Arthroscopic Management of Posterior Horn and Complex Meniscal Tears
Key Takeaway
Arthroscopic management of posterior horn meniscal tears requires meticulous technique to preserve functional tissue while eliminating mechanical symptoms. Utilizing a 15-degree up-biting basket forceps through an ipsilateral portal facilitates precise resection. This guide details the step-by-step surgical approaches for bucket-handle, horizontal, radial, and complex tears, emphasizing biomechanical preservation, meniscal cyst decompression, and evidence-based postoperative rehabilitation protocols for optimal patient outcomes.
Introduction to Meniscal Preservation and Resection
The meniscus plays an indispensable role in the biomechanics of the knee, providing load transmission, shock absorption, joint stability, and articular cartilage lubrication. Historically, total meniscectomy was the standard of care for meniscal pathology, inevitably leading to early-onset osteoarthritis and altered joint kinematics. Contemporary orthopedic surgery strictly adheres to the principle of "maximum preservation of functional meniscal tissue."
When evaluating meniscal tears—particularly those involving the posterior horn, bucket-handle configurations, or complex degenerative patterns—the surgeon must meticulously balance the need to excise unstable, symptom-producing fragments with the imperative to retain a stable, contoured peripheral rim. This comprehensive guide details the advanced arthroscopic techniques required for the management of posterior horn tears, bucket-handle displacements, and complex meniscal lesions.
Biomechanical Considerations
Understanding meniscal biomechanics is critical when performing an arthroscopic partial meniscectomy. The menisci convert axial compressive forces into circumferential "hoop stresses." This function is primarily dependent on the integrity of the peripheral rim and the anterior and posterior root attachments.
Clinical Pearl: Resection of the inner third of the meniscus decreases contact area by approximately 10%, whereas total meniscectomy decreases contact area by up to 75%, exponentially increasing peak contact stresses on the articular cartilage. Therefore, all resections must be limited to the avascular, unstable portions of the tear, preserving the peripheral hoop tension mechanism.
Preoperative Evaluation and Patient Positioning
Imaging and Diagnostics
Magnetic Resonance Imaging (MRI) remains the gold standard for preoperative evaluation. It allows the surgeon to classify the tear pattern (horizontal, radial, longitudinal, complex), assess for associated meniscal cysts, and evaluate the integrity of the meniscal roots.
Operating Room Setup
- Anesthesia: General or regional anesthesia is utilized based on patient comorbidities and surgeon preference.
- Positioning: The patient is placed supine on the operating table. A lateral post or a leg holder is applied to the proximal thigh to allow for valgus stress (for medial compartment access) and varus stress (for lateral compartment access).
- Tourniquet: A pneumatic tourniquet is placed proximally but is often left uninflated unless visualization is compromised by bleeding.
- Portals: Standard anterolateral (viewing) and anteromedial (working) portals are established. Accessory portals may be required depending on the tear location and complexity.
Surgical Technique: Removal of Posterior Horn Tears
Posterior horn tears are among the most common meniscal pathologies and can be technically demanding to access due to the convex geometry of the femoral condyles and the tight posterior joint space.
Instrumentation and Approach
To facilitate the removal of a posterior horn tear, specialized instrumentation is required. Standard straight biters often fail to reach the posterior-most extent of the tear without causing iatrogenic scuffing of the chondral surfaces.
- The 15-Degree Up-Biting Basket: Use a 15-degree up-biting, low-profile basket forceps. The upward angle matches the contour of the posterior femoral condyle, allowing the jaws to engage the meniscal tissue safely.
- Portal Selection: Carry the resection out through the ipsilateral portal. For a medial posterior horn tear, the anteromedial portal is the primary working portal.
Step-by-Step Resection
- Probing: Thoroughly probe the posterior horn to delineate the extent of the tear. Identify the transition zone between healthy, stable tissue and the degenerative, mobile fragment.
- Piecemeal Resection: Introduce the 15-degree up-biting basket. Begin resecting the unstable leaflet bit by bit.
- Contouring: Trim the meniscus back to a stable, contoured peripheral rim. Avoid creating sharp angles or "dog ears," which can act as stress risers and propagate future tears.
- Final Evaluation: Use a motorized shaver (typically 4.0 mm or 4.5 mm) on a low oscillation setting to smooth the resected edge. Probe the remaining rim to ensure no hidden unstable fragments remain.
Surgical Warning: Over-resection of the posterior horn, particularly near the posterior root attachment, can completely defunctionalize the meniscus, leading to rapid chondrolysis. Always err on the side of preservation.
Surgical Technique: Bucket-Handle Tears (Two-Portal Technique)
Bucket-handle tears represent a displaced longitudinal tear where the inner fragment migrates into the intercondylar notch, often causing mechanical locking of the knee. While repair is always the first choice in young patients with tears in the red-red or red-white zones, chronic, deformed, or white-white zone tears often require resection.
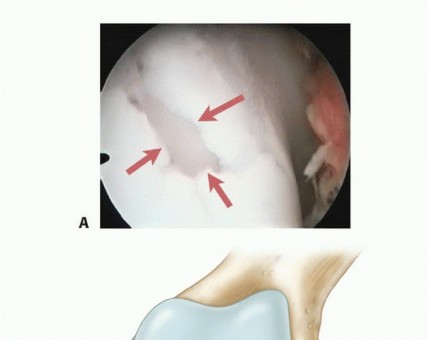
Step 1: Probing and Assessment
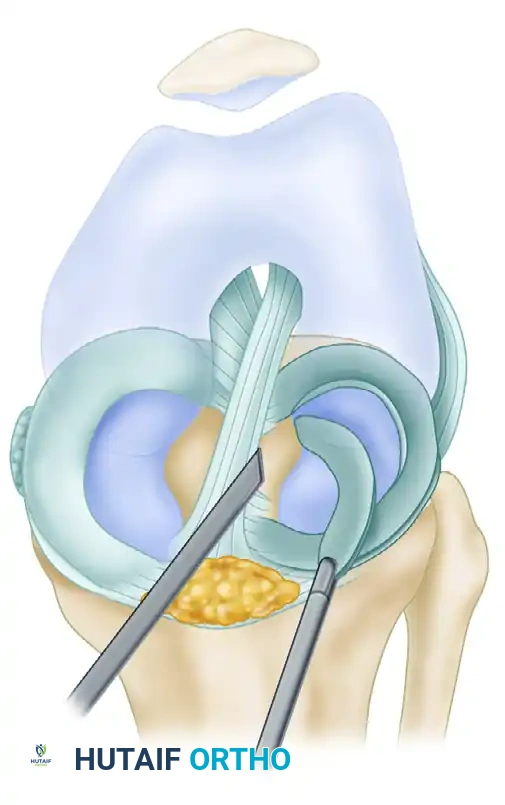
The displaced bucket-handle tear is first visualized and probed to assess its mobility, tissue quality, and the exact locations of its anterior and posterior attachments.
A, Displaced bucket-handle tear of the lateral meniscus being probed to assess mobility and attachment points.
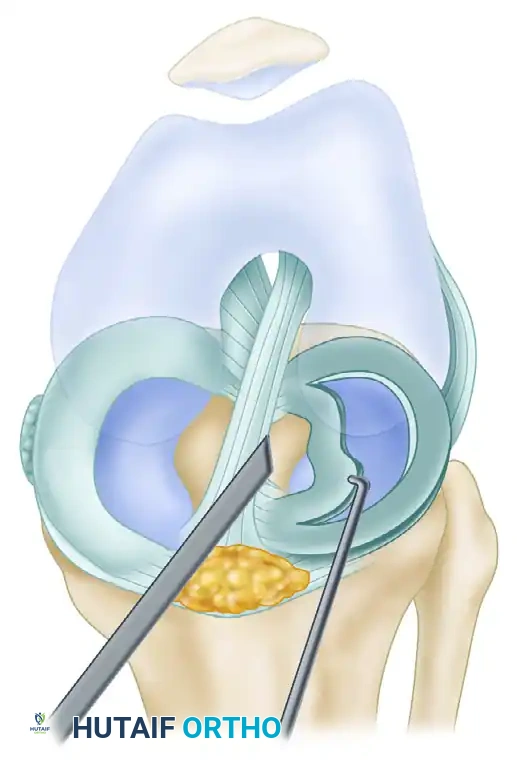
Step 2: Reduction
Before resection, the displaced fragment must be reduced back to its anatomical position. This is achieved using a blunt probe or the closed jaws of a grasper. Reduction allows the surgeon to accurately visualize the anterior and posterior hinges.
Step 3: Posterior Attachment Release
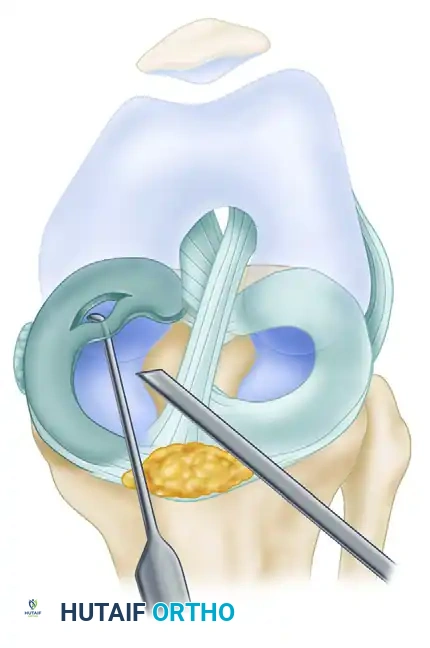
Once reduced, the posterior attachment is addressed first. Using arthroscopic scissors or a narrow punch, the posterior attachment is partially released. It is crucial not to completely transect the posterior attachment at this stage, as doing so will allow the fragment to float freely in the joint, making the anterior release exceedingly difficult.
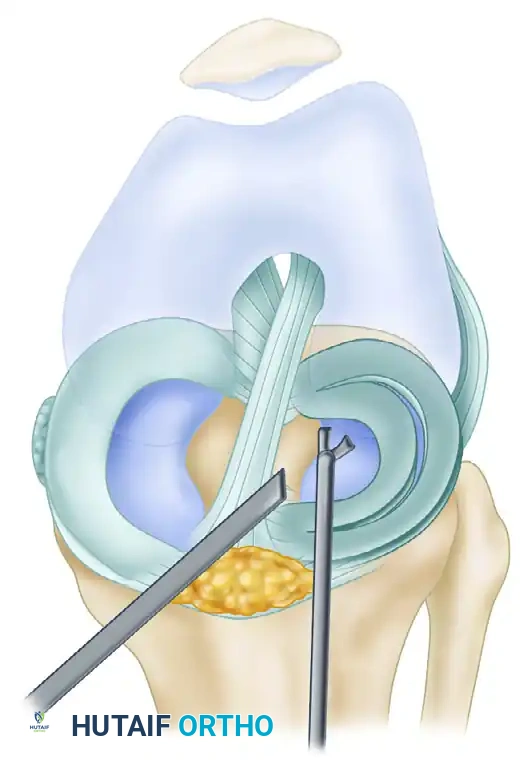
B, After reduction of the displaced bucket-handle tear, the posterior attachment is partially released with arthroscopic scissors.
Step 4: Anterior Attachment Release
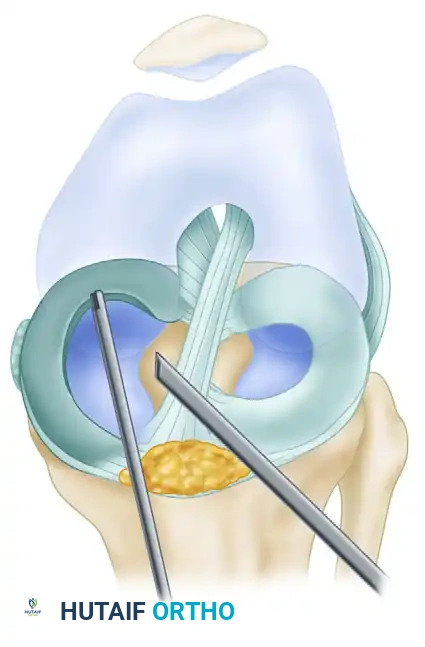
With the posterior hinge partially intact to provide tension, the surgeon moves to the anterior attachment. Using scissors or a basket forceps, the anterior attachment is completely released.
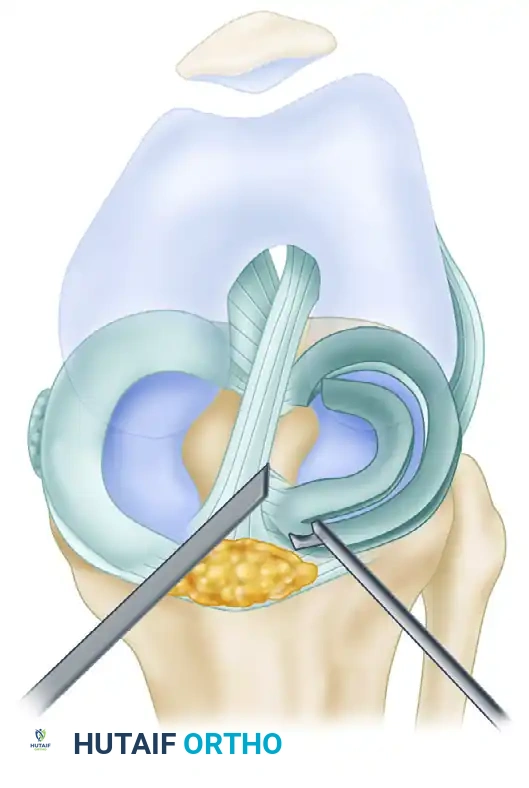
C, The anterior attachment is completely released with scissors while the posterior hinge maintains tissue tension.
Step 5: Avulsion and Extraction
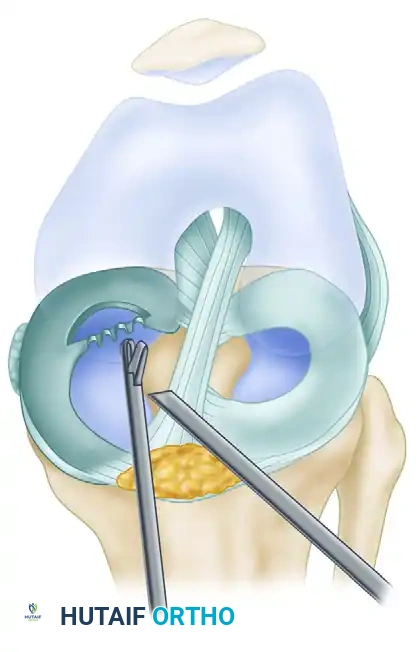
The surgeon then introduces a heavy arthroscopic grasper. The freed anterior aspect of the fragment is securely grasped. By applying a firm, twisting traction force, the tenuous remaining posterior attachment is avulsed, and the entire bucket-handle fragment is extracted through the portal.
D, The tenuous remaining posterior attachment is avulsed with a grasper, and the fragment is extracted from the joint.
Surgical Technique: Longitudinal Incomplete Intrameniscal Tears
Incomplete longitudinal tears often present on the inferior surface of the meniscus and may not be immediately visible from a superior viewing angle.
Identification and Probing
Thorough probing of the inferior meniscal surface is mandatory. The probe tip is hooked under the meniscus and pulled anteriorly to reveal hidden clefts.
A, Probing a longitudinal intrameniscal incomplete inferior surface tear.
Resection Strategy
Once identified, the unstable inferior leaflet is removed. This is typically done piecemeal using a low-profile basket forceps.
B, The unstable fragment is removed bit by bit with basket forceps, taking care to preserve the superior stable tissue.
Smoothing and Contouring
After the gross unstable tissue is removed, the remaining meniscal rim must be contoured to prevent further propagation. A motorized trimmer is utilized to create a smooth transition zone.
C, The meniscal rim is smoothed and contoured with a motorized trimmer to eliminate stress risers.
Management of Horizontal, Oblique, Radial, and Complex Tears
In evaluating horizontal, oblique, radial, and complex tears, the overarching surgical philosophy remains imperative: evaluate meticulously and remove only damaged tissue while maintaining functional, healthy meniscal tissue.
Horizontal Tears and Meniscal Cysts
Horizontal cleavage tears split the meniscus into superior and inferior leaves. With horizontal tears of long-term duration, a meniscal cyst may develop due to synovial fluid being pumped through the meniscal cleft into the parameniscal tissues.
- Preoperative Identification: The presence of a cyst is generally evident on preoperative MRI and should be actively looked for during the arthroscopic examination.
- Resection: In most instances, the unstable portions of both the superior and the inferior leaves are resected back to relatively normal, stable tissue.
- Cyst Decompression: The horizontal cleft must be probed. If a meniscal cyst is present, it must be decompressed to prevent recurrence of pain and swelling.
- A small curved curet may be placed through the cleft, aimed toward the surgeon’s finger palpating the exterior extent of the meniscal cyst on the joint line.
- The cyst can be opened with the curet and drained directly into the knee joint.
- Alternatively, a shaver (used with suction but without running the oscillating blades) can be used to open and decompress the cyst.
- Localization can also be aided by placing a spinal needle percutaneously from the exterior directly into the cyst under arthroscopic visualization.
Flap Tears
Flap tears are highly mobile and notorious for causing acute mechanical catching.
- Evaluation Pitfalls: When evaluating flap tears, one must probe the meniscus at the tear site carefully. Often, a flap can roll up under the normal portion of the meniscus, obscuring its true size and contour.
- Hidden Flaps: Likewise, a flap can flip posteriorly, hiding behind the femoral condyle. Careful examination of the posterior compartments (often requiring a 70-degree arthroscope or a trans-notch view) is necessary to evaluate these meniscal tears fully.
- Resection: Resection of a flap tear or a complex degenerative tear is generally accomplished with a basket forceps to morcellize the tear. Careful probing is done repeatedly during the resection to ensure that the remaining meniscal tissue is of relatively normal contour with a smooth transition at its edges.
Radial Tears
Radial tears disrupt the circumferential collagen fibers of the meniscus, directly compromising its ability to withstand hoop stresses. They are divided into partial and complete tears.
- Partial Radial Tears: A partial-depth radial tear of the meniscus is treated with saucerization. The sharp corners of the tear are rounded off, balancing and contouring the edges to prevent the tear from propagating further toward the capsule.
- Complete Radial Tears: Complete radial tears that extend all the way to the meniscosynovial junction present a difficult biomechanical problem. Resection of a complete radial tear essentially defunctionalizes the entire meniscus, acting biomechanically similar to a total meniscectomy.
- Repair Indications: Because resection results in the loss of the functional protective mechanism of the meniscus, many authors and current evidence-based guidelines dictate that horizontal mattress repair of the peripheral portion of the meniscus is indicated for complete radial tears, even if they extend into the avascular zone, to restore hoop tension.
Clinical Pearl: When saucerizing a partial radial tear, ensure the transition zone is wide and gradual. A sharp, narrow V-shaped resection will concentrate stress at the apex, leading to rapid tear propagation.
Postoperative Care and Rehabilitation Protocol
The postoperative care following an arthroscopic partial meniscectomy (including the removal of posterior horn tears, bucket-handle resections, and complex tear debridement) is focused on controlling inflammation, restoring range of motion (ROM), and progressively reloading the joint.
Phase 1: Immediate Postoperative (Weeks 0-2)
- Weight-Bearing: Patients are generally allowed weight-bearing as tolerated (WBAT) immediately postoperatively, often with the assistance of crutches for the first few days until normal gait mechanics are restored.
- Bracing: No brace is typically required for isolated partial meniscectomies.
- Range of Motion: Immediate emphasis is placed on achieving full terminal extension (to prevent arthrofibrosis) and progressive flexion.
- Therapy: Cryotherapy, elevation, and isometric quadriceps strengthening (quad sets, straight leg raises) are initiated on postoperative day one.
Phase 2: Intermediate Rehabilitation (Weeks 2-4)
- Gait: Discontinue crutches once the patient demonstrates a non-antalgic gait and good quadriceps control.
- Strengthening: Transition to closed kinetic chain exercises (mini-squats, leg presses, stationary cycling).
- Proprioception: Initiate balance and proprioceptive training.
Phase 3: Return to Activity (Weeks 4-6+)
- Advanced Strengthening: Progress to dynamic, multi-planar movements.
- Sport-Specific Training: Introduce agility drills, light plyometrics, and sport-specific functional activities.
- Clearance: Return to full competitive sports or heavy manual labor is typically permitted between 4 to 6 weeks, provided the patient has full, painless ROM, no effusion, and isokinetic strength testing demonstrates at least 90% symmetry compared to the contralateral limb.
Note: If a meniscal repair was performed (e.g., for a complete radial tear or a reducible bucket-handle tear in the vascular zone), the postoperative protocol is significantly altered, typically requiring restricted weight-bearing and limited flexion for 4 to 6 weeks to protect the repair construct.
📚 Medical References
You Might Also Like