Meniscal Preservation and Restoration: Fibrin Clot Augmentation and Allograft Transplantation
Key Takeaway
Meniscal allograft transplantation and fibrin clot augmentation are advanced techniques for managing meniscal deficiency and complex tears. Fibrin clots provide essential growth factors to avascular zones, enhancing healing in isolated repairs. For post-meniscectomy syndrome, meniscal allografts offer significant symptomatic relief. This guide details the Port et al. fibrin clot preparation method and the University of Pittsburgh meniscal transplantation technique, emphasizing strict patient selection, precise graft sizing, and meticulous surgical execution.
BIOLOGICAL AUGMENTATION IN MENISCAL REPAIR
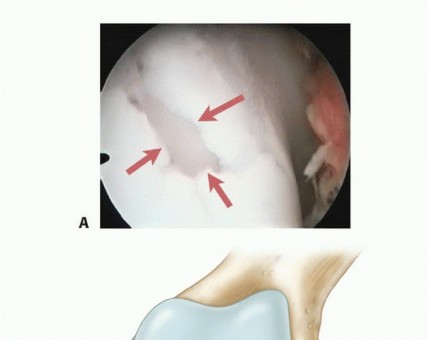
The preservation of meniscal tissue is a paramount objective in contemporary orthopedic surgery, given the meniscus's critical role in load transmission, shock absorption, joint stability, and articular cartilage nutrition. While tears in the peripheral vascularized zone (the "red-red" zone) demonstrate excellent healing potential following primary repair, lesions extending into the avascular inner two-thirds (the "red-white" and "white-white" zones) present a profound biological challenge.
To address the limited intrinsic healing capacity of the avascular meniscus, biological augmentation techniques have been developed. Among these, the application of an exogenous fibrin clot remains a highly effective, low-cost, and biologically robust method to introduce chemotactic and mitogenic factors directly into the repair site.
Rationale and Indications for Fibrin Clot Application
Although the exact molecular mechanisms by which a fibrin clot or platelet-rich plasma (PRP) facilitates meniscal healing continue to be investigated, the prevailing consensus is that the clot acts as both a bioactive scaffold and a delivery vehicle. It provides a concentrated source of platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), and fibronectin, which collectively stimulate fibrochondrocyte proliferation, migration, and extracellular matrix synthesis.
Clinical Pearl: Fibrin clot augmentation is highly recommended when repairing isolated meniscal tears located 3 to 5 mm from the meniscosynovial junction (the red-white and white-white zones).
Conversely, when a meniscal repair is performed concomitantly with an anterior cruciate ligament (ACL) reconstruction, the addition of an exogenous fibrin clot is generally deemed unnecessary. The intra-articular drilling of femoral and tibial tunnels generates a nutrient- and stem-cell-rich hemarthrosis that bathes the meniscal repair site, effectively providing an endogenous clot and rendering exogenous augmentation redundant.
Preparation of the Fibrin Clot (Port et al. Technique)
The preparation of a structurally sound fibrin clot requires meticulous technique to ensure the clot possesses sufficient tensile strength to be handled, sutured, and implanted without disintegrating. The technique described by Port et al. remains the gold standard.
- Blood Draw and Syringe Selection: Using standard venipuncture, obtain an aliquot of 5 to 10 mL of whole autologous blood. The choice of syringe dictates the final geometry of the clot:
- Transfer to a 20-mL or 60-mL plastic syringe to form a shorter, thicker clot (ideal for radial or short longitudinal tears).
- Transfer to a 10-mL syringe to form a longer, thinner clot (ideal for extended bucket-handle or long longitudinal tears).
- The Stirring Process: Utilize a 4-mm frosted glass stirring rod. If a frosted rod is unavailable, a smooth glass rod can be prepared by aggressively abrading it with fine-grit corundum paper (ensure the rod is washed thoroughly with sterile saline before use).
- Insert the rod into the blood and gently stir in small, continuous circles.
- Crucial Step: Avoid any contact between the glass rod and the outer plastic wall of the syringe. Contact will cause premature sloughing and fragmentation of the forming clot.
- Temperature Regulation: Use your non-stirring hand to encircle the barrel of the syringe. The ambient body heat transferred from your hand accelerates the coagulation cascade. Place your fifth digit over the distal tip of the syringe to prevent blood loss.
- Clot Maturation: Within 3 to 5 minutes, a palpable change in the fluid's consistency will occur, indicating that fibrin polymerization has begun around the rod.
- Consolidation: Once the clot has formed, gently bring the rod to the wall of the syringe, allowing the clot to contact the plastic. Apply a gentle, radially directed force while continuing to make small circles. This action mechanically tightens and compresses the fibrin matrix.
- Extraction: After an additional 1 to 2 minutes of consolidation, carefully withdraw the rod with the adherent clot. Slide the clot off the rod onto a sterile gauze sponge. Gently blot the clot to express residual serum.
Surgical Warning: Do not aggressively squeeze the clot with instruments during extraction. Gentle blotting with gauze is sufficient. Once prepared, the clot can be used immediately or stored temporarily in saline-soaked gauze. A properly formed clot is highly cohesive; it can be stretched, manipulated, and squeezed with reasonable force without losing its structural integrity, and it is fully capable of holding sutures.
Surgical Delivery and Fixation of the Fibrin Clot
Delivering the clot into the aqueous environment of the knee joint requires precision to prevent it from being washed away or fragmented.
- Delivery Methods:
- Direct Insertion: Place the clot between the torn edges of the meniscus using a specialized plastic delivery tube and a pusher.
- Needle Delivery: Insert the clot through the barrel of a syringe attached to a large-bore 14-gauge spinal needle, injecting it directly into the tear interface.
- Suture Shuttle Technique: Place 0-0 polydioxanone (PDS) sutures into each end of the clot. Using meniscal repair needles, pass these sutures down a cannula, under the body of the meniscus, and out through the joint capsule. One suture is placed at the anterior extent of the tear, and the second at the posterior extent. Gently tease the clot into the tear interface by applying tension to the sutures.
- Fluid Management: During clot placement by any of these means, it is imperative to turn off the arthroscopic fluid inflow and drain the knee. Attempting to place a clot under high fluid pressure will inevitably result in clot disruption and displacement.
- Final Fixation: Once the clot is perfectly positioned between the torn meniscal edges, secure it by reapproximating the meniscus using previously placed inside-out or all-inside mattress repair sutures.
MENISCAL ALLOGRAFT TRANSPLANTATION (MAT)
When meniscal tissue is irreparably damaged or has been previously excised, the knee is subjected to exponentially increased contact stresses, inevitably leading to early-onset osteoarthritis. Meniscal replacement continues to evolve, transitioning from soft-tissue-only fixation to advanced bone-plug and bone-bridge techniques with strictly defined indications.
Clinical Outcomes and Biomechanics
The primary goal of Meniscal Allograft Transplantation (MAT) is to relieve pain and improve function in the post-meniscectomy knee. Current literature demonstrates that MAT provides excellent symptomatic relief, with asymptomatic results reported in over 90% of properly selected patients in the short to medium term.
However, the degree of chondroprotective function provided by a transplanted meniscus remains a subject of intense academic debate. While biomechanical studies show that MAT restores contact mechanics to near-normal levels, long-term clinical graft failure rates have historically ranged from 21% to 60%.
In a landmark study by Verdonk et al., a 7.2-year follow-up of 100 MAT procedures revealed that while 70% of patients maintained asymptomatic relief, approximately one-third required additional surgery for meniscal tears, shrinkage, or impingement. Furthermore, the functional relief provided by MAT is often confounded by the fact that many patients undergo concomitant procedures—such as high tibial osteotomy (HTO) for realignment, ACL reconstruction for stabilization, or osteochondral autograft/allograft transplantation—at the time of the meniscal transplant.
Indications and Patient Selection
Patient selection is the single most critical determinant of success in MAT. The ideal candidate fits a highly specific clinical profile.
Primary Indications:
* Prior total or subtotal meniscectomy.
* Age 50 years or younger (physiologically young).
* Symptoms (pain, swelling) strictly localized to the meniscectomized tibiofemoral compartment.
* No advanced arthrosis: The joint space must be 2 mm or greater on a standing 45-degree posteroanterior (PA) flexion weight-bearing radiograph. There should be no flattening of the femoral condyles or excessive osteophyte formation.
Absolute and Relative Contraindications:
* Uncorrected axial malalignment (e.g., varus alignment in a medial meniscal deficient knee).
* Uncorrected ligamentous instability.
* Advanced chondromalacia (Outerbridge Grade IV) with exposed subchondral bone on the opposing articular surfaces.
* Previous joint infection or inflammatory arthropathy.
* Obesity (BMI > 30 is a strong relative contraindication).
Clinical Pearl: The patient must be highly motivated, thoroughly informed about the salvage nature of the procedure, and willing to permanently decrease impact-loading activities (e.g., long-distance running, heavy jumping).
Graft Procurement, Processing, and Sizing
When deciding between a fresh-frozen or a cryopreserved meniscus, the surgeon must be intimately familiar with allograft procurement protocols to ensure a high-quality, young, healthy graft is secured. In a comprehensive study by Sgaglione et al., cryopreserved menisci performed similarly to fresh-frozen menisci and carried identical risks. The risk of viral disease transmission, specifically acquired immunodeficiency syndrome (AIDS), is exceptionally low, estimated at 1 in 1.6 million with modern nucleic acid testing.
Note: Investigational studies of biological tissue scaffolds (e.g., collagen meniscal implants, polyurethane scaffolds) for partial or complete meniscal replacement are ongoing. While they may provide acceptable off-the-shelf alternatives in the future, current results are limited to short-term data and specific partial-defect indications.
Graft Sizing:
Accurate sizing is non-negotiable. A graft mismatched by more than 5% will fail to restore normal hoop stresses and may cause paradoxical increased contact pressures or early graft extrusion.
* Sizing is best performed using the Pollard method on standard anteroposterior (AP) and lateral radiographs, adjusting for magnification.
* The AP view determines the coronal width of the meniscus, while the lateral view determines the sagittal length.
* Magnetic Resonance Imaging (MRI) is increasingly utilized for three-dimensional templating to determine exact meniscal coverage and bone-bridge dimensions.
SURGICAL TECHNIQUE: THE UNIVERSITY OF PITTSBURGH METHOD
The University of Pittsburgh technique is a highly regarded, reproducible method for MAT utilizing bone fixation. Best biomechanical results are consistently obtained with a meniscal allograft that has a bone block (for the lateral meniscus) or a bone bridge (for the medial meniscus) attached, as this preserves the native insertional anatomy and allows for rigid bony healing.
The technique is systematically divided into four distinct parts: Graft Preparation, Tunnel Placement, Graft Insertion, and Graft Fixation.
Part 1: Graft Preparation
Preparation occurs on the back table while the diagnostic arthroscopy is underway.
* The allograft is thawed in warm saline.
* For a medial meniscus, a bone bridge connecting the anterior and posterior horns is typically fashioned. The bridge is cut to specific dimensions (usually 7-8 mm wide and 10 mm deep) using a micro-sagittal saw.
* For a lateral meniscus, where the anterior and posterior horn insertions are anatomically closer together, a single keyhole bone plug or a cylindrical bone block is fashioned.
* Traction sutures (usually No. 2 non-absorbable high-strength sutures) are placed through the posterior horn and the junction of the posterior and middle thirds of the graft. These will serve as shuttle sutures during insertion.
Part 2: Tunnel Placement and Recipient Site Preparation
Meticulous preparation of the recipient bed is vital for graft incorporation.
* Remnant Debridement: The native meniscal remnant is debrided back to a bleeding peripheral rim (1-2 mm) to stimulate a vascular response. The native anterior and posterior horn footprints are identified and cleared of soft tissue.
* Slot/Tunnel Creation:
* For a bone bridge (Medial): A rectangular slot is created in the tibial plateau, connecting the anterior and posterior horn footprints. This is achieved using a specialized drill guide, followed by box chisels and rasps to create a precise trough that matches the dimensions of the graft's bone bridge.
* For bone plugs (Lateral): Independent anterior and posterior tibial tunnels are drilled anatomically at the native horn insertion sites using a guide pin and an 8-mm or 9-mm reamer.
Part 3: Graft Insertion
Inserting the graft requires patience and careful manipulation to avoid damaging the articular cartilage.
* An accessory medial or lateral arthrotomy is created, corresponding to the compartment receiving the graft.
* Suture passers are used to shuttle the previously placed traction sutures from the posterior horn of the graft through the posterior capsule and out through a posteromedial or posterolateral safety incision.
* By applying gentle, simultaneous tension on the posterior traction sutures and guiding the bone block/bridge into the prepared tibial slot or tunnels, the graft is smoothly reduced into the joint.
* A meniscal probe is used to ensure the graft is not folded or caught under the condyle.
Part 4: Graft Fixation
Rigid fixation of both the bone and the soft tissue is required to withstand postoperative forces.
* Bony Fixation:
* If a bone bridge/slot technique is used, the bone bridge is press-fit into the tibial trough. It can be further secured with a bioabsorbable interference screw or by tying sutures over a cortical button on the anterior tibia.
* If independent bone plugs are used, the sutures exiting the bottom of the bone plugs are tied over a bone bridge on the anteromedial tibia.
* Soft Tissue Fixation: Once the bone is secured, the periphery of the meniscal allograft is sutured to the native capsule. This is typically performed using an inside-out technique.
* Zone-specific cannulas are used to pass multiple vertical or horizontal mattress sutures (No. 2-0 non-absorbable) every 3 to 5 mm along the periphery.
* Sutures are tied over the joint capsule through the posterior safety incisions under direct visualization, ensuring the knot rests on the capsule and not within the joint space.
Postoperative Rehabilitation Protocol
The rehabilitation following MAT is conservative, designed to protect the bone-to-bone healing and the peripheral soft-tissue repair.
* Phase I (0-6 weeks): The patient is strictly non-weight-bearing (NWB) or touch-down weight-bearing. The knee is locked in full extension in a hinged brace. Range of motion (ROM) is limited to 0 to 90 degrees to prevent excessive shear forces on the posterior horn.
* Phase II (6-12 weeks): Progressive weight-bearing is initiated. The brace is unlocked, and ROM is advanced as tolerated. Closed-chain kinetic exercises begin.
* Phase III (3-6 months): Full weight-bearing without a brace. Introduction of light jogging and proprioceptive training.
* Phase IV (6+ months): Return to low-impact sports. High-impact, pivoting, and cutting sports are generally discouraged permanently to preserve the longevity of the allograft.
You Might Also Like