly, frail patients, often necessitating revision surgery with significantly poorer outcomes and higher mortality.
Current Guidelines:
- AAOS (American Academy of Orthopaedic Surgeons): Guidelines recommend surgical fixation for nearly all displaced ITFs, emphasizing early surgical intervention within 24-48 hours when medically appropriate. They advocate for IMN for unstable fractures, acknowledging the importance of good reduction and appropriate implant positioning (e.g., TAD).
- BOA (British Orthopaedic Association): Similar to AAOS, emphasizing IMN for unstable fractures, early mobilization, and a multidisciplinary approach to patient care.
- AO Foundation Principles: Promote anatomical or near-anatomical reduction, stable fixation, preservation of blood supply, and early, safe mobilization. The auxiliary screw technique aligns with these principles by aiming for a precise reduction and enhanced stability.
Relevance of the Innovative Auxiliary Screw Technique:
The presented innovative auxiliary screw technique directly addresses a critical and often underestimated factor in IMN failure: the residual anterior cortical gap. By providing a targeted, percutaneous method to achieve and maintain reduction of the anterior cortex, this technique offers a practical solution to a known biomechanical instability. It complements existing IMN systems by:
1.
Improving Reduction Quality:
Ensuring true bone-to-bone contact at the anterior cortex.
2.
Enhancing Stability:
Mitigating the toggling forces on the lag screw, reducing shear stress and minimizing cutout risk.
3.
Facilitating Early Rehabilitation:
By creating a more robust and stable construct, it allows for more confident early weight-bearing, which is crucial for elderly patients.
While biomechanical rationale and preliminary clinical observations support its efficacy, further robust prospective studies and randomized controlled trials are warranted to fully validate its impact on reducing complication rates and improving long-term patient outcomes compared to standard IMN techniques alone. This innovative approach holds significant promise in refining the surgical management of intertrochanteric fractures, pushing the boundaries of precision and stability.
Clinical & Radiographic Imaging
You Might Also Like