Masterclass in Lateral Meniscal Suturing: Advanced Surgical Techniques
Key Takeaway
Lateral meniscal suturing requires meticulous technique to restore joint biomechanics while protecting the common peroneal nerve. By maintaining the knee at 90 degrees of flexion during posterior horn repair, the nerve safely drops below the joint line. Advanced repair strategies, including inside-out vertical mattress suturing, hybrid approaches for bucket-handle tears, and transtibial root repairs, ensure robust fixation. Strict adherence to evidence-based postoperative protocols is essential for optimal meniscal healing and long-term joint preservation.
INTRODUCTION TO LATERAL MENISCAL PRESERVATION
The lateral meniscus plays an indispensable role in the biomechanical homeostasis of the knee joint. Unlike the medial meniscus, which is relatively fixed, the lateral meniscus is highly mobile, covering a larger percentage of the articular surface of the lateral tibial plateau. It transmits up to 70% of the load in the lateral compartment. Consequently, the loss of lateral meniscal tissue leads to exponentially increased contact pressures, rapid articular cartilage degradation, and early-onset osteoarthritis.
Historically, meniscectomy was the standard of care; however, contemporary orthopedic surgery mandates a preservation-first approach. Lateral meniscal suturing encompasses a variety of advanced arthroscopic techniques designed to restore the anatomical integrity and hoop stresses of the meniscus. This comprehensive guide details the indications, neurovascular considerations, step-by-step surgical techniques, and postoperative rehabilitation protocols required for successful lateral meniscal repair.
SURGICAL ANATOMY AND NEUROVASCULAR CONSIDERATIONS
The anatomy of the lateral compartment presents unique challenges during meniscal repair. The presence of the popliteus hiatus disrupts the peripheral capsular attachment of the lateral meniscus, creating a natural zone of hypermobility. Furthermore, the proximity of critical neurovascular structures demands absolute anatomical precision.
The Common Peroneal Nerve
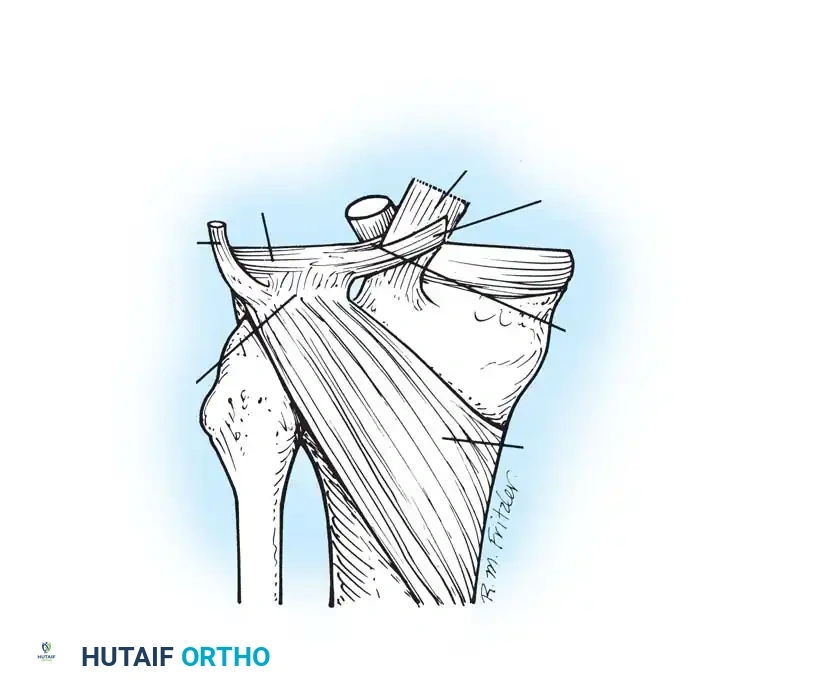
The most significant risk during lateral meniscal suturing—particularly when addressing the posterior horn and posterolateral corner—is iatrogenic injury to the common peroneal nerve. The nerve courses posterior to the biceps femoris tendon and wraps around the fibular neck.
🚨 SURGICAL WARNING: The common peroneal nerve is at extreme risk during inside-out suturing of the posterior horn of the lateral meniscus. To mitigate this risk, the surgeon must strictly maintain the knee at or near 90 degrees of flexion during needle passage. In this flexed position, the nerve falls well below the joint line, safely out of the trajectory of the exiting meniscal needles.
The Popliteus Tendon and Hiatus
When repairing tears in the middle third of the lateral meniscus, surgeons must be cognizant of the popliteus tendon. Sutures passed blindly through the popliteus hiatus can inadvertently capture the popliteus tendon, leading to postoperative stiffness, pain, and restricted internal tibial rotation. Needles must enter and exit the capsule superior to the palpable biceps femoris tendon and carefully avoid tethering the popliteus.
PATIENT POSITIONING AND SETUP
Proper patient positioning is critical for both joint access and neurovascular protection.
- Anesthesia and Tourniquet: The procedure is typically performed under general or regional anesthesia. A proximal thigh tourniquet is applied but inflated only if visualization is compromised by bleeding.
- Leg Positioning: The patient is positioned supine with the operative leg in a standard arthroscopic leg holder or resting over a lateral post.
- The Figure-Four Position: To access the lateral compartment, the knee is placed in the "figure-four" position (hip flexed, abducted, and externally rotated, with the knee flexed to 90 degrees). This position opens the lateral joint space by applying a varus stress and naturally protects the peroneal nerve by maintaining 90 degrees of knee flexion.
SURGICAL TECHNIQUES FOR LATERAL MENISCAL SUTURING
The technique selected depends on the tear pattern, location (red-red, red-white, or white-white zone), and chronicity. The fundamental goal is to achieve stable, anatomic reduction using a stacked vertical mattress configuration whenever possible, as this construct provides the highest biomechanical pull-out strength.
The Inside-Out Technique
The inside-out technique remains the gold standard for repairing tears of the posterior horn and the middle third of the lateral meniscus.
- Preparation: The tear edges and the adjacent parameniscal synovium are aggressively debrided using an arthroscopic shaver and a meniscal rasp. This synovial rasping stimulates a bleeding response, introducing mesenchymal stem cells and growth factors into the repair site.
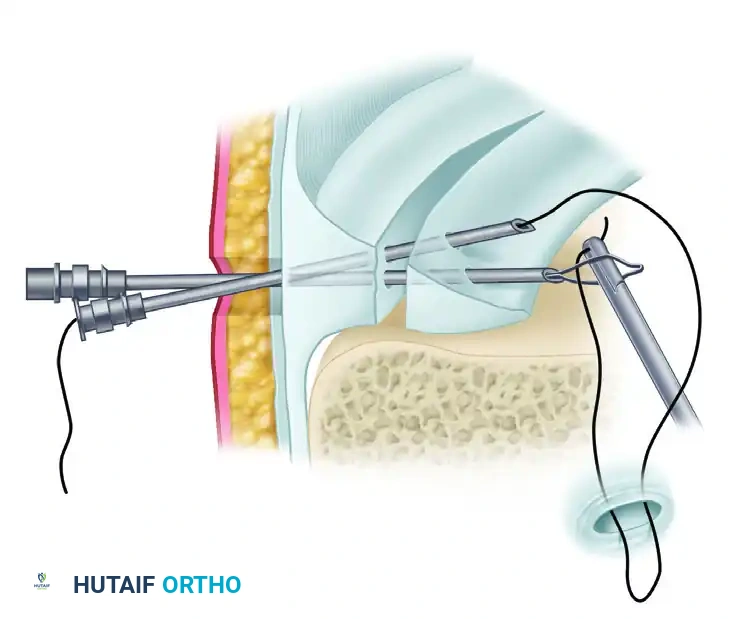
- Cannula Placement: A curved, double-lumen meniscal repair cannula is introduced through the contralateral portal.
- Suture Passage: Long, flexible needles loaded with non-absorbable or slowly absorbable suture (e.g., 2-0 FiberWire or PDS) are advanced through the cannula, across the meniscal tear, and out through the posterolateral capsule.
- Spacing: Sutures should be placed approximately 3 mm from the meniscal edge and spaced every 4 to 5 mm along the length of the tear. A stacked vertical mattress configuration (one suture on the femoral surface, one on the tibial surface) is highly recommended to prevent eversion of the meniscal edges.
💡 CLINICAL PEARL: When suturing posterolaterally, ensure the needles exit the capsule superior to the palpable biceps femoris tendon. A small posterolateral safety incision can be made down to the capsule to retrieve the needles under direct vision, further protecting the peroneal nerve.
The Outside-In Technique (Johnson Technique)
The outside-in technique is particularly useful for tears involving the anterior horn and the anterior portion of the middle third of the lateral meniscus, where the inside-out trajectory is technically difficult.
- Spinal Needle Placement: An 18-gauge spinal needle is passed from the outside of the knee, through the capsule, and across the meniscal tear into the joint space under direct arthroscopic visualization.
- Suture Shuttle: A permanent suture or a specialized wire cable loop is introduced through the spinal needle.
- Retrieval: The suture is retrieved through an anterior portal. A Mulberry knot can be tied in the end of the suture, which is then pulled back until the knot rests against the meniscal surface, or a standard mattress configuration can be created by passing a second needle.
FIGURE 51-25: Johnson technique. Permanent suture brought in through the anterior portal and placed into a wire cable loop to facilitate outside-in meniscal repair.
Managing Large Bucket-Handle Tears
Displaced peripheral bucket-handle tears of the lateral meniscus require a methodical approach to prevent the large fragment from displacing during suturing. A combination of inside-to-outside and outside-to-inside methods is frequently employed.
- Reduction: The bucket-handle fragment is anatomically reduced using a blunt probe.
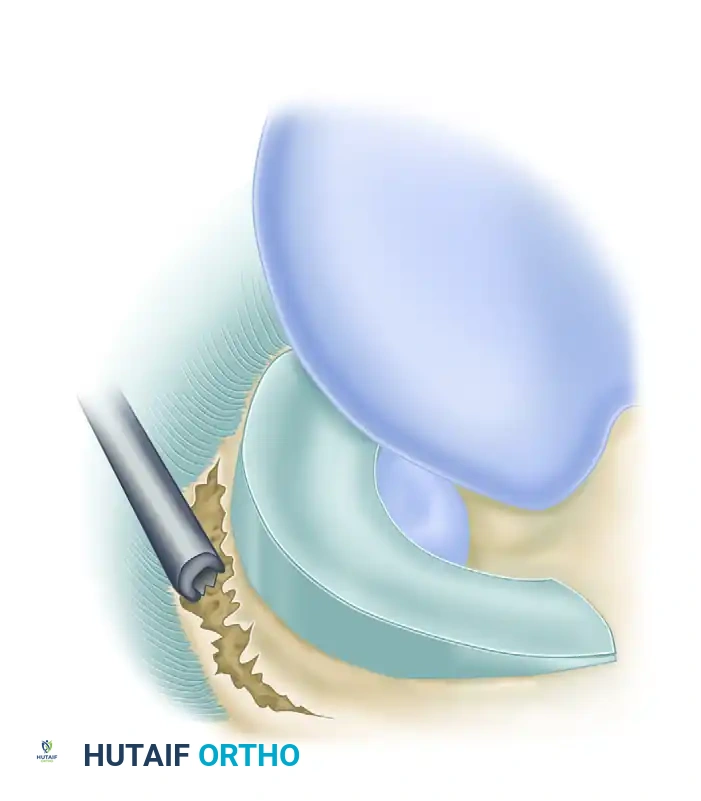
- The Stabilizing Suture: Place a single horizontal mattress suture, using a cannulated technique, into the midportion of the tear. This initial "stay suture" provides the necessary stability to the large bucket-handle fragment, preventing gross displacement when subsequent spinal needles or inside-out needles are passed through the posterior and anterior horn regions.
- Systematic Fixation: Once the midportion is stabilized, the surgeon can systematically work from posterior to anterior, placing stacked vertical mattress sutures to secure the fragment.
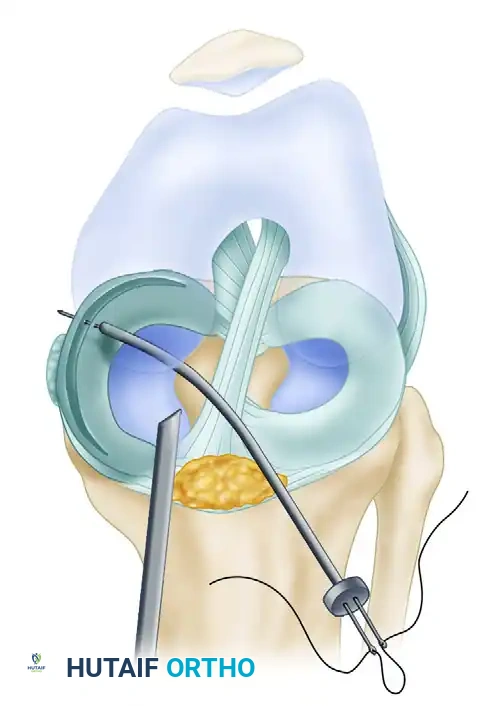
FIGURE 51-27: Suture placement in the midportion of a large bucket-handle tear using a curved cannula technique. This initial suture stabilizes the fragment for subsequent fixation.
ADVANCED REPAIR: RADIAL TEARS AND ROOT AVULSIONS
Historically considered irreparable, complete radial tears and meniscal root avulsions are now routinely repaired in active patients to prevent the catastrophic loss of meniscal hoop stresses.
Repair of Radial Tears
A complete radial tear that extends to the capsule completely disrupts the circumferential fibers of the meniscus, rendering it biomechanically equivalent to a total meniscectomy. In young patients with otherwise healthy meniscal tissue, these must be repaired.
- Debridement and Rasping: The edges of the radial tear are freshened, and the adjacent synovium is aggressively rasped.
- Suture Configuration: A longitudinal repair strategy is utilized. This typically consists of passing two longitudinal sutures on the superior surface of the meniscus and one on the inferior surface.
- Reapproximation: The first vertical mattress suture is placed to reapproximate the meniscal fragments. Subsequently, additional vertical mattress sutures are added to secure the posterior aspect of the capsule. At least two vertical mattress sutures are required, and often a third "stacked" vertical mattress suture is necessary to achieve a stable, watertight construct.
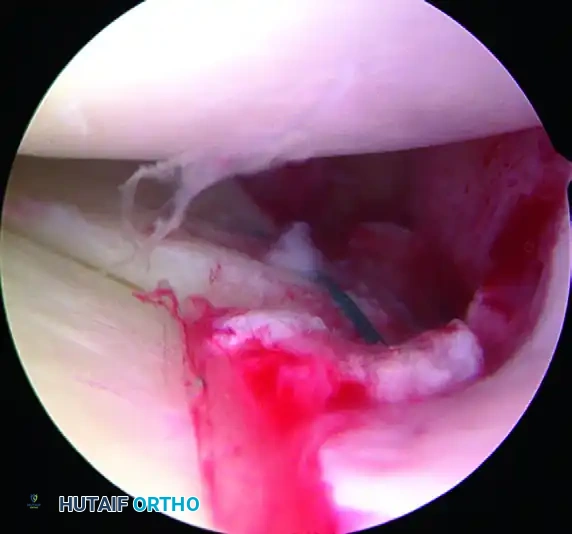
FIGURE 51-28: Arthroscopic view of the repair of a complete radial tear of the lateral meniscus. Note the meticulous reapproximation of the meniscal fragments using stacked vertical mattress sutures.
Repair of Lateral Meniscal Root Tears
Root tears of the lateral meniscus frequently occur in conjunction with Anterior Cruciate Ligament (ACL) tears. While some stable, partial root tears may heal in situ with synovial rasping (as described by Shelbourne et al.), unstable complete root tears of the posterior horn require robust surgical fixation.
Transtibial Pull-Out Technique:
1. Bed Preparation: The posterior bony bed at the anatomic footprint of the lateral meniscal root is decorticated and freshened using a curette or burr to promote a bleeding bone bed.
2. Tunnel Drilling: An ACL tibial guide is utilized to drill a tunnel from the anterolateral tibia to the base of the lateral root footprint.
3. Suture Passage: A suture shuttle device (e.g., Knee Scorpion or similar passing instrument) is used to pass heavy, non-absorbable mattress sutures (such as suture tape) through the detached meniscal root.
4. Fixation: The suture limbs are shuttled down through the tibial bone tunnel and tied over a cortical button or secured with a bio-tenodesis screw on the anterior tibia.
Suture Anchor Technique:
Alternatively, the repair may be accomplished using a 4.5 mm suture anchor. As described by Koenig and Ranawat, this anchor can be placed into the lateral root footprint through a high posteromedial portal.
Anatomical Note: While it may seem counterintuitive to use a posteromedial portal for a lateral structure, the lateral meniscal root inserts centrally, just anterior to the Posterior Cruciate Ligament (PCL). A high posteromedial portal provides an excellent, direct trajectory across the intercondylar notch to address the lateral root footprint.
KNOT TYING AND TENSIONING
The final, critical step in any meniscal suturing procedure is the tying of the knots. If approximation and stability have been achieved arthroscopically, the sutures are tied to each other over appropriate bridges of the posterolateral capsule.
🚨 PITFALL AVOIDANCE: Always tie the sutures with the knee in full extension.
Tying meniscal sutures while the knee is flexed will inadvertently plicate (tighten) the posterior capsule. When the patient subsequently attempts to straighten their leg postoperatively, the tethered capsule will prevent full extension, resulting in a permanent flexion contracture.
Ensure that the knots are tied directly over the capsule, avoiding the capture of subcutaneous fat or the iliotibial band, which can cause localized pain and friction syndromes.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol is paramount to the success of a lateral meniscal repair. The meniscal tissue heals slowly, relying on peripheral blood supply and synovial diffusion. The rehabilitation protocol must balance the protection of the fragile repair with the prevention of arthrofibrosis.
Phase 1: Maximum Protection (Weeks 0 to 6)
* Immobilization: Immediately postoperatively, the knee is immobilized in a commercial hinged knee brace locked in full extension.
* Weight-Bearing: The patient is restricted to partial weight-bearing (toe-touch to 20 lbs) on crutches for 4 to 6 weeks. The exact duration depends on the stability of the tear, the complexity of the repair, and the distance of the tear from the peripheral blood supply (red-white vs. white-white zones).
* Range of Motion (ROM): Passive ROM is typically limited to 0-90 degrees for the first 4 weeks to prevent excessive shear forces on the posterior horn, particularly during deep flexion.
Phase 2: Moderate Protection (Weeks 6 to 12)
* Weight-Bearing: Progression to full weight-bearing is permitted as tolerated.
* ROM: The brace is unlocked, and the patient progresses to full, unrestricted range of motion.
* Strengthening: Closed kinetic chain exercises (e.g., mini-squats, leg presses) are initiated, keeping flexion angles less than 90 degrees initially.
Phase 3: Return to Activity (Months 3 to 6)
* Advanced Strengthening: Focus shifts to proprioception, neuromuscular control, and sport-specific drills.
* Clearance: Return to pivoting, cutting, and high-impact sports is generally delayed until 5 to 6 months postoperatively, contingent upon the recovery of at least 90% quadriceps and hamstring strength compared to the contralateral limb.
CONCLUSION
Lateral meniscal suturing is a technically demanding but highly rewarding joint-preserving procedure. Mastery of this surgery requires a profound understanding of lateral compartment anatomy, particularly the course of the common peroneal nerve and the popliteus hiatus. By judiciously employing inside-out, outside-in, and hybrid suturing techniques—and by adhering strictly to biomechanical principles during knot tying and postoperative rehabilitation—the orthopedic surgeon can successfully restore meniscal function, thereby safeguarding the long-term health of the knee joint.
You Might Also Like