Distal Radius Fractures: Comprehensive Guide to Surgical Anatomy, Biomechanics & Management
Key Takeaway
Distal radius fractures (DRFs) are common upper extremity injuries. Treatment aims to restore anatomical parameters—radial length, inclination, and volar tilt—and articular congruity for optimal function and complication prevention. Management integrates fracture characteristics, patient factors, detailed surgical anatomy, and biomechanics, guiding decisions for non-operative or operative strategies.
Reduction Technique & Treatment: Essential Guide for The Wrist
Introduction & Epidemiology
Distal radius fractures (DRFs) represent the most prevalent osseous injury of the upper extremity, accounting for approximately one-sixth of all fractures encountered in clinical practice. The incidence exhibits a bimodal distribution, affecting younger, active individuals involved in high-energy trauma, and a significantly larger cohort of osteoporotic elderly patients sustaining low-energy falls. The primary mechanism of injury is typically a fall onto an outstretched hand (FOOSH), leading to varying degrees of comminution, displacement, and articular involvement.
The goal of treatment, irrespective of the chosen modality, is the restoration of anatomical parameters—specifically radial length, radial inclination, and volar tilt—and articular congruity to optimize functional outcomes and mitigate the risk of post-traumatic arthrosis and other complications. Numerous classification systems exist to characterize DRFs, including Frykman, AO, Fernandez, and Universal classifications, each providing a framework for understanding fracture morphology, stability, and guiding treatment decisions. While the trend towards operative management has increased, particularly with the advent of volar locking plate technology, a significant proportion of DRFs can still be effectively managed non-operatively.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy and biomechanics of the distal radius and carpus is paramount for effective treatment.
Surgical Anatomy
- Distal Radius: The distal radius flares distally, comprising the radial styloid, the sigmoid notch (articulating with the ulnar head), and the articular surface for the carpus (scaphoid and lunate fossae). The volar cortex is typically thicker and denser than the dorsal cortex, a critical consideration for implant placement. The watershed line on the volar aspect serves as a crucial landmark, delineating the safe zone for volar plate placement to avoid flexor tendon irritation.
- Distal Ulna & DRUJ: The ulnar head articulates with the sigmoid notch of the radius, forming the distal radioulnar joint (DRUJ). Stability of the DRUJ is conferred by the triangular fibrocartilage complex (TFCC), which originates from the distal radius and inserts into the ulnar fovea and styloid process. Ulnar styloid fractures are common concomitants of DRFs and can indicate potential TFCC injury or DRUJ instability.
- Carpus: The carpus consists of eight bones arranged in two rows. The scaphoid and lunate articulate with the distal radius, forming the radiocarpal joint. Ligamentous stability, particularly the scapholunate and lunotriquetral ligaments (intrinsic) and robust extrinsic ligaments (e.g., radioscaphocapitate, long/short radiolunate), is crucial for maintaining carpal alignment and load distribution.
- Tendons: The dorsal compartment houses the extensor tendons, organized into six compartments. The extensor pollicis longus (EPL) tendon, traversing Lister's tubercle, is particularly vulnerable to irritation or rupture in dorsal plating or malunion. The volar aspect contains the flexor tendons and the median nerve within the carpal tunnel.
- Neurovascular Structures: The median nerve, radial artery, and ulnar neurovascular bundle are susceptible to injury or compression in the setting of DRFs. The superficial radial nerve crosses the distal forearm dorsoradially, requiring careful retraction during radial-sided approaches.
Biomechanics
The distal radius bears approximately 80% of the axial load transmitted across the wrist, with the remaining 20% handled by the ulna and TFCC. Normal anatomical parameters include:
*
Radial Length (or Radial Height):
Approximately 11-12 mm, measured from the ulnar aspect of the lunate fossa to the tip of the radial styloid on a PA radiograph. Loss of radial length can lead to ulnocarpal impaction and DRUJ dysfunction.
*
Radial Inclination:
Approximately 22-23°, measured as the angle between a line perpendicular to the long axis of the radius and a line connecting the radial styloid tip to the ulnar aspect of the lunate fossa on a PA radiograph.
*
Volar Tilt (or Palmar Tilt):
Approximately 11-12° (range 0-20°), measured as the angle between the articular surface of the distal radius and a line perpendicular to the long axis of the radius on a lateral radiograph. Dorsal angulation is a characteristic feature of Colles' fractures.
*
Articular Congruity:
Maintenance of a smooth articular surface, with intra-articular step-off or gap typically not exceeding 1-2 mm.
Deforming forces in DRFs include the impact force of the initial injury, muscle pull from the brachioradialis (causing proximal migration and radial deviation), pronator quadratus (causing pronation and volar displacement of the distal fragment), and extrinsic wrist flexors and extensors. These forces contribute to characteristic deformities observed in different fracture patterns.
Indications & Contraindications
The decision between non-operative and operative management for distal radius fractures is complex and multifactorial, considering fracture characteristics, patient factors, and surgeon experience.
Indications for Non-Operative Management
Non-operative treatment is generally reserved for stable fractures with acceptable alignment or those that achieve acceptable reduction and stability following closed manipulation. Specific radiographic criteria for acceptable reduction typically include:
* Radial inclination: ≥ 15°
* Volar tilt: Neutral to 15° volar (some tolerate up to 5-10° dorsal in low-demand elderly patients)
* Radial length: < 3 mm shortening relative to the contralateral wrist
* Intra-articular step-off or gap: < 1-2 mm
* DRUJ congruity: Maintained
Patient-specific factors also play a significant role. Elderly, low-demand patients with significant comorbidities may tolerate a greater degree of residual deformity if functional outcomes are not significantly compromised and surgical risks outweigh potential benefits.
Indications for Operative Management
Operative intervention is indicated when anatomical reduction cannot be achieved or maintained non-operatively, or when fracture characteristics predict a high likelihood of poor functional outcome with conservative treatment.
- Unstable Fractures: Fractures that displace after initial closed reduction, high-energy fractures with significant comminution, or those with inherent instability patterns.
- Irreducible Fractures: Inability to achieve acceptable reduction via closed manipulation, often due to soft tissue interposition (e.g., pronator quadratus, FPL tendon, periosteum) or significant comminution.
- Intra-articular Displacement: Articular step-off or gap > 2 mm.
- Significant Dorsal Tilt: Persistent dorsal angulation > 10-20° (thresholds vary, but often > 10° in younger patients, > 15-20° in older patients).
- Significant Radial Shortening: Radial length loss > 3-5 mm.
- Loss of Radial Inclination: Radial inclination < 15°.
- Open Fractures: Require surgical debridement and stabilization.
- Associated Injuries: Carpal instability (e.g., scapholunate dissociation), TFCC tears with DRUJ instability, concomitant nerve compression (e.g., acute carpal tunnel syndrome).
- Patient Factors: Young, active, high-demand individuals where optimal anatomical restoration is critical for long-term function.
Contraindications
Absolute contraindications to surgery are rare and typically relate to the patient's overall medical status rendering them unfit for anesthesia and surgical intervention. Relative contraindications include severe osteopenia where implant purchase is compromised, active local or systemic infection, or pre-existing severe medical comorbidities that elevate surgical risk beyond the potential benefit. In such cases, a less invasive approach or palliation may be considered.
Summary of Operative vs. Non-Operative Indications
| Parameter | Non-Operative Management (Conservative) | Operative Management (Surgical) |
|---|---|---|
| Fracture Stability | Minimally displaced; Stable after closed reduction. | Unstable; Displaced or re-displaced after closed reduction. |
| Articular Involvement | Intra-articular step-off/gap < 1-2 mm. | Intra-articular step-off/gap ≥ 2 mm. |
| Dorsal Angulation | Volar tilt 0-15°; Acceptable dorsal tilt (e.g., < 10-20° in specific cases). | Dorsal tilt ≥ 10-20° (varies by patient/surgeon). |
| Radial Length | Radial shortening < 3 mm. | Radial shortening ≥ 3-5 mm. |
| Radial Inclination | Radial inclination ≥ 15°. | Radial inclination < 15°. |
| Irreducibility | Not applicable; easily reducible. | Inability to achieve/maintain acceptable reduction. |
| Open Fractures | Not applicable. | All open fractures require surgical management. |
| Associated Injuries | No significant associated carpal instability or acute nerve compromise. | Acute carpal tunnel syndrome, carpal instability, severe DRUJ instability. |
| Patient Demands | Low-demand, elderly patient. | Young, active, high-demand patient requiring optimal functional recovery. |
| Medical Status | Unfit for surgery due to severe comorbidities. | Medically stable and fit for anesthesia and surgical intervention. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for optimizing outcomes and minimizing complications in distal radius fracture management.
Pre-Operative Planning
- Clinical Assessment: A thorough history focusing on mechanism of injury, hand dominance, occupation, and baseline functional status. Physical examination includes neurovascular assessment, evaluation for open wounds, and assessment of associated injuries (e.g., carpal, elbow, shoulder).
- Radiographic Assessment: Standard PA, lateral, and oblique radiographs are essential. For intra-articular or complex comminuted fractures, a Computed Tomography (CT) scan is highly recommended. This provides detailed information regarding articular involvement, fragment size and location, and helps differentiate volar from dorsal comminution. CT allows for virtual reduction and precise implant selection and placement strategy.
-
Anesthetic Consultation:
Anesthetic choice is a crucial decision point. As per established guidelines:
"Anaesthesia is necessary for the reduction of this fracture, and either a general anaesthetic or intravenous regional anaesthetic (Bier block) may be used with success. Although the latter has a good safety record, it should not be employed unless facilities for resuscitation are freely available. Where there is a preference for general anaesthesia but the patient attends late at night with a history of recent intake of food or drink, it is permissible and often safer to apply a temporary plaster back shell and an arm sling, and delay reduction of the fracture till morning."
Peripheral nerve blocks (e.g., supraclavicular, interscalene) can also be utilized, offering post-operative analgesia.
- Equipment Preparation: This includes fluoroscopy unit, specialized hand table, finger trap traction device (e.g., Chinese finger traps), pneumatic tourniquet, standard orthopedic instrument set, K-wires, various volar locking plates (different sizes and designs), plate-specific instruments (drill guides, t-handles), and possibly external fixator components or dorsal plating systems depending on the planned approach. Arthroscope and related equipment should be available if arthroscopically-assisted reduction is planned.
-
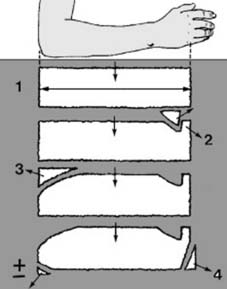
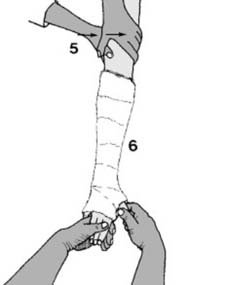
Plaster Back Slab Preparation (for post-reduction immobilization or delayed definitive fixation):
"Before any manipulation, start by preparing a suitable plaster back slab. The length should equal the distance from the olecranon to the metacarpal heads (1). The width in an adult should be 15 cm (6″), and it should be about eight layers thick. The slab should be trimmed with a tongue (2) for the first web space, a large radial curve to allow elbow flexion (3) and allowance for ulnar deviation (4)." This meticulous preparation ensures proper immobilization post-reduction.

Patient Positioning
The patient is typically positioned supine on the operating table.
*
Arm Placement:
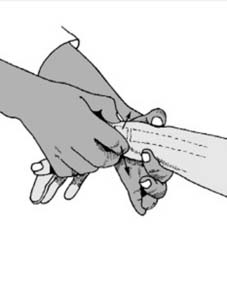
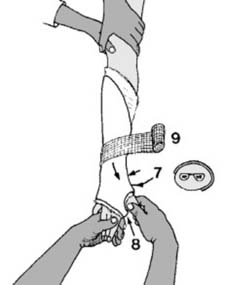
The affected arm is placed on a radiolucent hand table. For traction, Chinese finger traps are applied to the index, middle, and ring fingers, suspended from an IV pole or a dedicated traction tower at a 90-degree angle to the forearm, providing ligamentotaxis. This aids in fracture disimpaction and elongation. Counter-traction is applied via an unpadded strap around the upper arm.
*
Tourniquet:
A pneumatic tourniquet is applied high on the upper arm to ensure a bloodless field, typically inflated to 250-300 mmHg, or 100 mmHg above systolic blood pressure.
*
Fluoroscopy:
The C-arm fluoroscopy unit is positioned to allow facile acquisition of true PA and lateral views of the distal radius without needing to reposition the arm. This is crucial for real-time assessment of reduction and hardware placement.
*
Sterile Field:
The entire arm, from the tourniquet down to the fingertips, is prepped and draped in a sterile fashion, allowing for visualization of the hand, wrist, and forearm.
Detailed Surgical Approach / Technique
The choice of surgical technique is dictated by fracture pattern, surgeon preference, and patient factors. The volar approach with locking plate fixation is currently the most prevalent method.
Principles of Reduction
Regardless of the approach, the fundamental principles of reduction remain consistent:
1.
Disimpaction and Ligamentotaxis:
Axial traction is applied to disengage impacted fragments and utilize intact ligamentous structures to aid in reduction. This is often achieved with finger traps.
2.
Correction of Deformity:
Address dorsal angulation, radial shortening, and loss of radial inclination.
3.
Articular Congruity:
Restore the smooth articular surface, especially in intra-articular fractures, to minimize post-traumatic arthrosis.
4.
Stability:
Maintain reduction using external or internal fixation to allow for early functional rehabilitation.
Closed Reduction and Percutaneous Pinning (if indicated)
For fractures amenable to closed reduction (typically extra-articular or simple intra-articular patterns), the technique involves:
1.
Anesthesia:
As previously discussed (General, Bier block, or regional nerve block).
2.
Traction:
Apply longitudinal traction via finger traps or manual pull.
3.
Exaggeration and Disimpaction:
Exaggerate the deformity (e.g., hyperextension for a Colles' fracture) to disimpact fragments.
4.
Manipulation:
Apply direct pressure to the displaced fragments. For a dorsally displaced Colles' fracture, apply volar pressure over the distal fragment while simultaneously applying counter-traction and pronating the forearm.

5.
Fluoroscopic Assessment:
Evaluate reduction in PA and lateral views.
6.
Stabilization:
If deemed stable and within acceptable radiographic parameters, apply a well-molded cast (e.g., sugar tong or dorsal/volar splint). If unstable after reduction, percutaneous K-wire fixation can be considered. K-wires can be inserted from the radial styloid into the proximal radius or across the fracture site to hold articular fragments.

Open Reduction Internal Fixation (ORIF) - Volar Approach
The volar approach via Henry's approach is the most common technique for unstable distal radius fractures, particularly those with volar comminution or dorsal displacement.
- Incision: A longitudinal incision is made on the volar aspect of the forearm, centered over the flexor carpi radialis (FCR) tendon, extending from the distal forearm crease proximally to just proximal to the wrist crease distally.
-
Dissection:
- Subcutaneous dissection, identifying and protecting the palmar cutaneous branch of the median nerve and radial artery branches.
- The antebrachial fascia is incised longitudinally, typically lateral to the FCR tendon.
-
The FCR tendon is identified and retracted ulnarly. The radial artery is typically retracted radially.

- The pronator quadratus (PQ) muscle is then exposed. It lies directly over the volar aspect of the distal radius.
-
The PQ is carefully elevated from its radial origin off the radius using an elevator. This allows exposure of the volar cortex of the distal radius. Efforts should be made to preserve its ulnar insertion if possible, as this contributes to DRUJ stability and muscle function.

-
The fracture hematoma is evacuated, and the fracture fragments are visualized.

-
Reduction:
- Under direct visualization and fluoroscopic guidance, the fracture is reduced.
- Ligamentotaxis with traction facilitates initial length restoration.
- Specific articular fragments, particularly those involving the lunate fossa, are manipulated with K-wires used as joysticks, dental picks, or small elevators.
-
Temporary K-wire fixation can be employed to hold key fragments in reduction.
- Volar angulation and radial inclination are restored. Bone graft (autograft or allograft) or bone graft substitute may be used to fill metaphyseal defects, particularly with significant comminution.
-
Fixation:
-
A volar locking plate, contoured to the distal radius, is selected. The plate should be positioned just proximal to the watershed line to minimize flexor tendon irritation.
- Initial fixation typically involves a non-locking screw proximally to secure the plate to the radial shaft, allowing fine-tuning of plate position.
-
Distal locking screws are then inserted. These screws are designed to provide subchondral support, capturing small articular fragments and resisting collapse. Screw length must be carefully measured to avoid dorsal cortex penetration and potential extensor tendon irritation or rupture.
 ](https://musculoskeletalkey.com/wp-content/uploads/2017/03/B9780443068768100097_gr28.jpg)
](https://musculoskeletalkey.com/wp-content/uploads/2017/03/B9780443068768100097_gr28.jpg)
- Subsequent proximal locking screws are inserted, ensuring adequate cortical purchase.
-
Final fluoroscopic images (PA and lateral) are obtained to confirm plate and screw position, reduction parameters (radial length, inclination, volar tilt), and articular congruity. Special attention is paid to screw length to avoid dorsal prominence or penetration of the DRUJ.

-
A volar locking plate, contoured to the distal radius, is selected. The plate should be positioned just proximal to the watershed line to minimize flexor tendon irritation.
- Closure: The pronator quadratus muscle is meticulously repaired over the plate, if possible, providing an important soft tissue buffer for the flexor tendons. The fascia and subcutaneous layers are closed, followed by skin closure.
External Fixation
External fixation (bridging or non-bridging) may be indicated for severely comminuted fractures, open fractures, or those with significant soft tissue compromise. It can also be used as a temporizing measure. Pins are inserted into the radius and often the second metacarpal for bridging constructs. Ligamentotaxis is achieved by distraction. Adjunctive K-wires are often used to address articular fragments.
Complications & Management
Distal radius fractures, even with optimal management, are associated with a range of potential complications. Proactive recognition and timely intervention are crucial for salvage.
Table of Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approximate) | Pathophysiology / Clinical Presentation | Salvage Strategy |
|---|---|---|---|
| Malunion | 10-30% | Persistent deformity in radial length, inclination, or volar tilt. Leads to pain, decreased range of motion (ROM), altered wrist mechanics, carpal instability, DRUJ dysfunction, and premature osteoarthrosis. Clinically manifest as reduced grip strength, limited forearm rotation, chronic pain. | Early: Corrective osteotomy (opening or closing wedge) with internal fixation. Late: Fusion (radiocarpal, DRUJ) or partial wrist denervation for pain. Distal ulna procedures (Darrach, Sauve-Kapandji) for DRUJ issues. |
| Nonunion | Rare (<1%) | Failure of fracture fragments to heal after 6-9 months, usually due to severe comminution, inadequate fixation, or infection. Presents with persistent pain, instability, and delayed healing signs on imaging. | Open reduction with debridement of fibrous tissue, bone grafting (autogenous cancellous), and stable internal fixation (e.g., locking plate). |
| Post-traumatic Arthritis | 10-20% (intra-articular) | Primarily due to irreducible intra-articular step-off/gap (> 1-2 mm) or malunion leading to altered joint mechanics and cartilage wear. Symptoms include chronic pain, stiffness, crepitus, and swelling. | Early: Corrective osteotomy to restore articular congruity. Late: Partial or total wrist arthrodesis, proximal row carpectomy (PRC), or wrist arthroplasty (less common). |
| Median Nerve Compression | 5-15% | Acute carpal tunnel syndrome (due to fracture hematoma, fragment displacement, or swelling) or chronic compression from malunion or prominent hardware. Presents with paresthesias, numbness in median nerve distribution, pain, thenar weakness. | Acute: Emergent carpal tunnel release (CTR) and fracture reduction/stabilization. Chronic: CTR, potentially hardware removal if prominent, or corrective osteotomy for malunion. |
| Tendon Rupture | 1-5% (EPL most common) | EPL: Typically late onset (weeks to months post-injury) due to attrition over sharp bone fragments (Lister's tubercle) or prominent dorsal hardware. Presents as inability to actively extend the thumb IP joint. Flexor tendons (FPL): Less common, usually due to prominent volar hardware. Presents as inability to flex thumb IP. | EPL: Tendon transfer (e.g., extensor indicis proprius). Flexor tendons: Direct repair or tendon grafting, often requiring hardware removal. |
| Complex Regional Pain Syndrome (CRPS) Type I | 2-5% (variable) | A painful, debilitating condition characterized by severe pain, edema, stiffness, skin changes (trophic), and autonomic dysfunction (sweating, temperature dysregulation). Onset usually within weeks of injury. Pathophysiology poorly understood. | Early recognition and multidisciplinary approach: intensive physical/occupational therapy, neuropathic pain medications, stellate ganglion blocks, psychological support. Early mobilization and pain control are preventive. |
| Distal Radioulnar Joint (DRUJ) Instability / Arthritis | 5-10% | Result of TFCC injury, ulnar styloid nonunion, malunion of distal radius leading to incongruity, or iatrogenic injury. Presents as pain with forearm rotation, clicking, instability. | Acute: TFCC repair, ulnar styloid fixation. Chronic: TFCC reconstruction, DRUJ stabilization procedures, Darrach procedure, Sauve-Kapandji, or wafer resection for arthritis. Corrective osteotomy for radial malunion. |
| Hardware-Related Complications | 5-10% | Screw prominence (dorsal cortical breach causing tendon irritation/rupture, volar breach causing flexor tendon irritation), plate impingement, infection, implant loosening. | Hardware removal, revision surgery (e.g., shorter screws, different plate contour), antibiotics for infection, debridement. |
| Infection | < 2% (ORIF) | Superficial or deep wound infection. Presents with redness, swelling, pain, purulent discharge, fever. Higher risk in open fractures or immunocompromised patients. | Debridement, irrigation, culture-specific antibiotics. Deep infections may require hardware removal, especially if chronic or if union is achieved. |
| Loss of Reduction | 5-15% (conservative) | Recurrent displacement of fracture fragments after initial reduction and casting, due to unstable fracture pattern, inadequate cast molding, or premature mobilization. | Repeat closed reduction and casting (if still possible and acceptable), or conversion to operative management (ORIF, external fixation). |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is an integral component of successful treatment for distal radius fractures, aiming to restore wrist function, strength, and range of motion while protecting the fixation. Protocols vary based on fracture stability, type of fixation, and surgeon preference.
Immediate Post-Operative Phase (Days 0-2 Weeks)
- Immobilization: A well-padded sugar tong splint or dorsal/volar splint is typically applied post-surgery to provide comfort and protect the surgical site. For stable fixation (e.g., volar locking plate), rigid cast immobilization may be avoided. For less stable constructs (e.g., K-wires, external fixator), more rigid or longer immobilization may be necessary.
- Pain Management: Administer appropriate analgesics, including multimodal regimens, to control post-operative pain and facilitate early motion.
- Edema Control: Elevate the hand above heart level continuously. Apply ice packs intermittently to reduce swelling.
- Early Active Motion (Non-Restricted Joints): Encourage immediate active range of motion (ROM) of the digits, elbow, and shoulder to prevent stiffness and manage swelling. This includes finger flexion/extension, pronation/supination of the forearm (if fixation allows, especially with volar plates), elbow flexion/extension, and shoulder circumduction.
- Wound Care: Monitor incision site for signs of infection. Dressing changes as per protocol.
Early Mobilization Phase (2-6 Weeks Post-Op)
- Transition to Removable Orthosis: If fixation is stable (e.g., volar locking plate), the static splint is typically discontinued, and a removable wrist brace or dynamic splint may be introduced, allowing for controlled, protected wrist motion.
- Active Wrist ROM: Initiate gentle, active wrist flexion, extension, radial and ulnar deviation, and forearm pronation/supination. Progression is guided by pain and swelling.
- Passive Wrist ROM: Gentle passive ROM exercises may be introduced by a physical or occupational therapist, carefully avoiding forceful manipulations.
- Light Grip Strengthening: Begin with gentle grip exercises using soft putty or sponges.
- Scar Management: Initiate scar massage and desensitization techniques once the incision is healed.
- Neurovascular Monitoring: Continue monitoring for signs of median nerve compression or CRPS.
Intermediate Rehabilitation Phase (6-12 Weeks Post-Op)
- Progressive Strengthening: Advance strengthening exercises for wrist and forearm muscles using resistance bands, light weights, and functional activities. Focus on improving grip strength and fine motor skills.
- Advanced ROM: Progress active and passive ROM to achieve full pain-free motion.
- Proprioception and Coordination: Introduce balance and coordination exercises specific to the upper extremity.
- Activities of Daily Living (ADLs): Gradually increase participation in ADLs, avoiding heavy lifting or impact loading.
- Work/Sport Specific Training: Begin tailored exercises for return to work or sport, if applicable.
Late Rehabilitation Phase (12+ Weeks Post-Op)
- Full Activity Resumption: Gradual return to full work, recreational activities, and sports, depending on recovery and fracture healing.
- Residual Deficits: Address any persistent limitations in strength, endurance, or ROM.
- Long-Term Follow-up: Monitor for late complications such as malunion, nonunion, or post-traumatic arthritis. Implant removal may be considered in symptomatic cases.
For non-operatively managed fractures, the initial immobilization period is typically longer (4-6 weeks in a cast), followed by a similar progression of ROM and strengthening exercises once the cast is removed. The overall duration of rehabilitation is highly individualized and depends on fracture severity, patient age, general health, and compliance with the rehabilitation program.
Summary of Key Literature / Guidelines
The management of distal radius fractures has evolved significantly over recent decades, driven by advancements in surgical techniques and implant technology, particularly the widespread adoption of volar locking plates (VLPs).
Volar Locking Plates (VLPs) vs. Other Fixation Methods
- VLPs vs. K-wires: Numerous Level I randomized controlled trials (RCTs) and systematic reviews have demonstrated superior functional outcomes, earlier mobilization, and reduced reoperation rates for unstable distal radius fractures treated with VLPs compared to K-wire fixation, particularly in older patients. VLPs provide superior stability, enabling immediate post-operative wrist motion.
- VLPs vs. External Fixation: While external fixation (EF) remains a viable option for highly comminuted or open fractures, VLPs have shown comparable or superior functional outcomes in many unstable DRFs, with the advantage of avoiding pin site complications and allowing earlier functional use without bulky external hardware. EF often still requires supplemental K-wires for articular fragments.
- VLPs vs. Dorsal Plating: Volar plating has largely supplanted dorsal plating for most DRFs due to the thicker volar cortex providing better screw purchase, the ability to restore volar tilt, and reduced risk of extensor tendon irritation compared to dorsal plates. Dorsal plating may be reserved for specific fracture patterns involving severe dorsal comminution not addressable from a volar approach.
Acceptable Reduction Parameters
Debate continues regarding "acceptable" radiographic reduction parameters, particularly in elderly, low-demand patients. While stringent criteria (e.g., < 2 mm articular step-off, < 10° dorsal tilt, < 2 mm radial shortening) are generally advocated for younger, active patients, some studies suggest that older, low-demand individuals can tolerate greater residual deformity without significant functional compromise, particularly if pain control is achieved. However, the current consensus leans towards anatomical restoration whenever possible, even in older adults, given the increasing activity levels of this population.
Role of Arthroscopy
Arthroscopically-assisted reduction and internal fixation (ARIF) for intra-articular distal radius fractures is an established technique, allowing direct visualization of the articular surface, removal of incarcerated fragments, and assessment/repair of associated ligamentous injuries (e.g., TFCC, scapholunate ligament). While requiring specialized equipment and expertise, ARIF can lead to improved articular congruity and detection of otherwise missed soft tissue injuries. However, it is generally more technically demanding and may increase operative time compared to traditional ORIF.
Evidence-Based Guidelines
Professional organizations like the American Academy of Orthopaedic Surgeons (AAOS) provide clinical practice guidelines that highlight the evidence-based recommendations for the treatment of distal radius fractures. These guidelines generally support:
* Initial non-operative management for stable, minimally displaced fractures.
* Operative stabilization for unstable or significantly displaced fractures.
* The use of VLPs for operative management due to their biomechanical stability and facilitation of early rehabilitation.
* Careful consideration of patient factors, including age, activity level, and comorbidities, when selecting treatment.
In conclusion, the contemporary management of distal radius fractures emphasizes anatomical reduction and stable fixation to permit early mobilization, thereby optimizing functional recovery and minimizing long-term complications. The choice of technique remains a nuanced decision, integrating fracture characteristics, patient demands, and evidence-based principles.
You Might Also Like