Ulnar Styloid Fractures: Comprehensive Guide to Anatomy, Biomechanics & Surgical Management for DRUJ Stability
Key Takeaway
Ulnar styloid fractures are clinically significant due to their intimate relationship with the TFCC and paramount role in Distal Radioulnar Joint (DRUJ) stability. Surgical management is indicated primarily when DRUJ instability persists after associated distal radius fracture fixation, or with large, displaced styloid fragments. This addresses the risk of chronic pain and functional impairment.
Understand & Treat Styloid Fractures Ulnar: Expert Surgical Guide
Introduction & Epidemiology
Ulnar styloid fractures, while often appearing as an ancillary injury in the context of a distal radius fracture (DRF), represent a critical determinant of long-term wrist function, particularly regarding distal radioulnar joint (DRUJ) stability. The incidence of ulnar styloid fractures associated with DRF ranges significantly in the literature, commonly cited between 50% and 60%, underscoring their prevalence. Isolated ulnar styloid fractures are less common but do occur, typically from direct trauma or avulsion mechanisms.
The primary clinical significance of an ulnar styloid fracture lies in its intimate relationship with the triangular fibrocartilage complex (TFCC). The TFCC, the primary stabilizer of the DRUJ, inserts prominently onto the fovea and base of the ulnar styloid. Consequently, displacement or non-union of the styloid fragment can directly compromise the integrity and function of the TFCC, leading to persistent DRUJ instability, pain, clicking, and ultimately, post-traumatic degenerative changes. Despite their prevalence, ulnar styloid fractures are sometimes overlooked or considered benign, potentially contributing to suboptimal outcomes following DRF fixation if DRUJ instability is not adequately addressed. This guide aims to delineate a comprehensive understanding of ulnar styloid fractures and their surgical management, focusing on their critical biomechanical role and the imperative for meticulous operative intervention when indicated.
Surgical Anatomy & Biomechanics
Successful management of ulnar styloid fractures necessitates a thorough understanding of the regional anatomy and biomechanics of the DRUJ and TFCC.
Surgical Anatomy
- Ulnar Styloid: The most distal projection of the ulnar head, varying in length and prominence among individuals. It serves as a crucial anchor point for critical soft tissue structures.
-
Triangular Fibrocartilage Complex (TFCC):
This complex structure is the primary stabilizer of the DRUJ and a major load bearer. It consists of the articular disc (meniscus homolog), the dorsal and volar radioulnar ligaments, the ulnar collateral ligament, and the sheath of the extensor carpi ulnaris (ECU) tendon.
- Peripheral Attachment: The critical insertion points for the TFCC are the fovea (a depression on the ulnar head) and the base of the ulnar styloid. The strong foveal fibers primarily originate from the dorsal and volar radioulnar ligaments, while the superficial fibers insert along the styloid. Fractures at the base of the styloid, or large fragments, often involve the primary attachments of these crucial ligaments.
- Articular Disc: The central, avascular portion that articulates with the lunate and triquetrum, and bears axial load. Its peripheral vascularized portion is capable of healing.
- Distal Radioulnar Joint (DRUJ): A uniaxial pivot joint allowing pronation and supination. Its stability is conferred by bony congruity (sigmoid notch of the radius, ulnar head) and, predominantly, by the TFCC.
-
Neurovascular Structures:
- Ulnar Nerve: The dorsal cutaneous branch of the ulnar nerve is superficial and vulnerable to injury during ulnar-sided approaches. The main ulnar nerve and artery run volar and more proximally, protected by the flexor carpi ulnaris (FCU) tendon.
- Extensor Carpi Ulnaris (ECU): Lies in the 6th dorsal compartment, just radial to the ulnar styloid. Its sheath forms part of the TFCC.
- Flexor Carpi Ulnaris (FCU): Lies volar and ulnar, inserting into the pisiform, hamate, and fifth metacarpal.
Biomechanics
- DRUJ Stability: The TFCC acts as a sling, maintaining the relationship between the distal radius and ulna throughout pronation and supination. It resists axial, translational, and rotational forces. Intact peripheral TFCC fibers, particularly the dorsal and volar radioulnar ligaments inserting at the fovea and styloid base, are essential.
- Load Transmission: The TFCC transmits approximately 20% of the axial load across the wrist.
-
Styloid Fracture Impact:
- Large Fragments: Fractures involving a significant portion (>2-3mm displacement or >25% of the styloid base) are highly problematic because they often avulse the strong peripheral TFCC attachments. This directly compromises DRUJ stability.
- Small, Apex Fragments: Fractures of the styloid tip typically do not directly involve the main foveal or radioulnar ligament attachments and are less likely to cause DRUJ instability.
- Proximal vs. Distal: Proximal styloid fractures, especially those at the base, carry a higher risk of DRUJ instability due to disruption of the foveal and stout superficial TFCC insertions.
- DRUJ Instability: Clinical assessment of DRUJ stability following DRF reduction is paramount. If the DRUJ remains unstable, it mandates a thorough evaluation of the TFCC and ulnar styloid. A "positive piano key sign" or excessive translation after reduction indicates instability.
Indications & Contraindications
The decision to operatively treat an ulnar styloid fracture hinges primarily on its impact on DRUJ stability, the size and displacement of the fragment, and the associated TFCC injury. This decision is often made in conjunction with the management of an associated distal radius fracture.
Operative Indications
- DRUJ Instability: This is the most critical indication. If, after anatomical reduction and stable fixation of an associated distal radius fracture, the DRUJ remains unstable upon provocative testing (e.g., ballotment, piano key test), surgical stabilization of the ulnar styloid or direct TFCC repair is indicated. Arthroscopic assessment provides invaluable direct visualization of TFCC integrity.
-
Large, Displaced Ulnar Styloid Fragments:
- Displacement >2-3 mm: Significantly displaced fragments disrupt the TFCC's mechanical integrity.
- Involvement of >25-30% of the Styloid Base: Fragments comprising a substantial portion of the styloid's base are likely to carry significant TFCC attachments, leading to instability if unaddressed.
- Avulsion of TFCC from Styloid: As identified arthroscopically, if the articular disc is lax and the TFCC's peripheral fibers are primarily attached to the displaced styloid fragment.
- Associated with TFCC Tears: When arthroscopy reveals a peripheral TFCC tear (especially foveal or styloid avulsion) in conjunction with an ulnar styloid fracture, repair is indicated.
- Non-union with Symptoms: A painful, symptomatic non-union of the ulnar styloid, particularly if associated with chronic DRUJ instability.
Non-Operative Indications
- Stable DRUJ: The most important factor. If the DRUJ is stable after DRF reduction (or in isolated styloid fractures), even with a displaced styloid, non-operative management is typically preferred.
- Small, Non-Displaced Styloid Fractures: Fractures of the styloid tip or very small fragments (<2 mm displacement, <25% involvement of the styloid base) are often treated non-operatively as they typically do not compromise DRUJ stability.
- Asymptomatic Non-union: If a styloid non-union is discovered incidentally and the patient is asymptomatic with a stable DRUJ, no intervention is required.
- Patient Comorbidities: High surgical risk due to significant medical comorbidities precluding elective surgery.
Contraindications
- Severe Comminution: Extensive comminution of the ulnar styloid that precludes stable anatomical reduction and fixation. In such cases, TFCC repair might be attempted, or the fragments might be excised if they are too small to reconstruct, with consideration for DRUJ stabilization procedures if instability persists.
- Active Infection: Absolute contraindication to elective hardware placement.
- Poor Soft Tissue Envelope: Compromised skin or soft tissue over the fracture site.
- Non-compliant Patient: Inability or unwillingness to adhere to post-operative rehabilitation protocols.
Table: Operative vs. Non-Operative Indications for Ulnar Styloid Fractures
| Feature | Operative Management | Non-Operative Management |
|---|---|---|
| DRUJ Stability | Unstable (after DRF reduction) | Stable (after DRF reduction, or isolated fracture) |
| Fragment Size | Large (>25-30% of styloid base) | Small (<25% of styloid base, styloid tip) |
| Fragment Displacement | >2-3 mm | <2 mm, non-displaced |
| TFCC Status | Lax articular disc/peripheral TFCC avulsion (arthroscopic) | Intact/stable TFCC |
| Symptoms | Symptomatic non-union/DRUJ instability | Asymptomatic non-union/DRUJ stability |
| Associated DRF | Yes, with persistent DRUJ instability | Yes, with stable DRUJ after DRF fixation |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial to optimize surgical outcomes for ulnar styloid fractures, especially when associated with distal radius fractures.
Pre-Operative Planning
-
Clinical Assessment:
- History: Mechanism of injury, hand dominance, functional demands, baseline medical comorbidities.
- Physical Examination: Thorough neurovascular assessment. Careful evaluation of DRUJ stability via provocative testing (e.g., comparing pronation/supination to contralateral wrist, piano key sign, ballottement test for anterior/posterior translation of the ulna relative to the radius). This assessment is critical both before and after provisional reduction of any associated DRF.
-
Imaging Studies:
- Plain Radiographs: AP, lateral, and oblique views of the wrist are standard. These help determine the size, displacement, and comminution of the styloid fragment, as well as the extent of any associated distal radius fracture.
- Computed Tomography (CT) Scan: Highly recommended for complex DRF with styloid involvement, particularly to assess DRUJ congruity, fragment orientation, and to identify small, potentially overlooked fragments. Useful for surgical planning, especially for screw placement.
- Magnetic Resonance Imaging (MRI): While not routinely required for acute fractures, MRI can provide detailed information about TFCC integrity and morphology, which may influence decision-making for delayed presentations or persistent symptoms.
-
Fixation Strategy:
- Based on imaging and clinical assessment, determine the preferred fixation method: tension band wiring, K-wires, or headless cannulated screws. headless cannulated screws are often preferred for larger, amenable fragments due to their compressive properties and low profile.
- Consider hardware availability and specific screw sizes (e.g., 2.0-2.4 mm).
- Plan for concurrent DRF fixation if applicable, as the DRF must be anatomically reduced and stably fixed before addressing the styloid and DRUJ stability.
- Anesthesia Consultation: Standard pre-operative assessment for regional (e.g., axillary block) or general anesthesia.
- Informed Consent: Discuss potential complications including non-union, malunion, DRUJ instability, hardware irritation/failure, infection, nerve injury (dorsal cutaneous branch of ulnar nerve), CRPS, and the need for possible hardware removal. Emphasize the potential for persistent DRUJ pain or instability despite optimal surgical intervention.
Patient Positioning
- Position: Supine on the operating table, with the affected arm on a radiolucent hand table.
- Tourniquet: A pneumatic tourniquet is applied to the upper arm to provide a bloodless field, typically inflated to 250-300 mmHg.
- Arm Holder: A dedicated arm holder or traction tower may be used if wrist arthroscopy or ligamentotaxis for DRF reduction is planned.
- Fluoroscopy: The C-arm fluoroscope should be draped and positioned to allow for clear AP and lateral views of the wrist without repositioning the patient or the arm. This is crucial for confirming DRF reduction, guidewire placement, and final screw position.
- Draping: Standard sterile draping of the arm up to the tourniquet, ensuring adequate exposure for both arthroscopic portals and the open surgical incision on the ulnar side of the wrist. A waterproof stockinette and adhesive drape are often used.
Detailed Surgical Approach / Technique
The surgical management of ulnar styloid fractures is often undertaken in conjunction with the fixation of an associated distal radius fracture. The priority is to achieve stable anatomical reduction of the distal radius first, as this often indirectly improves DRUJ alignment and allows for a more accurate assessment of residual DRUJ instability.
1. Arthroscopic Assessment and DRF Fixation
- Distal Radius Fixation First: Proceed with the planned open reduction and internal fixation (ORIF) of the distal radius fracture. Achieve anatomical reduction and stable fixation, typically with a volar locking plate.
-
Arthroscopic Evaluation (if indicated):
- With the DRF stably reduced, insert the arthroscope in the dorsal 3/4 portal (between the 3rd and 4th dorsal compartments) and the probe in the 6R portal (radial to the ECU tendon). This allows for direct visualization of the TFCC and DRUJ articulation.
- "Palpate the tension of the articular disc." Use the probe to stress the TFCC, assessing its attachment and integrity.
- "Good tension indicates that the majority of the peripheral TFCC fibers are intact or still attached to the proximal ulna." In this scenario, if the DRUJ is stable, direct styloid fixation might not be necessary.
- "A peripheral tear of the articular disc is repaired arthroscopically when detected." If a peripheral TFCC tear is identified and contributing to instability, primary arthroscopic repair may be performed, often with suture anchors.
-
"Stabilization of a large ulnar styloid fragment is considered when the articular disc is lax by palpation and no peripheral TFCC is identified (TECH FIG 5)."
This specific finding strongly suggests that the TFCC's critical attachments have avulsed with the styloid fragment. The image
could be relevant here to illustrate the arthroscopic view of a lax TFCC or a styloid avulsion. - "In this instance, the majority of the fibers of the TFCC are attached to the displaced ulnar styloid fragment." This arthroscopic finding mandates open reduction and internal fixation of the ulnar styloid to re-establish TFCC tension and DRUJ stability.
2. Open Surgical Approach to the Ulnar Styloid
-
Incision Planning:
- "Make a small incision between the extensor carpi ulnaris and the flexor carpi ulnaris tendons and identify the fracture site." This implies a longitudinal incision on the direct ulnar aspect of the wrist. It's crucial to clarify this anatomical interval. A more precise description for a direct ulnar approach involves a longitudinal incision centered over the ulnar styloid, typically between 2 to 4 cm in length, depending on fragment size and required exposure.
- Landmarks: The incision should be positioned radial to the palpable tendon of the flexor carpi ulnaris (FCU) and ulnar to the extensor carpi ulnaris (ECU) tendon (which lies within the 6th dorsal compartment). This provides direct access to the styloid while avoiding major tendons and neurovascular bundles.
-
Dissection:
- Carefully incise the skin and subcutaneous tissues.
- Protect the dorsal cutaneous branch of the ulnar nerve: This sensory nerve is highly variable in its course but frequently crosses the operative field dorsally. It must be identified, protected, and retracted.
- Incise the superficial fascia longitudinally. Identify the fracture site by palpation and direct visualization. The ulnar styloid fragment often retracts distally and radially due to the pull of the TFCC and ulnocarpal ligaments.
-
Fragment Retrieval and Mobilization:
- "Retrieve the distal fragment, which often displaces in a distal and radial direction." Use fine surgical instruments (e.g., Adson forceps, small rake retractors) to gently retrieve and expose the fragment.
- "Mobilize the styloid fragment using a no. 15 blade, taking care to protect the TFCC insertion." Carefully debride any interposed soft tissues or hematoma from the fracture site on both the styloid fragment and the ulnar metaphysis. Ensure the TFCC attachments to the fragment remain as intact as possible; do not strip them further. This mobilization prepares the surfaces for anatomical reduction and allows for controlled manipulation.
3. Reduction and Provisional Fixation
-
Anatomical Reduction:
- "Reduce the fragment anatomically, under direct visual- ization..." Using fine pointed reduction clamps or small bone hooks, meticulously reduce the styloid fragment to its anatomical position. Direct visualization is critical to ensure perfect alignment, which is essential for restoring DRUJ stability and TFCC function.
- During reduction, ensure that there is no rotational malalignment of the fragment. The fragment should sit flush with the ulnar metaphysis.
-
Provisional Stability:
-
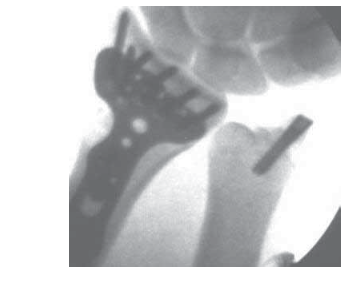
"...and insert a guidewire in a retrograde manner for provisional stability."
Once anatomical reduction is achieved, maintain it with temporary reduction clamps. Insert a 1.1 mm or 1.25 mm (0.045" or 0.054") guidewire percutaneously or through a small stab incision, directed from the tip of the styloid fragment proximally across the fracture line into the ulnar metaphysis. Ensure the guidewire trajectory provides optimal purchase in the ulnar cancellous bone. The guidewire should be positioned to allow for definitive fixation with a screw or tension band. Fluoroscopic images
could illustrate guidewire placement and initial reduction.
-
"...and insert a guidewire in a retrograde manner for provisional stability."
Once anatomical reduction is achieved, maintain it with temporary reduction clamps. Insert a 1.1 mm or 1.25 mm (0.045" or 0.054") guidewire percutaneously or through a small stab incision, directed from the tip of the styloid fragment proximally across the fracture line into the ulnar metaphysis. Ensure the guidewire trajectory provides optimal purchase in the ulnar cancellous bone. The guidewire should be positioned to allow for definitive fixation with a screw or tension band. Fluoroscopic images
4. Definitive Fixation
-
Choice of Fixation:
The primary goal is stable fixation allowing early range of motion.
- "Stabilize the ulnar styloid fragment using either a tension band technique (with wire and two K-wires) or, preferably, using a micro headless cannulated screw."
- Considerations: Fragment size, bone quality, surgeon preference, and the need for compression. For larger, single fragments, a headless compression screw is generally preferred.
-
Micro Headless Cannulated Screw Technique (Preferred):
- Guidewire Placement: Confirm the provisional guidewire's position on fluoroscopy (AP and lateral views) to ensure accurate reduction and optimal screw trajectory. The guidewire should be centered within the fragment and extending well into the ulnar metaphysis.
- Measurement: Use a depth gauge over the guidewire to determine the appropriate screw length.
- Drilling/Tapping: Pre-drill (if recommended by the screw system) and tap (if self-tapping screws are not used) over the guidewire according to the manufacturer's specifications.
- Screw Insertion: "Place the cannulated headless screw over the guidewire and verify fracture reduction with fluoroscopy." Carefully advance the headless cannulated screw over the guidewire. As the screw engages the bone, it will create interfragmentary compression, drawing the fragment tightly to the ulna. The headless design allows for subchondral placement without hardware prominence.
-
Final Fluoroscopy:
Verify final screw position and fracture reduction in multiple planes using fluoroscopy. Ensure the screw does not violate the DRUJ articular surface or impinge on adjacent tendons. The image
orcan illustrate the final screw placement.
-
Tension Band Technique:
- K-wire Placement: Two small K-wires (e.g., 0.035" or 0.045") are inserted parallel to each other from the tip of the styloid across the fracture into the ulnar metaphysis. Ensure they gain good purchase.
- Wire Loop: A figure-of-eight tension band wire (e.g., 20 or 22 gauge) is then passed around the protruding K-wire ends and looped around a proximally drilled transverse hole in the ulnar metaphysis or around a small Kirschner wire placed transversely.
- Tightening: The wire is progressively tightened, creating compression across the fracture site. The K-wires are then bent and cut.
- Advantages: Good compression, effective for comminuted fragments or poor bone quality.
- Disadvantages: More prominent hardware, higher potential for soft tissue irritation, may require a second surgery for hardware removal.
5. Final Assessment and Closure
- DRUJ Stability Check: After definitive styloid fixation, perform a final, rigorous assessment of DRUJ stability by pronating and supinating the forearm and applying stress. The DRUJ should now be stable.
- Final Arthroscopy (completion of seed content): "Insert the arthroscope into the 3/4 portal and the probe into" the DRUJ to visually confirm stable DRUJ kinematics and assess any residual TFCC tears or incarceration. This ensures that the styloid fixation has effectively restored TFCC tension and DRUJ congruence.
-
Wound Closure:
- Irrigate the wound thoroughly.
- Close the subcutaneous tissues and skin in layers using absorbable sutures for subcutaneous closure and non-absorbable sutures or staples for skin.
- Apply a sterile dressing.
- Apply a sugar tong splint or long arm cast to provide immediate post-operative protection, with the forearm in neutral rotation.
Complications & Management
Despite meticulous surgical technique, complications can arise following ulnar styloid fracture fixation. Prompt recognition and appropriate management are crucial for optimizing patient outcomes.
Common Complications and Management Strategies
| Complication | Incidence | Management Strategy |
|---|---|---|
| DRUJ Instability / Malunion | 5-20% (can be higher with delayed diagnosis) |
Prevention:
Meticulous anatomical reduction and stable fixation of styloid and DRF. Intraoperative DRUJ stability check.
Acute/Early: Revision fixation of styloid/DRF, TFCC repair (suture anchors if avulsion from fovea). Chronic: TFCC reconstruction, Sauvé-Kapandji procedure, Darrach procedure, hemiresection arthroplasty, or prosthetic DRUJ replacement. |
| Non-union | 5-15% (higher in large, displaced fragments) |
Prevention:
Rigid fixation, anatomical reduction, adequate blood supply.
Symptomatic: Bone grafting (autogenous or allograft), revision internal fixation (screw or tension band). If small, may consider excision. Asymptomatic: Observe. |
| Hardware Irritation / Failure | 10-25% (especially with tension bands/K-wires) |
Symptoms:
Pain, clicking, reduced range of motion, palpable prominence.
Management: Symptomatic hardware removal after fracture healing (typically 3-6 months). If failure prior to union, consider revision fixation. |
| Infection | <2% (superficial), <1% (deep) |
Prevention:
Strict aseptic technique, prophylactic antibiotics.
Superficial: Oral antibiotics, wound care. Deep: Surgical debridement, intravenous antibiotics, hardware removal (if stable union or unstable with planned revision). |
| Neurovascular Injury | <1% (dorsal cutaneous ulnar nerve most common) |
Prevention:
Careful dissection, identification, and protection of the dorsal cutaneous branch of the ulnar nerve.
Management: Neuropathic pain management, potential nerve repair/grafting if transected, neurolysis for impingement. |
| Complex Regional Pain Syndrome (CRPS) | 1-5% (any wrist trauma/surgery) |
Prevention:
Gentle tissue handling, adequate pain control, early mobilization.
Management: Multidisciplinary approach: regional nerve blocks, physical therapy, occupational therapy, pain medication, psychological support. Early recognition is key. |
| Stiffness / Loss of Motion | Variable, depending on severity of injury |
Prevention:
Early, controlled post-operative rehabilitation.
Management: Intensive physical/occupational therapy, dynamic splinting, manipulation under anesthesia. Severe cases may require surgical release (arthrolysis). |
| Ulnar Impaction Syndrome | Long-term complication if DRUJ malunion |
Prevention:
Restore appropriate ulnar variance and DRUJ alignment.
Management: Ulnar shortening osteotomy, wafer resection, Darrach procedure. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is integral to achieving optimal functional outcomes following ulnar styloid fracture fixation. The protocol is tailored to the stability of the fixation, the quality of bone, and the presence of associated injuries (e.g., DRF, TFCC repair).
1. Immobilization (Initial Phase: Weeks 0-4/6)
- Initial Splinting: Immediately post-operatively, a well-padded sugar tong splint or long arm cast is applied, typically with the forearm in neutral rotation to minimize stress on the DRUJ.
- Duration: Immobilization usually lasts for 4 to 6 weeks, depending on the fracture stability and surgeon preference.
- Goals: Protect the healing fracture and TFCC repair, minimize swelling and pain.
- Patient Education: Instruct patients on elevation, icing, and gentle active range of motion (AROM) of uninvolved joints (fingers, thumb, elbow, shoulder) to prevent stiffness.
2. Early Motion (Transition Phase: Weeks 4/6 - 8/12)
- Splint Removal: Once clinical and radiographic signs of early healing are evident (typically around 4-6 weeks), the splint is discontinued.
-
Initiate Controlled Range of Motion:
- Passive Range of Motion (PROM): Gentle, pain-free PROM of the wrist (flexion/extension, radial/ulnar deviation) is initiated.
- Active Range of Motion (AROM): Progress to active wrist motion.
- Forearm Rotation: Controlled, pain-free pronation and supination are introduced carefully, especially if DRUJ stability was a primary concern. Initially, limit end-range rotation to protect the healing TFCC and styloid.
- Soft Tissue Mobilization: Gentle scar massage and desensitization around the incision site.
- Modalities: Therapeutic modalities such as ultrasound, heat, or cold therapy may be used to manage pain and swelling.
- Goals: Restore initial wrist and forearm motion, reduce stiffness, and prevent adhesions.
3. Strengthening (Progressive Phase: Weeks 8/12 - 16+)
-
Gradual Strengthening:
Once good range of motion is achieved and pain is well controlled, progressive strengthening exercises are introduced.
- Isometric Exercises: Initial exercises for wrist flexors, extensors, pronators, and supinators.
- Isotonic Exercises: Use light weights, elastic bands, or therapeutic putty for grip strengthening.
- Functional Exercises: Incorporate activities that mimic daily tasks.
- DRUJ Strengthening: Specific exercises to strengthen the musculature around the DRUJ (e.g., pronator quadratus, ECU).
- Proprioception Training: Introduce activities to improve joint position sense and control.
- Goals: Restore full strength, endurance, and functional capacity of the wrist and forearm.
4. Return to Activity (Advanced Phase: Weeks 16+)
- Sport-Specific/Work-Specific Training: For athletes or individuals with demanding occupations, progressive, sport- or work-specific drills are incorporated.
- Impact Activities: High-impact or heavy lifting activities are typically restricted until at least 4-6 months post-operatively, depending on radiographic union and clinical stability.
- Full Return: Full return to unrestricted activities is guided by clinical assessment of pain, strength, and range of motion, often requiring 4 to 6 months or longer.
- Patient Education: Emphasize the importance of continued home exercise programs and activity modification as needed.
Throughout the rehabilitation process, close collaboration between the surgeon, physical therapist, and occupational therapist is essential. Regular follow-up appointments with radiographs are crucial to monitor fracture healing and assess DRUJ stability. Any signs of persistent pain, instability, or delayed union warrant re-evaluation and potential modification of the rehabilitation plan or further intervention.
Summary of Key Literature / Guidelines
The management of ulnar styloid fractures has evolved significantly, particularly with advancements in arthroscopic techniques and internal fixation. A consensus has emerged regarding their critical role in DRUJ stability, especially when associated with distal radius fractures.
- Association with DRUJ Instability: Numerous studies consistently highlight the strong correlation between displaced ulnar styloid fractures and DRUJ instability following distal radius fracture fixation. The integrity of the TFCC, particularly its foveal and styloid attachments, is paramount. Clinical studies have shown that untreated displaced ulnar styloid fractures in the context of DRF are associated with increased rates of DRUJ instability, pain, and poorer functional outcomes (e.g., Palmer et al., Whipple et al.).
- Size and Displacement Criteria: While no universally accepted, absolute threshold exists for operative fixation based solely on fragment size, a general consensus suggests that fragments larger than 2-3 mm displacement or involving more than 25-30% of the styloid base are more likely to compromise DRUJ stability and warrant consideration for fixation. Smaller, non-displaced fractures, particularly those of the styloid tip, typically heal without intervention and do not destabilize the DRUJ.
- Arthroscopic Assessment: The value of wrist arthroscopy in evaluating TFCC integrity and DRUJ stability post-DRF fixation is increasingly recognized. Direct visualization allows for precise diagnosis of TFCC avulsions from the styloid or fovea, which is a key indicator for styloid fixation or direct TFCC repair (Geissler et al.). The seed content directly reflects this contemporary practice, emphasizing arthroscopic palpation of disc tension.
-
Fixation Methods:
- Tension Band Wiring: A time-tested technique, particularly effective for smaller, avulsion-type fractures or those with comminution where screw fixation is challenging. However, hardware prominence and irritation often lead to subsequent removal.
- Headless Compression Screws: Increasingly favored for larger, amenable fragments due to their ability to provide interfragmentary compression, low profile, and reduced need for hardware removal. Studies comparing outcomes often favor screws for larger fragments due to superior compression and patient comfort (e.g., Kim et al.).
- Suture Anchors: Can be considered for pure TFCC avulsions from the styloid (without a significant bony fragment) or in conjunction with styloid fixation.
- Timing of Intervention: While some isolated, asymptomatic styloid non-unions can be observed, intervention for symptomatic non-union or chronic DRUJ instability is often necessary. Early, acute fixation of unstable styloid fractures during the primary DRF surgery is generally preferred to prevent chronic instability and its sequelae.
- Long-Term Outcomes: Untreated DRUJ instability arising from ulnar styloid fractures can lead to chronic pain, loss of forearm rotation, impaired grip strength, and ultimately, post-traumatic DRUJ arthrosis. Successful anatomical reduction and stable fixation of the ulnar styloid, particularly when restoring TFCC tension, significantly improve long-term DRUJ stability and overall wrist function.
- Guidelines: While specific society guidelines dedicated solely to ulnar styloid fractures are limited, major orthopedic societies (e.g., AAOS, AANA) emphasize the comprehensive evaluation and management of DRUJ stability when treating distal radius fractures. The decision-making process should integrate radiographic findings, intraoperative DRUJ stability assessment (with or without arthroscopy), and patient-specific factors.
In conclusion, the ulnar styloid fracture, particularly when displaced and involving the TFCC attachment, is not a benign injury. Its meticulous evaluation and, when indicated, operative stabilization are paramount to restoring DRUJ stability, preserving TFCC function, and achieving optimal, long-lasting outcomes for the injured wrist.
You Might Also Like
