Benefits of Exercise: Orthopedic Health for a Stronger You
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Benefits of Exercise: Orthopedic Health for a Stronger You. The benefits of exercise for orthopedic health include building strong muscles and bones, improving joint stability and range of motion, and enhancing posture. Regular physical activity also aids in weight management, reducing joint stress, and promoting joint lubrication. These actions collectively lead to a stronger musculoskeletal system and better overall well-being.
The Indispensable Role of Structured Exercise in Orthopedic Practice: Prevention, Non-Operative Management, and Perioperative Optimization
Introduction & Epidemiology
Exercise, far exceeding its general health benefits, stands as a cornerstone therapeutic modality within orthopedic surgery. Its judicious application spans the entire spectrum of patient care, from primary prevention of musculoskeletal pathologies to pre-operative optimization and intensive post-operative rehabilitation. The epidemiological burden of musculoskeletal conditions is staggering; disorders such as osteoarthritis (OA), chronic low back pain, rotator cuff pathologies, and ligamentous instabilities contribute significantly to global disability, healthcare costs, and diminished quality of life. Sedentary lifestyles and physical inactivity are recognized modifiable risk factors that exacerbate the incidence and severity of these conditions, accelerating degenerative processes and diminishing physiological reserves.
From an orthopedic perspective, structured exercise influences tissue homeostasis and biomechanical function at multiple levels. It acts as a powerful stimulus for bone remodeling, enhancing bone mineral density and reducing osteoporotic fracture risk. It modulates articular cartilage health by promoting nutrient diffusion and adapting to physiological loads, potentially slowing the progression of early OA. Exercise strengthens the musculotendinous units, improving joint stability, distributing forces more effectively across joints, and enhancing proprioception and neuromuscular control. Furthermore, it plays a critical role in weight management, thereby reducing mechanical stress on load-bearing joints.
This academic review delves into the mechanisms, indications, contraindications, and practical implementation of exercise within the context of orthopedic surgical practice, emphasizing its role in optimizing patient outcomes across various orthopedic pathologies.
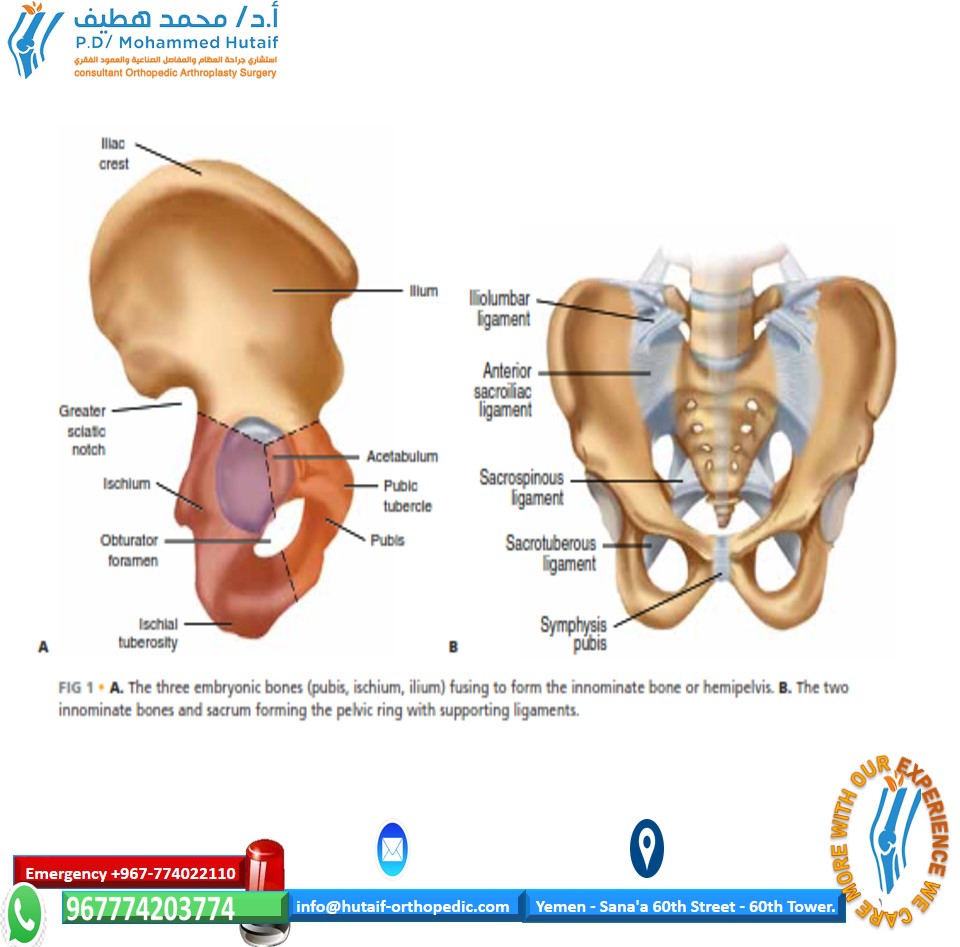
Surgical Anatomy & Biomechanics
Understanding the surgical anatomy and biomechanics influenced by exercise is fundamental to appreciating its therapeutic value in orthopedics. The musculoskeletal system operates as an integrated kinetic chain, where regional deficits can manifest as distal pathologies.
Musculoskeletal Unit and Joint Stability
- Muscles and Tendons: Exercise, particularly resistance training, induces muscle hypertrophy, increases muscle fiber cross-sectional area, and enhances motor unit recruitment and synchronization. This improves muscle strength, power, and endurance. Tendons adapt to mechanical loading by increasing collagen synthesis and cross-linking, enhancing tensile strength and stiffness, thereby improving their capacity to transmit forces and resist injury. A robust musculature provides dynamic stability to joints, attenuating excessive motion and protecting ligaments and capsules from undue stress.
- Ligaments and Joint Capsules: While ligaments and capsules primarily provide static stability, surrounding musculature significantly influences their functional integrity. Strong, well-coordinated muscles can reduce the strain on ligaments during dynamic activities, potentially mitigating the risk of sprains or tears. Post-injury or post-surgery, controlled loading through exercise promotes collagen alignment and maturation, enhancing the mechanical properties of healing ligamentous tissues, although their intrinsic healing capacity often necessitates surgical intervention for complete ruptures.
- Articular Cartilage: Articular cartilage is aneural and avascular, relying on cyclic compression and decompression during weight-bearing activities for nutrient exchange and waste removal. Moderate, physiological loading stimulates chondrocyte activity, promoting matrix synthesis and maintaining cartilage health. Conversely, prolonged immobilization or excessive, repetitive high-impact loading can be detrimental, leading to cartilage degradation. Exercise programs designed to maintain joint congruity and reduce aberrant loading patterns can play a protective role, particularly in early-stage osteoarthritis.
- Bone: Bone is a dynamic tissue that remodels in response to mechanical stress, governed by Wolff's Law. Weight-bearing and resistance exercises stimulate osteoblast activity, increasing bone mineral density (BMD) and improving bone architecture. This is crucial for preventing osteoporosis and maintaining skeletal integrity, thereby reducing the risk of fragility fractures. In fracture healing, controlled, progressive weight-bearing and muscle activation can optimize callus formation and bone remodeling.
Biomechanical Principles in Exercise
- Load Management: Optimal exercise involves carefully prescribed loads that stimulate adaptation without causing injury. Understanding tissue tolerance thresholds is paramount. For instance, gradual increases in load and volume are essential in tendinopathy rehabilitation to promote collagen remodeling without exacerbating pain or microtrauma.
- Kinetic Chain Integration: The body functions as an interconnected system. Core stability, hip strength, and ankle mobility, for example, profoundly influence knee and shoulder mechanics. Exercise programs must address the entire kinetic chain to optimize movement patterns, distribute forces efficiently, and prevent compensatory movements that could lead to injury or surgical failure.
- Neuromuscular Control and Proprioception: Exercise, particularly balance and agility training, enhances proprioception (the sense of joint position and movement) and neuromuscular control (the coordinated action of muscles to produce desired movements). Improved proprioception is vital for dynamic joint stability, fall prevention, and successful return to activity post-injury or surgery, particularly following ligamentous reconstructions or joint replacements.
Indications & Contraindications
The application of exercise in orthopedic practice requires a nuanced understanding of its indications and contraindications, distinguishing between its role in non-operative management and its integration into perioperative pathways.
Indications for Exercise (Non-Operative Management & Perioperative Optimization)
Primary Non-Operative Management:
- Early to Moderate Osteoarthritis (All Joints): Structured exercise programs (aerobic, resistance, flexibility, balance) improve pain, joint function, range of motion, and muscle strength. Evidence supports its efficacy in delaying or even obviating the need for joint arthroplasty in many patients.
-
Chronic Musculoskeletal Pain:
- Chronic Low Back Pain (CLBP): Core strengthening, motor control exercises, and aerobic conditioning are first-line treatments, often superior to passive modalities.
- Cervicogenic Pain: Strengthening of deep neck flexors and scapular stabilizers, combined with postural correction.
- Chronic Tendinopathies (e.g., patellar, Achilles, gluteal, lateral epicondylitis): Eccentric loading programs, progressive resistance training, and kinetic chain optimization are highly effective.
-
Ligamentous Laxity/Mild Instability:
- Patellofemoral Instability: Quadriceps strengthening (VMO focus), hip abductor/external rotator strengthening to improve patellar tracking.
- Ankle Instability: Proprioceptive training, balance exercises, and peroneal strengthening to enhance dynamic stability and prevent recurrent sprains.
- Shoulder Instability: Rotator cuff and scapular stabilizer strengthening to improve dynamic glenohumeral stability.
- Functional Limitations due to Deconditioning/Sarcopenia: Age-related muscle loss and general deconditioning significantly impair functional independence and increase fall risk. Progressive resistance training is critical.
- Postural Dysfunction: Strengthening core musculature, scapular retractors, and addressing muscle imbalances.
Pre-Operative Optimization (Pre-habilitation):
- Any Elective Orthopedic Surgery: Particularly for joint arthroplasty (hip, knee), spinal fusion, and major reconstructive procedures. Pre-habilitation aims to improve baseline strength, endurance, flexibility, and functional status, thereby enhancing post-operative recovery, reducing complications, and shortening length of hospital stay.
- Obese Patients Undergoing Surgery: Exercise combined with nutritional intervention can improve cardiovascular fitness and reduce operative risks.
Post-Operative Rehabilitation:
- Universal Indication: Following nearly all orthopedic surgical interventions (fracture fixation, arthroplasty, ligament/tendon repair/reconstruction, spinal surgery) to restore range of motion, strength, proprioception, and functional capacity. This will be elaborated in a subsequent section.
Contraindications for Exercise
While exercise is broadly beneficial, specific conditions and circumstances necessitate caution or complete cessation of certain activities.
- Acute Unstable Fractures: Until adequate stabilization (surgical or non-surgical) is achieved. Controlled, protected motion may begin earlier for certain stable fractures.
- Acute Inflammatory Arthropathy Exacerbations: High-impact or weight-bearing exercise during flares of rheumatoid arthritis, gout, or pseudogout can exacerbate inflammation and joint damage.
- Acute Severe Pain Limiting Function: Pain should be managed before initiating aggressive exercise. Relative contraindication, as gentle, pain-free ROM may still be beneficial.
- Unstable Angina, Decompensated Heart Failure, Uncontrolled Hypertension, Acute Myocardial Infarction: Require medical clearance and optimization of cardiovascular status.
- Active Infection (especially osteomyelitis or septic arthritis): Exercise is contraindicated; infection must be treated first.
- Recent Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE): Anticoagulation must be optimized and risk of embolization assessed before mobilization.
- Severe Neurological Deficits: Exercise prescription must be carefully adapted, often requiring assistive devices or specialized therapy.
- Progressive Neurological Conditions: Tailored programs are crucial to maintain function and prevent secondary complications, but strenuous exercise may be contraindicated.
Table: Operative vs. Non-Operative Indications in Orthopedics
| Condition/Pathology | Primary Non-Operative Management (Exercise-Centric) | Primary Operative Management (Exercise as Adjunct) |
|---|---|---|
| Osteoarthritis | Early-to-moderate stages (Kellgren-Lawrence Grades 1-3) with symptomatic relief via activity modification, progressive resistance, aerobic, and flexibility training. | Advanced stages (K-L Grade 4), intractable pain despite comprehensive non-operative treatment, significant functional impairment, severe deformity (e.g., Arthroplasty). |
| Rotator Cuff Pathology | Tendinopathy, partial thickness tears (<50% thickness), subacromial impingement with good pain control, strength, and ROM. | Full-thickness tears, large partial tears (>50% thickness), acute traumatic tears, irreparable tears with specific surgical indications (e.g., Repair, Reconstruction, Reverse Arthroplasty). |
| Spinal Conditions | Mechanical low back pain, discogenic pain (without radiculopathy), mild to moderate stenosis, mild spondylolisthesis, cervicogenic pain. | Progressive neurological deficit (motor weakness, myelopathy, cauda equina), intractable radiculopathy, unstable spinal fractures, severe deformity (e.g., Decompression, Fusion). |
| Ligamentous Instability | Mild ankle sprains, mild patellofemoral instability, mild shoulder instability with adequate dynamic stabilization from periarticular musculature. | Complete ligament ruptures (e.g., ACL, severe PCL), recurrent dislocations, chronic gross instability unresponsive to non-operative treatment (e.g., Reconstruction, Repair). |
| Fractures | Stable, non-displaced fractures managed non-surgically (e.g., distal radius, stable ankle, vertebral compression without neurological deficit). | Unstable, displaced, intra-articular fractures, open fractures, pathological fractures requiring stabilization (e.g., ORIF, IM Nailing, Arthroplasty). |
| Chronic Tendinopathies | Patellar, Achilles, gluteal, lateral epicondylitis unresponsive to conservative modalities but without severe structural damage (e.g., eccentric loading). | Recalcitrant tendinopathy with structural tears, enthesopathy with calcification requiring debridement, failed conservative management (e.g., Debridement, Repair, Biologic augmentation). |
Pre-Operative Planning & Patient Positioning
Pre-operative planning, particularly involving pre-habilitation, is a critical component of contemporary orthopedic surgical care, especially for elective procedures. It integrates the "benefits of exercise" into the surgical pathway, aiming to optimize patient physiology before the stress of surgery.
Pre-Operative Planning
-
Patient Assessment:
- Functional Baseline: Objective measurement of gait, balance, functional strength (e.g., 30-second chair stand, 6-minute walk test), and range of motion. Use validated patient-reported outcome measures (PROMs) such as the WOMAC, KOOS, DASH, or SF-36.
- Muscle Strength: Manual muscle testing (MMT) and dynamometry (handheld, isokinetic) to identify specific deficits.
- Cardiovascular Fitness: Assess aerobic capacity, often through questionnaires or formal stress testing, especially for patients with known comorbidities.
- Nutritional Status: Identify malnutrition or obesity, both of which negatively impact surgical outcomes.
- Psychological Readiness: Address anxiety, depression, or unrealistic expectations, which can influence adherence to pre- and post-operative protocols.
-
Risk Factor Modification:
- Obesity: Implement pre-operative weight loss programs.
- Smoking Cessation: Crucial for improving bone healing, reducing infection risk, and enhancing soft tissue healing.
- Glycemic Control: Optimize HbA1c in diabetic patients.
-
Pre-habilitation Program Design:
-
Tailored Exercise Prescription:
Based on the patient's baseline assessment and the specific surgical procedure.
- Aerobic Conditioning: Improves cardiovascular reserve, endurance, and reduces post-operative pulmonary complications.
- Resistance Training: Targets specific muscle groups that will be affected by surgery (e.g., quadriceps for TKA, rotator cuff for TSA) to build strength and mitigate post-operative atrophy.
- Flexibility and Range of Motion: Addresses pre-existing contractures or stiffness.
- Balance and Proprioception Training: Particularly for lower extremity surgeries, reduces fall risk.
- Patient Education: Comprehensive education on the surgical procedure, expected recovery trajectory, and the rationale for the pre-hab program.
- Duration: Typically 4-8 weeks prior to surgery. Even shorter durations have shown benefits.
-
Tailored Exercise Prescription:
Based on the patient's baseline assessment and the specific surgical procedure.
- Team Approach: Involves the orthopedic surgeon, physical therapist, occupational therapist, nutritionist, and primary care physician.
Patient Positioning (General Principles for Orthopedic Surgery)
Proper patient positioning is paramount in orthopedic surgery to ensure optimal surgical exposure, protect neural and vascular structures, prevent pressure injuries, and facilitate anesthetic management. While not directly related to exercise benefits, it is a critical component of pre-operative planning.
-
General Considerations:
- Access: Sufficient access to the surgical site and, if necessary, to the unaffected limb for comparisons or graft harvest.
- Anesthesia: Unobstructed access for airway management and intravenous lines.
- Imaging: Ability to obtain intraoperative fluoroscopic or radiographic images.
- Safety: Minimize risk of nerve compression, skin breakdown, vascular compromise, and falls.
-
Common Positions:
- Supine: Most common for anterior hip approaches, knee arthroplasty, and some upper extremity procedures. Requires careful padding of heels, sacrum, occiput, and ulnar nerves. Arms typically abducted on arm boards.
- Prone: Used for posterior spinal approaches, posterior hip approaches, and some Achilles tendon repairs. Requires chest rolls or spinal frames to offload abdominal pressure and facilitate ventilation. Careful attention to eyes, ears, nose, and male genitalia.
- Lateral Decubitus: Common for shoulder arthroscopy/arthroplasty (beach chair variant), lateral hip approaches, and some ankle/foot procedures. Adequate padding of the dependent arm, axilla, and peroneal nerve at the fibular head.
- Beach Chair: Semi-sitting position for shoulder arthroscopy/arthroplasty. Requires meticulous head and neck positioning to prevent cerebral hypoperfusion and ensure adequate venous return.
Detailed Surgical Approach / Technique
While exercise is not a surgical technique, a patient's exercise status (pre-operative conditioning and tissue quality) directly impacts the surgeon's operative field, decision-making, and the overall technical execution. This section outlines general principles of surgical technique in orthopedics, acknowledging the underlying influence of patient physiology modulated by exercise.
Principles of Orthopedic Surgical Technique (Influenced by Exercise Status)
-
Exposure and Incision:
- Internervous Planes: Respecting internervous planes (e.g., between sartorius and rectus femoris for anterior hip, deltoid and pectoralis for shoulder) minimizes muscle denervation and preserves function. A well-conditioned patient with less subcutaneous adipose tissue can often allow for a smaller, more precise incision and less extensive soft tissue dissection.
- Tissue Preservation: Minimizing collateral damage to muscles, tendons, and vascular structures is paramount. Tissues from well-conditioned patients often exhibit better vascularity and resilience, potentially leading to less intraoperative bleeding and enhanced healing potential.
- Retraction: Careful, judicious retraction to avoid undue tension on nerves and vessels. Healthy, pliable tissues from active patients often tolerate retraction better than atrophic, fibrotic tissues.
-
Pathology Addressing:
- Debridement/Resection: Precise removal of diseased tissue (e.g., osteophytes in OA, torn labrum, inflamed synovium). The extent of debridement can be influenced by the quality of surrounding tissues.
-
Repair/Reconstruction:
- Soft Tissue Repair (e.g., Rotator Cuff, Ligaments): Requires robust, healthy tissue for successful primary repair. Pre-operative exercise strengthening the surrounding muscles can improve the quality of the tendinous stump, making repair technically easier and more durable. Graft choice for reconstruction (autograft, allograft) is often dictated by patient factors and functional demands, influenced by their activity level.
- Fracture Reduction: Anatomical reduction is the goal for articular fractures to restore joint congruity and reduce post-traumatic OA. For metaphyseal/diaphyseal fractures, achieving appropriate alignment, rotation, and length is critical.
- Arthroplasty (Joint Replacement): Meticulous bone preparation, accurate component positioning, and soft tissue balancing are crucial. A patient with good pre-operative range of motion and muscle strength often allows for easier intraoperative soft tissue balancing and better early post-operative mobilization.
-
Fixation Principles:
- Biomechanical Stability: Achieving stable fixation (screws, plates, rods, sutures) is paramount for healing and early mobilization. Bone quality, significantly influenced by weight-bearing exercise (Wolff's Law), directly impacts implant purchase and stability. Osteoporotic bone presents greater challenges in achieving rigid fixation.
- Implant Selection: Choice of implant (e.g., intramedullary nail vs. plate, cemented vs. uncemented arthroplasty) considers bone quality, patient age, activity level, and fracture pattern.
- Suture Techniques: For soft tissue repairs, robust suture anchors and appropriate stitch configurations are vital to withstand early post-operative forces. The integrity of the tissue being repaired, often enhanced by pre-operative conditioning, directly affects the strength of the construct.
-
Intraoperative Considerations:
- Hemostasis: Meticulous control of bleeding reduces hematoma formation, infection risk, and improves visualization. Well-conditioned patients may have better vascular tone.
- Fluid Management: Crucial for maintaining hemodynamic stability.
- Tourniquet Use: Judicious application, minimizing duration to prevent nerve injury and reperfusion complications.
- Tissue Handling: Gentle handling of all tissues, particularly nerve and vascular structures, minimizes iatrogenic injury.
- Minimally Invasive Techniques: While often requiring specialized instrumentation and training, these techniques can reduce tissue disruption, pain, and recovery time. A well-conditioned patient can often tolerate and benefit more from these approaches due to inherent tissue resilience.
In essence, while surgery addresses structural pathology, the "canvas" upon which the surgeon operates—the patient's tissues, bone quality, muscle tone, and overall physiological reserve—is profoundly shaped by their exercise habits and overall physical conditioning. A patient optimized through pre-habilitation often presents a more favorable surgical environment, facilitating smoother execution, potentially lower complication rates, and more predictable recovery.
Complications & Management
Orthopedic surgery, despite advancements, is not without potential complications. A patient's pre-operative physical status, influenced by exercise, can impact the incidence of certain complications, and post-operative exercise is fundamental to their management.
Common Complications & Management
| Complication | Incidence (Approximate Range) | Description & Role of Exercise in Management / Prevention | Salvage / Management Strategies |
|---|---|---|---|
| Infection (SSI) | 0.5-5% (higher in certain procedures/patients) | Prevention: Pre-operative optimization (nutrition, glycemic control, smoking cessation), good skin hygiene. Exercise doesn't directly prevent SSI but improves overall physiological reserve. | Antibiotics (empirical then culture-specific), surgical debridement, irrigation, implant removal/exchange, wound VAC, muscle flap coverage. |
| Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) | 0.5-10% symptomatic, higher subclinical (procedure-dependent) | Prevention: Early post-operative mobilization, calf muscle pump exercises, ankle pumps, ambulation. Exercise enhances venous return. | Anticoagulation (LMWH, DOACs), compression stockings, IVC filter (rarely), urgent embolectomy for massive PE. |
| Nerve Injury | <1-3% (procedure/nerve dependent) | Prevention: Careful patient positioning, meticulous surgical technique, avoiding excessive traction. Exercise has no direct preventive role but can aid recovery if partial injury occurs. | Observation (for neurapraxia), neurolysis, nerve repair/grafting, tendon transfers for chronic deficits, bracing. |
| Vascular Injury | <1% (often associated with specific anatomical locations, e.g., popliteal artery in TKA) | Prevention: Meticulous surgical technique, anatomical knowledge. No direct role for exercise in prevention. | Urgent vascular repair/grafting, fasciotomy for compartment syndrome, limb salvage procedures. |
| Implant Failure (Loosening, Fracture) | 1-5% at 10 years (arthroplasty), variable for fixation | Prevention: Proper surgical technique, appropriate implant selection, optimal bone quality (influenced by lifelong weight-bearing exercise). Avoidance of premature excessive loading post-op. | Revision surgery (implant exchange, bone grafting, further fixation), activity modification. |
| Non-Union / Malunion (Fractures) | 5-10% (non-union), variable (malunion) | Prevention: Stable fixation, biological environment. Controlled, progressive loading (exercise) post-fixation can stimulate bone healing. Weight-bearing within limits. | Revision surgery (bone grafting, re-fixation, intramedullary nailing), electrical stimulation, biological augmentation. Osteotomy for malunion. |
| Arthrofibrosis / Stiffness | 5-20% (Knee/Shoulder, especially after trauma/surgery) | Management: Aggressive, early, controlled range of motion exercises, stretching, strengthening. Exercise is the primary non-surgical treatment. | Manipulation under anesthesia (MUA), arthroscopic or open arthrolysis, continuous passive motion (CPM). |
| Persistent Pain | 10-30% (variable etiology, nerve, soft tissue, central sensitization) | Management: Multimodal approach including therapeutic exercise to improve function, strength, and proprioception. Address deconditioning, muscle imbalances. | Multimodal pain management (analgesics, nerve blocks, neuromodulation, psychological support), revision surgery (if mechanical cause), physical therapy. |
| Heterotopic Ossification (HO) | 10-60% (especially after hip trauma/arthroplasty, spinal surgery) | Prevention: Prophylaxis (NSAIDs, radiation therapy). Early, aggressive range of motion exercises can sometimes mitigate stiffness but is not a primary prevention for HO formation itself. | Radiation therapy, surgical excision (only after maturation of HO, typically 6-12 months post-onset) followed by aggressive ROM. |
| Complex Regional Pain Syndrome (CRPS) | <1% (especially upper extremity trauma/surgery) | Management: Early mobilization, stress loading exercises (scrubbing, carrying), desensitization, graded motor imagery. Exercise is a key therapeutic component. | Multimodal pain management (nerve blocks, neuromodulation, physical therapy, occupational therapy, psychological support, medications). |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is the definitive stage where the benefits of structured exercise are most directly observed and implemented, aiming to restore function, prevent complications, and optimize long-term outcomes. Protocols are typically phased, guided by tissue healing timelines and individualized based on the patient, procedure, and surgeon's preference.
General Principles of Post-Operative Rehabilitation
- Tissue Healing Constraints: Respect the biological timelines of tissue healing (inflammation, proliferation, remodeling). Premature loading can disrupt repairs; prolonged immobilization can lead to stiffness and atrophy.
- Gradual Progression: Exercise intensity, volume, and complexity increase incrementally as the patient's condition improves and tissues heal.
- Individualization: Protocols must be tailored to the specific patient's age, comorbidities, pre-operative functional status, and goals.
- Pain as a Guide: While some discomfort is expected, exercises should generally be performed within a tolerable pain limit.
- Interdisciplinary Approach: Collaboration between the surgeon, physical therapist, occupational therapist, and pain management specialists is crucial.
Phased Rehabilitation Approach
Phase I: Acute / Protective Phase (Days to Weeks Post-Op)
- Goals: Protect the surgical repair/site, manage pain and swelling, minimize muscle atrophy, restore initial range of motion (ROM), and achieve independent functional mobility within precautions.
-
Exercises:
- Pain & Swelling Management: RICE (Rest, Ice, Compression, Elevation).
- Early ROM: Passive or assisted active range of motion (AAROM) within safe limits (e.g., CPM machine for TKA, pendulum exercises for shoulder). Avoid movements that stress the repair.
- Muscle Activation: Gentle isometric contractions (e.g., quad sets, gluteal sets, scapular squeezes) to maintain muscle tone without joint movement.
- Weight-Bearing: Strictly follow surgeon's weight-bearing precautions (NWB, PWB, WBAT). Gait training with assistive devices.
- Circulation: Ankle pumps, gentle foot/hand exercises to prevent DVT.
- Criteria for Progression: Controlled pain/swelling, wound healing, achievement of specific ROM milestones, independent functional mobility with assistive devices.
Phase II: Subacute / Controlled Motion Phase (Weeks to Months Post-Op)
- Goals: Restore full or functional ROM, gradually increase muscle strength and endurance, improve proprioception and neuromuscular control, and progress functional activities.
-
Exercises:
- Progressive ROM: Active range of motion (AROM), gentle stretching, sustained holds to regain lost motion. Manual therapy by a therapist.
-
Progressive Strengthening:
- Isotonic Exercises: Start with low resistance and high repetitions, gradually increasing resistance (e.g., therabands, light weights).
- Eccentric Training: Crucial for tendon healing and strength, introduced cautiously.
- Closed Chain Exercises: (e.g., mini-squats, wall slides for knee; push-ups for shoulder) to improve joint stability and co-contraction.
- Proprioception & Balance: Single-leg stance, unstable surface training (e.g., wobble board), gait retraining, visual feedback exercises.
- Endurance: Stationary cycling, elliptical, swimming (once wounds healed).
- Functional Training: Light ADLs, gradual progression to tasks simulating daily life.
- Criteria for Progression: Adequate pain control, full functional ROM, absence of joint effusion, specific strength gains, improved balance, independent functional mobility without assistive devices.
Phase III: Return to Function / Strength & Conditioning Phase (Months to Year+ Post-Op)
- Goals: Optimize muscle strength, power, and endurance; restore pre-injury/pre-surgical functional levels; prepare for return to sport/work; prevent re-injury.
-
Exercises:
- Advanced Strengthening: High-intensity resistance training, plyometrics (jumping, bounding), sport-specific drills, agility training.
- Cardiovascular Endurance: Higher intensity aerobic training.
- Complex Functional Training: Advanced balance exercises, multi-directional movements, carrying/lifting tasks, simulated work/sport activities.
- Maintenance Program: Development of a lifelong exercise program to maintain gains and prevent recurrence.
- Criteria for Progression: Achievement of symmetric strength and power, excellent neuromuscular control, absence of pain/instability during advanced activities, completion of functional performance testing (e.g., hop tests for knee, throwing velocity for shoulder).
- Return to Sport/Activity: Often involves a graduated return-to-play protocol, with specific criteria for each stage.
Specific Rehabilitation Modalities and Considerations
- Manual Therapy: Joint mobilizations, soft tissue mobilization, massage to address restrictions and pain.
- Modalities: Heat, cold, electrical stimulation (for pain, muscle re-education), ultrasound (limited evidence for direct tissue healing).
- Patient Education and Home Exercise Programs: Empowering patients to take an active role in their recovery is critical for long-term adherence and success.
Summary of Key Literature / Guidelines
The evidence base supporting structured exercise in orthopedic health is robust and continuously expanding. Major orthopedic societies and national health organizations routinely publish guidelines that underscore its importance.
Key Evidence and Guidelines:
-
Osteoarthritis (OA):
- AAOS (American Academy of Orthopaedic Surgeons) Guidelines: Strongly recommend exercise (aerobic, strengthening, aquatic) for symptomatic knee and hip OA. Numerous meta-analyses demonstrate exercise efficacy in reducing pain and improving function, often comparable to pharmacological interventions.
- ACR (American College of Rheumatology) Recommendations: Similarly endorse exercise as a core non-pharmacologic treatment for OA of the hand, hip, and knee.
- OARSI (Osteoarthritis Research Society International) Guidelines: Emphasize individualized exercise programs, including land-based strengthening and aerobic exercises, for all patients with OA, regardless of severity.
- Mechanism: Exercise improves muscle strength (reducing joint load), enhances joint stability, maintains cartilage nutrition, and modulates pain perception.
-
Chronic Low Back Pain (CLBP):
- Cochrane Reviews & Clinical Guidelines (e.g., NICE, AAOS): Consistently recommend exercise therapy (motor control, core stabilization, strength, aerobic) as a primary treatment for CLBP, demonstrating superiority over usual care or passive modalities.
- Mechanism: Strengthens core musculature, improves spinal stability, enhances segmental control, reduces fear-avoidance behaviors, and improves overall physical conditioning.
-
Rotator Cuff Pathology:
- AAOS Clinical Practice Guidelines: Recommend non-operative management, including therapeutic exercise, for partial-thickness rotator cuff tears and impingement syndrome. Pre-operative strengthening has shown to improve tissue quality prior to repair.
- Post-operative Rehabilitation: Essential for optimizing outcomes after rotator cuff repair, with phased protocols guided by biological healing. Evidence supports early, controlled passive motion progressing to active and resisted movements.
-
Pre-habilitation:
- Systematic Reviews and Meta-analyses: Demonstrate that pre-operative exercise programs (pre-habilitation) for elective orthopedic surgeries (especially TKA, THA, spine surgery) lead to improved functional capacity, shorter hospital stays, reduced post-operative complications, and enhanced recovery trajectories.
- Mechanism: Builds physiological reserve, improves muscle strength and endurance, enhances psychological readiness, and familiarizes patients with post-operative exercises.
-
Post-Operative Rehabilitation (General Principles):
- Evidence-Based Protocols: Most orthopedic surgical procedures have well-established, phased rehabilitation protocols supported by research, defining safe ROM limits, weight-bearing precautions, and progressive strengthening milestones.
- Examples: ACL reconstruction rehabilitation (early weight-bearing, controlled motion, progressive strengthening focusing on neuromuscular control and return to sport), joint arthroplasty rehabilitation (early mobilization, ROM, strengthening to regain independence).
- Mechanism: Prevents stiffness (arthrofibrosis), restores muscle strength and endurance, improves proprioception, reduces pain, and facilitates a safe return to activity.
The Future of Exercise in Orthopedics:
Emerging research focuses on personalized exercise prescriptions based on genetic predispositions, biomechanical analysis, and advanced imaging. The integration of technology (wearable sensors, virtual reality, telerehabilitation) is expanding the reach and effectiveness of exercise interventions, allowing for more precise monitoring and feedback.
In conclusion, structured exercise is not merely an adjunctive therapy but an integral and indispensable component of modern orthopedic care. From preventing disease progression and serving as a primary non-operative treatment to critically influencing surgical outcomes through pre-habilitation and dictating the success of post-operative recovery, its profound benefits resonate throughout the orthopedic surgical landscape. A deep understanding of its scientific underpinnings and diligent application are hallmarks of comprehensive orthopedic practice.
You Might Also Like