Understanding Normal Bone Metabolism: Your Body's Blueprint
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Understanding Normal Bone Metabolism: Your Body's Blueprint. Normal bone metabolism is a dynamic process essential for skeletal health and mineral balance. It is primarily regulated by parathyroid hormone (PTH) and 1,25(OH)2D3, alongside calcitonin. These hormones homeostatically control serum calcium and phosphate levels by influencing intestinal absorption, reabsorption in the kidney, and bone remodeling to maintain proper body function.
-
Normal bone metabolism
□ Calcium - Helps prevent heterotopic ossification after THA in patients at high risk for this development
- Incidence of heterotopic ossification after THA among patients with Paget disease is approximately 50%.
- Important in muscle and nerve function, clotting, and many other areas
- More than 99% of the body’s calcium is stored in bones.
- Plasma calcium is about equally free and bound (usually to albumin).
- Approximately 400 mg of calcium is released from bone daily.
- Absorbed in the duodenum by active transport
- Requires ATP and calcium-binding protein
- Regulated by 1,25(OH)2D3
- Absorbed in the jejunum by passive diffusion
- Kidney reabsorbs 98% of calcium (60% in proximal tubule)
- Calcium may be excreted in stool.
-
Primary homeostatic regulators of serum calcium are PTH and 1,25(OH) 2 D 3
-
Dietary requirement for elemental calcium:
- Approximately 600 mg/day for children
- Approximately 1300 mg/day for adolescents and young adults (ages 10–25 years)
- 750 mg/day for adults ages 25–50 years
- 1200–1500 for adults over age 50 years
- 1500 mg/day for pregnant women
- 2000 mg/day for lactating women
- 1500 mg/day for postmenopausal women and for the patient with a healing fracture in a long bone
- Calcium balance is usually positive in the first three decades of life and negative after the fourth decade.
- Phosphate
- A key component of bone mineral
- Approximately 85% of the body’s phosphate stores are in bone.
- Plasma phosphate is mostly unbound.
- Also important in enzyme systems and molecular interactions as a metabolite and buffer
- Dietary intake of phosphate is usually adequate.
- Daily requirement is 1000–1500 mg.
- Reabsorbed by the kidney (proximal tubule)
- Phosphate may be excreted in urine.
- Parathyroid hormone
- An 84–amino acid peptide
- Synthesized in and secreted from chief cells of the (four) parathyroid glands
- N-terminal fragment 1-34 is the active portion.
-
Teriparatide, the synthetic form of recombinant human PTH, contains this active sequence.
- Used to treat some forms of osteoporosis
- Increased risk of osteosarcoma
-
Effect of PTH mediated by the cAMP second-messenger mechanism downstream in osteocytes
Table 1.12
Regulation of Calcium and Phosphate Metabolism Parameter
|
PTH (Peptide)
|
1,25(OH)2D (Steroid)
|
Calcitonin (Peptide)
| ---|---|---|---|
Origin
| Chief cells of parathyroid
| Proximal tubule
| Parafollicular cells
| glands
| of kidney
| of thyroid gland
| ---|---|---|---|
Factors stimulating production
| Decreased serum Ca2+
| Elevated PTH level
Decreased
serum Ca2+ level
Decreased
serum Pi
| Elevated serum Ca2+ level
Factors inhibiting production
| Elevated serum Ca2+ Elevated 1,25(OH)2D
| Decreased PTH
Elevated serum Ca2+
Elevated
serum Pi
| Decreased serum Ca2+
Effect on end-organs for hormone action:
| |
|
Intestine
| No direct effect Acts indirectly on
bowel by stimulating production of 1,25(OH)2D in
kidney
| Strongly
stimulates intestinal absorption of Ca2+ and Pi
| ?
Kidney
| Stimulates 25(OH)D 1α-hydroxylase in mitochondria of proximal tubular cells to convert 25(OH)D to
1,25(OH)2D
Increases fractional resorption of filtered Ca2+
Promotes urinary excretion of Pi
| ?
| ?
Bone
| Stimulates
osteoclastic resorption of bone
Stimulates
recruitment of preosteoclasts
| Strongly
stimulates osteoclastic resorption of bone
| Inhibits
osteoclastic resorption of bone
? Role in
normal human physiology
Net effect on Ca 2+
| Increased serum Ca2+
| Increased
| Decreased serum
and P i concentrations in extracellular fluid and serum
| level
Decreased serum Pi level
| serum Ca2+ level
Increased
| serum Pi level | Ca2+ level (transient) |
| --- | --- | --- | --- |
Adapted from Netter FH:
CIBA collection of medical illustrations, vol 8: Musculoskeletal system, part I: Anatomy, physiology and developmental disorders,
Basel, Switzerland, 1987, CIBA, p 179.
1. PTH helps regulate plasma calcium.
1. Decreased calcium levels in extracellular fluid stimulate β2
adrenoreceptors to release PTH, which acts at the intestines, kidneys, and bones (
Table
1.12).
6. PTH directly activates osteoblasts.
7. PTH modulates renal phosphate filtration.
8. PTH may accentuate bone loss in elderly persons.
9. PTH-related protein and its receptor have been implicated in metaphyseal dysplasia.
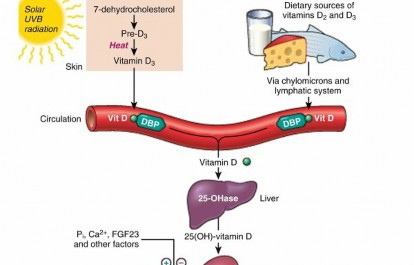
5. Vitamin D
1. Naturally occurring steroid
2.
Activated by ultraviolet radiation from sunlight or utilized from dietary intake (
Fig. 1.15)
3. Hydroxylated to 25(OH)D3 in the liver and hydroxylated a
second time in the kidney to one of the following:
1. 1,25(OH)2D3, the active hormone
2. 24,25(OH)2D3
, the inactive form (
Fig. 1.16)
4. 1,25(OH)2D3 works at the intestines, kidneys, and bones (see
Table 1.12).
5. Phenytoin (Dilantin) impairs metabolism of vitamin D.
6. Calcitonin
1. A 32–amino acid peptide hormone produced by clear cells in the parafollicles of the thyroid gland
2.
Limited role in calcium regulation (see
Table 1.12)
3. Increased extracellular calcium levels cause secretion of calcitonin.
1. Controlled by a β2 receptor
4. Inhibits osteoclastic bone resorption
1. Osteoclasts have calcitonin receptors.
2. Calcitonin decreases osteoclast number and activity.
5. Decreases serum calcium level
1. May also have a role in fracture healing and in reducing vertebral compression fractures in high-turnover osteoporosis
7. Other hormones affecting bone metabolism
1. Estrogen
1. Prevents bone loss by inhibiting bone resorption
1. Decrease in urinary pyridinoline cross-links
2. Because bone formation and resorption are coupled, estrogen therapy also decreases bone formation.
3. Supplementation is helpful in postmenopausal women only if started within 5–10 years after onset of menopause.
1. Risk of endometrial cancer is reduced when estrogen therapy is combined with cyclic progestin therapy.
4. Certain regimens of hormone replacement therapy may increase risks of heart disease and breast cancer.
5. Other postmenopausal pharmacologic interventions (alendronate, raloxifene) should be strongly considered.
2. Corticosteroids
1. Increase bone loss
1. Decrease gut
absorption of calcium by decreasing binding proteins
2. Decrease bone formation (cancellous more than cortical) by inhibiting collagen synthesis and osteoblast productivity
3. Thyroid hormones
1. Do not affect mineralization
2. Alternate-day therapy may reduce the effects.
1. Affect bone resorption more than bone formation
1. Large (thyroid-suppressive) doses of thyroxine can lead to osteoporosis.
2. Regulates skeletal growth at the physis
1. Stimulates chondrocyte growth, type X collagen synthesis, and alkaline phosphatase activity
2. Growth hormone
1. Causes positive calcium balance by increasing gut absorption of calcium more than it increases urinary excretion

 FIG. 1.15
Vitamin D metabolism.
DBP,
vitamin D–binding protein;
OHase,
1α-hydroxylase;
Pi,
inorganic phosphate.
FIG. 1.15
Vitamin D metabolism.
DBP,
vitamin D–binding protein;
OHase,
1α-hydroxylase;
Pi,
inorganic phosphate.
From Kumar V et al, editors:
Robbins and Cotran pathologic basis of disease
, Philadelphia, 2010, Saunders.
2. Insulin and somatomedins participate in this effect.
3. Growth factors
1. Transforming growth factor β (TGF-β), platelet-derived growth factor (PDGF), monokines, and lymphokines have roles in bone and cartilage repair.
1. Peak bone mass
1. Believed to occur between 16 and 25 years of age
2. Higher in men and in African Americans
3. After peak, bone loss occurs at a rate of 0.3%–0.5% per year
4. Rate of bone loss is 2%–3% per year in untreated women during the sixth through tenth years after menopause.
1. #### Affects trabecular more than cortical bone
1. Increase in trabecular rods results in increased anisotropy.

---
FIG. 1.16 Vitamin D metabolism in the renal tubular cell.
From Simon SR, editor:
Orthopaedic basic science,
Rosemont, IL, 1994, American Academy of Orthopaedic Surgeons, p 165.
2. Cortical bone becomes thinner and intracortical porosities increase.
3. Cortical bone becomes more brittle, less strong, and less stiff.
2. #### Long bones have greater inner and outer diameters.
2. Bone loss
1. Occurs at the onset of menopause when both bone formation and resorption are accelerated
1. A net negative change in calcium balance: menopause decreases intestinal absorption and increases urinary excretion of calcium.
2. #### Both urinary hydroxyproline and pyridinoline cross-links are elevated when bone resorption occurs.
3. #### Serum alkaline phosphatase level is elevated when bone formation is increased.
1.
Conditions of bone mineralization (
Tables
1.13
through
1.17)
1. Hypercalcemia
1. Can manifest in a number of ways
1. Polyuria, polydipsia, and nephrolithiasis
2. Excessive bony resorption with or without fibrotic tissue replacement (osteitis fibrosa cystica)
3. CNS effects (confusion, stupor, weakness)
4. GI effects (constipation)
2. Can also cause anorexia, nausea, vomiting, dehydration, and muscle weakness
3. Primary hyperparathyroidism
1. Overproduction of PTH usually a result of a parathyroid adenoma (surgical parathyroidectomy is curative)
1. Generally affects only one
parathyroid gland
2. Reflected in a net increase in plasma calcium and a decrease in plasma phosphate (as a result of enhanced urinary excretion)
3. #### Increased osteoclastic resorption and failure of repair attempts (poor mineralization as a result of low phosphate level)
4. Diagnosis:
1. Laboratory findings
1. Increased serum calcium, PTH, and urinary phosphate
2. Decreased serum phosphate
2. Bony changes
1. Osteopenia
2. Osteitis fibrosa cystica (fibrous replacement of marrow)
3. Brown tumors: increased giant cells, extravasation of RBCs, hemosiderin staining, fibrous tissue hemosiderin
4. Chondrocalcinosis
3. Radiographic findings
1. Deformed, osteopenic bones
2. Fractures
3. Shaggy trabeculae
4. Radiolucent areas (phalanges, distal clavicle, skull)
5. Destructive metaphyseal lesions
6. Calcification of soft tissues
4. Histologic changes
1. Osteoblasts and osteoclasts active on both sides of the trabeculae (as in Paget
4. Other causes of hypercalcemia
1. Familial syndromes
disease)
1. Areas of destruction
2. Wide osteoid seams
1. Pituitary adenomas associated with multiple endocrine neoplasia (MEN) types I and II
Table 1.13 Overview of Clinical and Radiographic Aspects of Metabol Disease Cause Clinical F Hypercalcemia
PTH Kidney sto
overproduction: hyperr
Hyperparathyroidism adenoma
PTH
overproduction: MEN/renal
Familial syndromes
Hypocalcemia
Hypoparathyroidism PTH Neuromus underproduction: irritabi idiopathic
Short MC
Renal abn
Bone defor
hypoto
Total bald
↓ Renal tubular
phosphate
dependent (types I and II) rickets Vitamin D– deficiency rickets Vitamin D–
See
Table 1.16
↓ Vitamin D diet; malabsorption
Rickets (osteomalacia)
Chronic renal failure: ↓ phosphate excretion
osteodystrophy Renal
PTH receptor abnormality
syndrome PHP/Albright
Bone defor
hypoto
Endocrine
abnorm
Vitamin D–resistant (hypophosphatemic) rickets
| resorption
| ---|---|---
Hypophosphatasia
| ↓ Alkaline
phosphatase
| Bone defor
hypoto
Osteopenia
Osteoporosis
| ↓ Estrogen: ↓ bone mass
| Kyphosis,
Scurvy
| Vitamin C
deficiency: defective collagen
| Fatigue, bl
effusio
Osteodensity
Paget disease of bon
|
e Osteoclastic
abnormality: ↑
bone turnover
| Deformitie
fractur
Osteopetrosis
| Osteoclastic abnormality: unclear
| Hepatospl
anemia
↓, Decreased; ↑, increased.
Table 1.14 Laboratory Findings and Clinical Data Regarding Patients Changes in Level or Concentra Disorder Serum Serum Alkalin Calcium Phosphatase Phosph Primary hyperparathyroidism ↑
None or ↓
None o
| |
| ---|---|---|---
Malignancy with bony metastases
| ↑
| None or ↑
| None o
Hyperthyroidism
| ↑
| None
| None
Vitamin D intoxication
| ↑
| None or ↑
| None o
↓, Decreased; ↑, increased.
Table 1.15 Laboratory Findings and Clinical Data Regarding Patients Changes in Level or Concentration --- Disorder Serum Serum Alka Calcium Phosphastase Phos Hypopara-thyroidism | ↓
| ↑
| Non Pseudohypoparathyroidism | ↓
| ↑
| Non Renal osteodystrophy (high-turnover bone disease resulting from renal disease [secondary hyperparathyroidism]) | ↓ or
none
| ↑↑↑
| ↑
| |
| ---|---|---|---
Renal osteodystrophy
| ↑ or
none
| None or ↑
| ↑
(low-turnover bone
| |
disease due to renal
| |
disease [aluminum
| |
toxicity])
| |
↓, Decreased; ↑, increased.
Table 1.16 Laboratory Findings and Clinical Data Regarding Patients Changes in Level or Concentration --- Disorder Serum Serum Alkaline PTH Calcium Phos phos Nutritional rickets: vitamin D deficiency | ↓ or
none
| ↓
| ↑
| ↑
| |
| |
| ---|---|---|---|---|
Nutritional rickets: calcium deficiency
| ↓ or
none
| ↓
| ↑
| ↑
Nutritional rickets: phosphate deficiency
| None
| ↓
| ↑
| None
Hereditary vitamin D–dependent rickets type I (pseudo–vitamin D deficiency)
| ↓
| ↓
| ↑
| ↑
Hereditary vitamin D–dependent rickets type II [hereditary resistance to 1,25(OH) 2D]
| ↓
| ↓
| ↑
| ↑ Hypophosphatemic rickets (also known as vitamin D–resistant rickets and phosphate diabetes; Albright syndrome is an example of a | None
| ↓↓↓
| ↑
| None
hypophosphatemic syndrome)
| |
| |
| ---|---|---|---|---|
Hypophosphatasia
| ↑
| ↑
| ↓↓↓
| None
↓, Decreased; ↑, increased;
phos,
phosphatase.
Table 1.17 Differential Diagnosis of Metabolic Bone Diseases Based Calcium Level --- Increased | Decreased Primary | Hypoparathyroidism Pseudohypoparathyr Renal osteodystrophy (high-turnover bo
disease) Nutritional rickets: vi
D deficiency Nutritional rickets: ca
deficiency Hereditary vitamin D
dependent rickets (types I and II)
Malignancy with bon metastasis
Malignancy without metastasis
Multiple myeloma Lymphoma Hyperthyroidism Vitamin D intoxicatio Sarcoidosis
Milk-alkali syndrome Severe generalized
immobilization
hyperparathyroidism Hyperthyroidism Vitamin D intoxication Malignancy without bony metastasis Malignancy with bony metastasis Multiple myeloma Lymphoma Sarcoidosis Milk-alkali syndrome Severe generalized immobilization Multiple endocrine neoplasias Addison disease Steroid administration Peptic ulcer disease Hypophosphatasia Pseudohypoparathyroidism Renal osteodystrophy Nutritional rickets: vitamin D deficiency Nutritional rickets: calcium deficiency Hereditary vitamin D– dependent rickets (types I and II)
1. Familial hypocalciuric hypercalcemia
1. Poor renal clearance of calcium
1. Malignancy (most common)
1. Can be life threatening; commonly associated with muscle weakness
2. Initial treatment should include hydration with normal saline (reverses dehydration).
3. Can occur in the absence of extensive bone metastasis
4. Most commonly results from release of systemic growth factors and cytokines that stimulate osteoclastic bone resorption at bony sites not involved in the tumor process (RANKL pathway)
5. PTH-related protein secretion (lung carcinoma)
6. Lytic bone metastases and lesions (e.g., multiple myeloma)
2. Hyperthyroidism
3. Vitamin D intoxication
4. Prolonged immobilization
5. Addison disease
6. Steroid administration
7. Peptic ulcer disease (milk-alkali syndrome)
8. Kidney disease
9. Sarcoidosis
10. Hypophosphatasia
1. Treatment of hypercalcemia
1. Hydration (saline diuresis)
2. Loop diuretics
3. Dialysis (for severe cases)
4. Mobilization (prevents further bone resorption)
5. Specific drugs (bisphosphonates, mithramycin, calcitonin, and gallium nitrate)
1.
Hypocalcemia (
Fig. 1.17)
1. Findings
1. Low plasma calcium
2. Results from low levels of PTH or vitamin D3
3. Neuromuscular irritability (tetany, seizures, Chvostek sign), cataracts, fungal nail infections, ECG changes (prolonged QT interval), and other signs and symptoms
1. Hypoparathyroidism
1. Reduced PTH level causes decrease in plasma calcium level and increase in plasma phosphate level
1. Urinary excretion not enhanced because of the lack of PTH
2. Common findings:
1. Fungal nail infections
2. Hair loss
3. Blotchy skin (pigment loss, vitiligo)
3. Skull radiographs may show basal ganglia calcification.
4. Iatrogenic hypoparathyroidism most commonly follows thyroidectomy.
2. Pseudohypoparathyroidism (PHP)
1. A rare genetic disorder caused by lack of effect of PTH on the target cells
2. PTH is normal or high.
3. PTH action is blocked by an abnormality at the receptor, by the cAMP system, or by a lack of required cofactors (e.g., Mg2+)
4. Defect in
GNAS
gene from mother
5. Albright hereditary osteodystrophy, a form of PHP
1. Short first, fourth, and fifth metacarpals (MCs) and metatarsals (MTs)
2. Brachydactyly

---
FIG. 1.17
Body’s reaction to hypocalcemia, with consequent resorption of bone. When calcium level falls, PTH is secreted, which releases calcium and Pi from bone. PTH increases renal reabsorption of calcium while inhibiting phosphate reabsorption. These actions in combination restore calcium concentration. If hypocalcemia persists, PTH stimulates renal production of 1,25(OH)2D3, which increases intestinal calcium absorption.
From Goldman L, Ausiello D, editors:
Cecil medicine,
ed 23, Philadelphia, 2008, Saunders Elsevier.
3. Exostoses
4. Obesity
5. Diminished intelligence
1. Pseudo-pseudohypoparathyroidism (pseudo-PHP)
1. Normocalcemic disorder that is phenotypically similar to PHP
2. However, response to PTH is normal.
3.
Renal osteodystrophy (
Fig. 1.18)
1. A spectrum of bone mineral metabolism disorders in chronic renal disease.
2. Due to impaired excretion, which compromises mineral homeostasis
3. Leads to abnormalities in bone mineral metabolism
4. High-turnover renal bone disease
1. Chronically elevated serum PTH level leads to
secondary hyperparathyroidism
(hyperplasia of parathyroid gland chief cells).
2. Factors contributing to sustained
PTH increase
and secondary hyperparathyroidism include:
1. #### Diminished renal phosphorus excretion; phosphorus retention promotes PTH secretion by three mechanisms:
•
Hyperphosphatemi lowers serum calcium, stimulating PTH.
-
Phosphorus impairs renal 1α-hydroxylase activity, impairing production of 1,25(OH) 2 D 3 .
-
Phosphorus retention may directly increase the synthesis of PTH.
- Hypocalcemia
- Impaired renal calcitriol [1,25(OH)2D3]
- Alterations in the control of PTH gene transcription secretion
- Skeletal resistance to the actions of PTH
- Low-turnover renal bone disease (adynamic lesion of bone and osteomalacia)
- Secondary hyperparathyroidism is not characteristic with this condition.
- Serum PTH level is normal or mildly elevated.
- Bone formation and turnover are reduced.
- Excess deposition of aluminum into bone (aluminum toxicity) negatively affects bone mineral metabolism.
- Impairs differentiation of precursor cells to osteoblasts
- Impairs proliferation of osteoblasts
- Impairs PTH release from the parathyroid gland
- Disrupts the mineralization process
- Adynamic lesion: accounts for the majority of cases of low-turnover bone disease in patients with chronic renal failure
- Osteomalacia: defects in mineralization of newly formed bone
- Radiographs may demonstrate a rugger jersey spine (vertebral bodies appear to have increased density in the upper and lower zones in a striated appearance, like that in childhood osteopetrosis) and soft tissue calcification.
-
β2-Microglobulin may accumulate
with long-term dialysis, leading to amyloidosis. -
Amyloidosis may be associated with carpal tunnel syndrome, arthropathy, and
pathologic fractures.

--- FIG. 1.18 Pathogenesis of bony changes in renal osteodystrophy. PTR, proximal tubule reabsorption.
From McPherson RA, Pincus MR, editors: Henry’s clinical diagnosis and management by laboratory methods, ed 21, Philadelphia, 2007, Saunders Elsevier. - In amyloidosis, Congo red stain causes tissue material to turn pink.
- Laboratory findings:
- Abnormal glomerular filtration rate (GFR)
- Increased alkaline phosphatase, blood urea nitrogen (BUN), and creatinine levels
- Decreased venous bicarbonate level
- Treatment directed at relieving the urologic obstruction or kidney disease
- Rickets (osteomalacia in adults; Box 1.1)
-
Failure of mineralization leading to changes in the physis in the zone of provisional calcification (increased width and disorientation) and bone (cortical thinning, bowing) B ox 1 . 1 C a u s es of R i c ket s a n d O s t eoma l a c i a
Nutritional Deficiency
Vitamin D deficiency
Dietary chelators (rare) of calcium Phytates
Oxalates (spinach) Phosphorus Deficiency (Unusual)
Abuse of antacids (which contain aluminum), which leads to severe dietary phosphate binding
Gastrointestinal Absorption Defects
Postgastrectomy (rare today)
Biliary disease (interference with absorption of fat-soluble vitamin D)
Enteric absorption defects Short bowel syndrome
Rapid transit (gluten-sensitive enteropathy) syndromes
Inflammatory bowel disease
Crohn disease Celiac disease
Renal Tubular Defects (Renal Phosphate Leak) - X-linked dominant hypophosphatemic vitamin D–resistant rickets or osteomalacia
- Classic Albright syndrome or Fanconi syndrome type I
- Fanconi syndrome type II
- Phosphaturia and glycosuria
- Fanconi syndrome type III
- Phosphaturia, glycosuria, aminoaciduria
- Vitamin D–dependent rickets (or osteomalacia) type I—a genetic or acquired deficiency of renal tubular 25(OH)D 1α-hydroxylase enzyme that prevents conversion of 25(OH)D to the active polar metabolite 1,25(OH)2D
-
Vitamin D–dependent rickets (or osteomalacia) type II—which
represents enteric end-organ insensitivity to 1,25(OH)D and is probably caused by an abnormality in the 1,25(OH)2D nuclear receptor) - Renal tubular acidosis
- Acquired: associated with many systemic diseases
- Genetic
- Debré–De Toni–Fanconi syndrome
- Lignac-Fanconi syndrome (cystinosis)
-
Lowe syndrome
Renal Osteodystrophy: Miscellaneous Causes Soft tissue tumors secreting
putative factors Fibrous dysplasia Neurofibromatosis
Other soft tissue and vascular mesenchymal tumors
Anticonvulsant medication (induction of the hepatic P450 microsomal enzyme system by some anticonvulsants—e.g., phenytoin, phenobarbital, and primidone [Mysoline]—causes increased degradation of vitamin D metabolites)
Heavy metal intoxication Hypophosphatasia
High-dose diphosphonates
Sodium fluoride
Adapted from Simon SR, editor: Orthopaedic basic science, ed 2, Rosemont, IL, 1994, American Academy of Orthopaedic Surgeons, p 169.
You Might Also Like

