Nonoperative Management Supracondylar: When it Works & How
Key Takeaway
This topic focuses on Nonoperative Management Supracondylar: When it Works & How, Nonoperative management supracondylar fractures is limited to nondisplaced (type I) fractures of the humerus with intact cortices and normal radiographic angles. It involves immobilizing the elbow in a splint or cast, flexed no more than 90 degrees. Clinicians must ensure distal radial pulse integrity and adequate perfusion, as increasing flexion risks brachial artery compression.
Nonoperative Management Supracondylar: When it Works & How
Introduction & Epidemiology
Supracondylar humerus fractures (SCHF) represent the most common elbow fracture in pediatric patients, accounting for approximately 60-70% of all elbow fractures in this population. These injuries typically occur in children aged 5-10 years, frequently resulting from a fall onto an outstretched hand with the elbow in hyperextension, leading to an extension-type fracture pattern (the vast majority). Flexion-type fractures, though less common, typically result from a direct blow to the posterior aspect of a flexed elbow. Given the proximity of critical neurovascular structures, SCHF carry a significant risk of complications, including neurovascular compromise, cubitus varus deformity, and Volkmann's ischemic contracture. Therefore, accurate diagnosis, appropriate classification, and judicious management are paramount to optimize functional outcomes and mitigate long-term sequelae. While operative intervention has become the mainstay for displaced fractures, nonoperative management remains a viable and often preferable option for carefully selected cases. This review will delineate the precise indications, techniques, and considerations for the nonoperative management of pediatric supracondylar humerus fractures.
Surgical Anatomy & Biomechanics
A thorough understanding of the pediatric distal humeral anatomy and its unique biomechanical properties is fundamental to both diagnosing and managing SCHF. The distal humerus features a relatively thin diaphysis above the broader, expanding metaphyseal region of the condyles. This inherent structural weakness, coupled with the laxity of pediatric ligaments, predisposes the elbow to fracture rather than dislocation in response to significant axial loads.
Key anatomical considerations include:
*
Ossification Centers:
The elbow's complex ossification sequence can mimic fracture patterns on radiographs. The order of appearance for ossification centers (CRITOE: Capitellum, Radial head, Internal/Medial epicondyle, Trochlea, Olecranon, External/Lateral epicondyle) is crucial for accurate interpretation of pediatric elbow radiographs. The capitellum is the first to ossify, typically around 1 year of age, providing a reliable landmark.
*
Cortical Thickness:
The anterior and posterior cortices of the distal humerus are critical for structural integrity. Disruption of these cortices, particularly the posterior, is indicative of displacement.
*
Anterior Humeral Line (AHL):
On a true lateral radiograph, a line drawn along the anterior cortex of the humeral shaft should ideally bisect the middle third of the capitellum. In a nondisplaced or minimally displaced extension-type SCHF, this line may pass through the anterior third of the capitellum, indicating subtle posterior displacement of the distal fragment relative to the shaft. While some anterior displacement of the AHL is acceptable for Type I fractures, significant anterior displacement (passing anterior to the capitellum) suggests extension malrotation or displacement.
*
Baumann's Angle (Humeral-Capitellar Angle):
This angle is formed by the intersection of a line drawn along the lateral humeral condylar physis and a line drawn along the longitudinal axis of the humeral shaft. It typically measures 69-78 degrees (average 72 degrees) and should be compared to the contralateral uninjured elbow. An increase in Baumann's angle (valgus angulation) suggests a medial column impaction or lateral column fracture, while a decrease (varus angulation) indicates lateral column impaction or medial column fracture, often leading to cubitus varus if uncorrected. For nonoperative management, maintenance of a near-normal Baumann's angle (typically within 5-10 degrees of the contralateral side) is a critical criterion.
*
Neurovascular Structures:
The brachial artery, median nerve, and radial nerve course immediately anterior and medial to the distal humerus. The ulnar nerve lies in the cubital tunnel posteriorly. Displacement of the fracture fragments, particularly posteromedial displacement, can directly impinge or lacerate these structures. Edema associated with the fracture can also lead to compartment syndrome, further compromising vascularity.
Biomechanical stability in Type I fractures relies on the intact periosteal sleeve and the inherent stability provided by the absence of significant displacement. These fractures typically have an intact posterior cortical hinge, which acts as a fulcrum for potential displacement. The goal of nonoperative management is to maintain this inherent stability until fracture union.
Indications & Contraindications
The indications for nonoperative management of supracondylar humerus fractures are strictly limited to nondisplaced or minimally displaced fractures, classically defined as Gartland Type I. The decision-making process hinges on meticulous clinical and radiographic evaluation to confirm the absence of significant displacement and neurovascular compromise.
Nonoperative Indications (Gartland Type I)
- Clinical Stability: No significant swelling or deformity. The limb is neurovascularly intact, with palpable distal pulses, normal capillary refill, and no motor or sensory deficits.
-
Radiographic Criteria:
- Nondisplaced Fracture Line: A visible fracture line is present without any discernible displacement of the distal fragment relative to the humeral shaft on both anteroposterior (AP) and lateral radiographs.
- Intact Anterior Humeral Line: The anterior humeral line drawn along the anterior cortex of the humerus should pass through the middle third of the capitellum. A minor deviation, where the line passes through the anterior third, may be acceptable if all other Type I criteria are met and there is no posterior cortical breach.
- Intact Posterior Cortex: Crucially, the posterior cortex must be completely intact, signifying an undisplaced fracture pattern. A "pucker sign" or visible breach of the posterior periosteum on the lateral radiograph often indicates Type II displacement requiring operative intervention.
- Normal Baumann's Angle: The Baumann's angle should be within 5-10 degrees of the contralateral, uninjured elbow, indicating no significant varus or valgus angulation.
- Intact Olecranon Fossa and Medial/Lateral Cortices: These structures should show no evidence of fracture or significant disruption, further confirming the nondisplaced nature.
- Absence of Fat Pad Signs as Sole Criterion: While the presence of anterior and posterior fat pad signs suggests an occult fracture (e.g., radial head or non-displaced SCHF), it is the presence of an actual fracture line meeting the above criteria that confirms SCHF for nonoperative management.
Contraindications for Nonoperative Management
Any fracture that does not strictly meet the criteria for a Gartland Type I fracture is generally considered a contraindication for nonoperative management and warrants operative intervention.
-
Displaced Fractures (Gartland Type II, III, IV):
- Type II: Posterior cortical hinge intact but anterior cortex disrupted with significant displacement.
- Type III: Complete displacement with no cortical contact.
- Type IV: Multidirectional instability after reduction (new classification by Wilkins).
- Neurovascular Compromise: Any evidence of vascular insufficiency (absent or diminished pulse, pallor, prolonged capillary refill, pulseless-pink hand) or nerve palsy (median, radial, or ulnar nerve deficits), even in Type I fractures, necessitates emergent evaluation and often operative intervention.
- Open Fractures: Presence of a skin breach communicating with the fracture site.
- Associated Injuries: Other significant injuries such as ipsilateral forearm fractures or elbow dislocations.
- Inability to Maintain Reduction: While primarily for Type II fractures, if a Type I fracture shows any signs of instability or impending displacement, it should be treated as a higher-grade injury.
- Compartment Syndrome: Clinical signs of acute compartment syndrome (pain out of proportion, pallor, paresthesia, pulselessness, paralysis) are an absolute contraindication and require emergent fasciotomy and likely fracture stabilization.
Operative vs. Non-Operative Indications
| Feature | Non-Operative Management (Gartland Type I) | Operative Management (Gartland Type II, III, IV, or Type I with Complications) |
|---|---|---|
| Fracture Displacement | Nondisplaced or minimally displaced | Displaced (anterior/posterior cortical disruption, complete offset) |
| Posterior Cortex | Intact posterior cortical hinge | Disrupted posterior cortex |
| Anterior Humeral Line | Bisects middle to anterior third of capitellum | Passes significantly anterior to capitellum or completely displaced |
| Baumann's Angle | Within 5-10 degrees of contralateral side | Significantly altered (e.g., >10-15 degrees difference from contralateral) |
| Neurovascular Status | Intact neurovascular examination (pulses, perfusion, sensation, motor) | Absent/diminished pulse, signs of ischemia, neurological deficits, impending compartment syndrome |
| Fracture Type | Gartland Type I (extension or flexion, but typically extension) | Gartland Type II, III, IV; Open fractures |
| Associated Injuries | None | Ipsilateral forearm fractures, elbow dislocations |
| Clinical Instability | Stable on clinical examination | Unstable, risk of loss of reduction |

Illustration of normal pediatric elbow anatomy and radiographic lines relevant to supracondylar fractures. Note the anterior humeral line passing through the capitellum and Baumann's angle for reference.
Pre-Operative Planning & Patient Positioning
While the focus of this topic is nonoperative management, "pre-operative planning" in this context refers to the comprehensive assessment and decision-making process that precedes any intervention, whether it be immobilization or surgery. For Type I fractures, this phase is critical to confirm suitability for nonoperative treatment and plan for appropriate follow-up. For cases deemed unsuitable for nonoperative care, this phase transitions into traditional surgical planning.
Pre-Treatment Planning for Nonoperative Cases
-
Clinical Assessment:
- Mechanism of Injury: Helps confirm extension vs. flexion type.
- Soft Tissue Evaluation: Assess for swelling, ecchymosis, skin compromise. Note any "pucker" sign anteriorly, which can indicate soft tissue interposition and potential instability, even in seemingly Type I fractures.
-
Neurovascular Examination:
This is paramount.
- Vascular: Palpate radial and ulnar pulses. Assess capillary refill time (<2 seconds). Evaluate for pallor or coolness. Document presence and quality of pulses (e.g., "2+ radial pulse").
- Neurological: Assess median (OK sign, thumb opposition), radial (thumb extension, wrist extension), and ulnar (finger abduction/adduction) nerve function. Test light touch sensation in respective dermatomes.
- Pain: Evaluate pain level and whether it is out of proportion to injury, which could suggest impending compartment syndrome.
-
Radiographic Evaluation:
- Standard Views: Obtain true AP and lateral radiographs of the elbow. Ensure the lateral view is a true lateral (superimposed humeral condyles) for accurate assessment of the anterior humeral line and fat pad signs.
- Contralateral Views: Consider obtaining comparative views of the uninjured elbow, particularly for assessing Baumann's angle and identifying subtle ossification patterns in younger children.
-
Critical Radiographic Analysis for Type I Confirmation:
- Evaluate the anterior humeral line. It should bisect the capitellum.
- Confirm an intact posterior cortical hinge.
- Measure Baumann's angle and compare to the contralateral side (if available).
- Rule out other fractures (e.g., radial head, lateral condyle).
- Fat Pad Signs: The presence of an anterior fat pad (sail sign) and especially a posterior fat pad indicates an intra-articular effusion, highly suggestive of an underlying fracture, even if a fracture line is not immediately apparent. In the absence of a visible fracture line, fat pad signs still warrant immobilization and follow-up radiographs to rule out occult fractures.
- Documentation: Thoroughly document all clinical and radiographic findings, including neurovascular status, fracture classification, and rationale for nonoperative management.
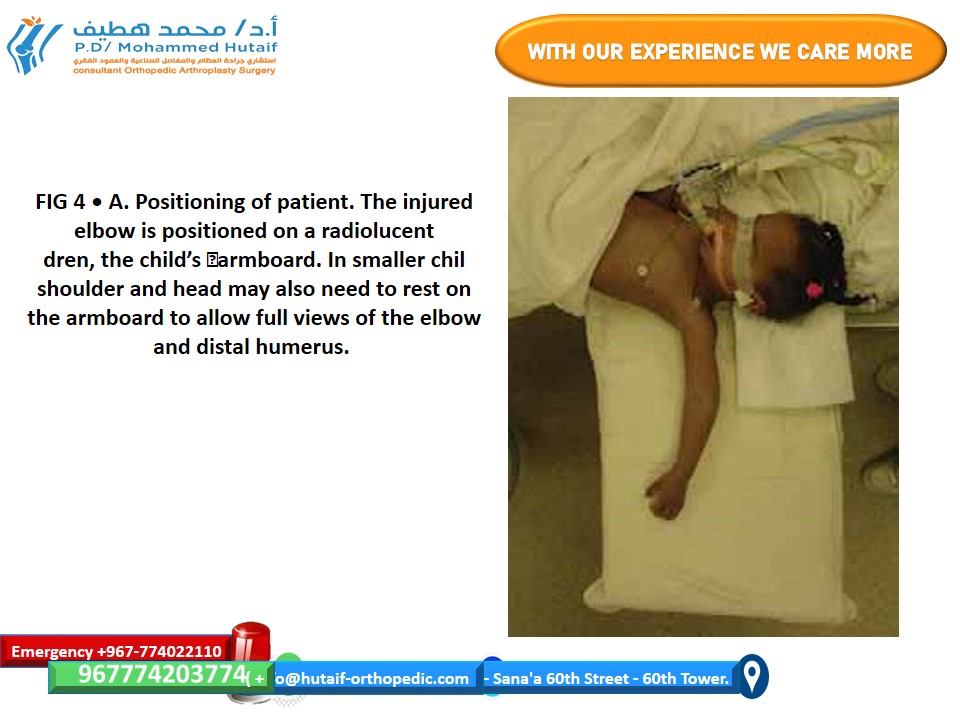
Patient Positioning for Nonoperative Management (Immobilization)
This is not a "surgical" positioning, but rather how the limb is positioned for effective splinting or casting.
*
Flexion Angle:
The elbow is typically immobilized in 70-90 degrees of flexion. This degree of flexion helps to "reduce" or maintain the reduction of the fracture fragments by relaxing the triceps and placing the fracture in a stable position. Exceeding 90 degrees of flexion can risk compressing the brachial artery, especially in the presence of swelling.
*
Forearm Rotation:
The forearm is usually placed in a neutral or slightly pronated position. This may vary slightly depending on the fracture pattern and surgeon preference, but pronation is often favored for extension-type fractures as it can help to stabilize the fracture by tightening the interosseous membrane and other soft tissues around the fracture site.
*
Gentle Handling:
Throughout the assessment and immobilization process, extreme care must be taken to avoid any undue manipulation or force that could displace a stable Type I fracture.
Detailed Nonoperative Management / Technique
The "technique" for nonoperative management of Gartland Type I supracondylar humerus fractures primarily involves proper immobilization and diligent monitoring. The goal is to provide sufficient stability for fracture healing while minimizing the risk of complications.
Step-by-Step Nonoperative Management
- Confirm Diagnosis and Classification: As outlined above, ensure the fracture unequivocally meets the criteria for a Gartland Type I. Any doubt about displacement or neurovascular status warrants re-evaluation and consideration for operative intervention.
- Neurovascular Re-assessment: Crucially, perform a complete neurovascular examination immediately prior to immobilization. Document all findings.
-
Closed Reduction (if necessary for minimally displaced Type I):
- While Type I fractures are by definition nondisplaced, some may have minimal displacement (e.g., slight posterior displacement of the capitellum relative to the AHL, but still an intact posterior cortex). In such cases, a gentle closed reduction maneuver may be performed prior to immobilization.
- This typically involves longitudinal traction with the elbow slightly flexed, followed by gentle flexion of the elbow to align the fragments.
- Self-correction: This is distinct from the aggressive reduction required for Type II or III fractures. For true Type I, significant reduction maneuvers are usually unnecessary and potentially harmful. The primary "reduction" is achieved simply by appropriate positioning for splinting.
-
Immobilization Technique:
- Material: A long-arm posterior splint, typically incorporating a sugar-tong component, is generally preferred acutely. This allows for some swelling accommodation. Once swelling subsides (usually 5-7 days), conversion to a long-arm cast may be considered, though continued splinting is often sufficient.
-
Position of Elbow Flexion:
Immobilize the elbow in approximately 70-90 degrees of flexion.
- Rationale: This position allows for optimal alignment of the fracture fragments, relaxation of the gastrocnemius-soleus complex, and mechanical stability. Excessive flexion (>90 degrees) can compress the brachial artery, leading to iatrogenic neurovascular compromise. Insufficient flexion (<70 degrees) may not provide adequate stability and could allow for redisplacement.
-
Forearm Rotation:
The forearm is typically placed in a neutral to slight pronation position.
- Rationale: For extension-type SCHF (the most common), pronation helps tighten the medial collateral ligament complex and periosteum, further stabilizing the fracture. It also reduces tension on the ulnar nerve.
- Padding: Ensure ample padding, especially over bony prominences (olecranon, epicondyles, radial head, ulnar styloid), to prevent pressure sores.
- Application: Apply the splint/cast snugly but not restrictively. There should be enough room to insert one finger between the cast/splint and the skin.
-
Post-Immobilization Neurovascular Re-assessment:
- Immediate Post-Application: Immediately after applying the splint/cast, perform another comprehensive neurovascular examination. Compare findings to the pre-immobilization assessment. This is a critical step.
- Documentation: Document the post-immobilization neurovascular status clearly. If there is any concern about diminished pulses, prolonged capillary refill, increased pain, or new neurological deficits, the splint/cast must be immediately removed, and the limb re-evaluated.
-
Radiographic Confirmation (if reduction performed):
- If any manipulative reduction was performed (even subtle for minimally displaced Type I), obtain post-immobilization AP and lateral radiographs to confirm acceptable alignment. This is less critical for truly nondisplaced Type I fractures where no manipulation occurred.
-
Patient/Parent Education (for ongoing monitoring):
-
Provide clear instructions regarding warning signs of neurovascular compromise (the "5 Ps"):
- Pain: Severe, increasing, out of proportion to injury, not relieved by analgesics.
- Pallor: Pale or white hand/fingers.
- Paresthesia: Numbness, tingling, loss of sensation.
- Paralysis: Inability to move fingers or wrist.
- Pulselessness: Absence of a palpable pulse.
- Instruct them to seek immediate medical attention if any of these signs develop.
- Advise on elevation of the limb to reduce swelling.
-
Provide clear instructions regarding warning signs of neurovascular compromise (the "5 Ps"):
-
Follow-up Schedule:
-
Initial Follow-up (3-7 days):
This is crucial to monitor for swelling resolution, reassess neurovascular status, and obtain repeat radiographs to check for any delayed displacement (loss of reduction) that can occur as swelling subsides.
-
 - Example of a follow-up radiograph for a pediatric supracondylar humerus fracture post-immobilization. Careful assessment of the anterior humeral line and Baumann's angle is critical to ensure maintenance of reduction.
-
- Subsequent Follow-up (2-3 weeks): Clinical and radiographic assessment to confirm continued healing and stability.
- Total Immobilization Duration: Typically 3-4 weeks for a Type I fracture.
-
Initial Follow-up (3-7 days):
This is crucial to monitor for swelling resolution, reassess neurovascular status, and obtain repeat radiographs to check for any delayed displacement (loss of reduction) that can occur as swelling subsides.
Historically: Traction Management
Historically, some displaced supracondylar fractures of the humerus, including certain Type II patterns, were managed with continuous traction (e.g., overhead Dunlop's traction or side-arm traction). This method aimed for gradual reduction and stabilization. However, with the advent of percutaneous pinning techniques, which offer comparable outcomes with shorter hospital stays, reduced nursing burden, and a lower incidence of traction-related complications, the use of traction has become exceedingly limited. It is now primarily reserved for highly specific situations, such as patients with significant soft tissue injury or swelling precluding immediate pinning, or in resource-limited settings. For Type I fractures, traction was never a primary management modality.
Complications & Management
While nonoperative management of Gartland Type I supracondylar humerus fractures is generally safe and effective, complications can arise, requiring vigilant monitoring and appropriate intervention. Complications can be broadly categorized as specific to the fracture or related to the immobilization.
Complications of Nonoperative Management
-
Loss of Reduction:
- Incidence: Relatively low in true Type I fractures, but can occur if initial classification was inaccurate or if excessive swelling subsides, leading to instability.
- Presentation: Increased pain, new deformity, or radiographic evidence of displacement (e.g., posterior cortical breach, altered Baumann's angle or anterior humeral line) on follow-up radiographs.
- Salvage Strategy: If loss of reduction is noted and the fracture becomes a Gartland Type II or III, conversion to operative management (closed reduction and percutaneous pinning) is indicated. Re-immobilization nonoperatively is generally not recommended for displaced fractures.
-
Neurovascular Compromise (Delayed):
- Incidence: Rare in Type I fractures initially, but can develop if swelling progresses within a restrictive cast or if the fracture displaces.
- Presentation: Worsening pain (especially pain out of proportion), paresthesia, pallor, pulselessness, or paralysis (the "5 Ps"). The most feared complication is Volkmann's Ischemic Contracture , resulting from prolonged ischemia leading to muscle necrosis and fibrosis.
-
Salvage Strategy:
- Immediate Cast/Splint Removal: If any signs of neurovascular compromise are present, the immobilization device must be immediately removed.
- Limb Repositioning: Gently extend the elbow slightly to relieve potential brachial artery compression, if possible without displacing the fracture.
- Re-assessment: Re-evaluate neurovascular status. If compromise persists, emergent consultation with orthopedic and vascular surgeons is warranted.
- Surgical Exploration/Fasciotomy: If a "pulseless-pink" hand (perfusion but no palpable pulse) or signs of compartment syndrome persist despite splint removal, surgical exploration of the brachial artery and/or fasciotomy may be required.
-
Stiffness/Limited Range of Motion:
- Incidence: Uncommon after Type I fractures managed nonoperatively, especially with appropriate duration of immobilization and early, gentle mobilization.
- Presentation: Persistent flexion contracture or extension deficit beyond the expected healing period.
- Salvage Strategy: Gentle active range of motion exercises initiated after immobilization. Avoidance of aggressive passive stretching. Rarely, physiotherapy or dynamic splinting might be indicated for persistent stiffness. Surgical intervention for stiffness (e.g., capsular release) is exceedingly rare for Type I nonoperative management.
-
Malunion (Cubitus Varus/Valgus):
- Incidence: Very rare in true Type I fractures, as there is no initial displacement. It usually results from a missed or undertreated subtle displacement (e.g., a Type II initially misdiagnosed as Type I, or loss of reduction that went unnoticed).
- Presentation: Visible elbow deformity, often with altered carrying angle (cubitus varus being more common for extension-type SCHF).
- Salvage Strategy: For mild cosmetic deformity, observation is usually sufficient. Severe cubitus varus can sometimes be associated with late ulnar nerve palsy or posterolateral rotatory instability and may require corrective osteotomy (e.g., lateral closing wedge osteotomy) once the child reaches skeletal maturity or if symptoms arise.
Complications of Surgical Management (Briefly, for Context)
While beyond the primary scope of nonoperative care, it's crucial for the academic surgeon to be aware of operative risks when comparing management strategies.
*
Iatrogenic Nerve Injury:
Ulnar nerve (with medial pins), radial nerve (with lateral pins).
*
Pin Site Infection:
Localized infection at the pin entry sites.
*
Loss of Fixation/Pin Migration:
Pins bending, breaking, or backing out.
*
Vascular Injury:
Direct injury to the brachial artery during pinning or reduction.
*
Compartment Syndrome:
Can still occur post-operatively.
*
Stiffness/Heterotopic Ossification:
Less common but can occur.
Markdown TABLE: Common Complications and Management Strategies
| Complication | Incidence (Gartland Type I Nonoperative) | Presentation | Salvage Strategy |
|---|---|---|---|
| Loss of Reduction | Low (<5%) | Increased pain, new deformity, radiographic displacement | Convert to operative management (CRPP) |
| Neurovascular Compromise | Very Low (<1%) | Worsening pain, pallor, paresthesia, pulselessness, paralysis | Immediate splint/cast removal, re-assessment; potentially surgical exploration/fasciotomy |
| Stiffness | Low | Persistent limited ROM beyond expected healing | Gentle AROM; avoid PROM; physiotherapy if needed (rarely surgical) |
| Malunion (Cubitus Varus) | Very Low | Altered carrying angle, visible deformity | Observation for mild; corrective osteotomy for severe symptomatic deformity (late) |
| Pressure Sores | Low | Skin breakdown under cast/splint | Proper padding, immediate cast change; local wound care |
Post-Operative Rehabilitation Protocols (Nonoperative)
For nonoperatively managed Gartland Type I supracondylar humerus fractures, the "post-operative" phase refers to the period following immobilization, focused on restoring pain-free range of motion and function. The rehabilitation protocol is typically straightforward and aims to avoid aggressive interventions that could lead to complications.
-
Immobilization Period (3-4 weeks):
- Maintain the splint or cast for an average of 3-4 weeks. The exact duration may vary based on the child's age, perceived stability, and radiographic evidence of early callus formation.
- During this period, active range of motion of the shoulder, wrist, and hand should be encouraged to prevent stiffness in adjacent joints.
-
Splint/Cast Removal (3-4 weeks post-injury):
- Radiographic assessment at the time of removal should confirm early union.
- After removal, the elbow will likely exhibit some stiffness and mild discomfort.
-
Initiation of Gentle Active Range of Motion (AROM):
- The cornerstone of rehabilitation is active, pain-free range of motion .
- The child should be encouraged to use the arm normally for daily activities.
- Simple exercises include gentle flexion, extension, pronation, and supination, guided by comfort. "Gravity-assisted" exercises can be helpful (e.g., dangling arm while leaning forward).
- Crucially, passive range of motion (PROM) or aggressive stretching is strictly contraindicated. Forced manipulation can lead to pain, swelling, re-fracture, or stimulate heterotopic ossification, prolonging recovery or creating permanent deficits.
-
Weight-Bearing Restrictions:
- Avoid heavy lifting or carrying for another 2-4 weeks after cast removal, depending on the radiographic evidence of consolidation.
-
Return to Activity:
- Light, non-contact sports may be gradually introduced after 6-8 weeks, once full pain-free range of motion is achieved and radiographic union is evident.
- Contact sports and activities involving high impact or risk of re-injury (e.g., gymnastics, football) are typically restricted for 8-12 weeks, or until complete radiographic union and full strength are restored.
-
Monitoring:
- Continue to monitor for pain, swelling, and progress in range of motion.
- Persistent stiffness or pain warrants further evaluation.
- Most children achieve excellent or good functional outcomes with full or nearly full range of motion.
Summary of Key Literature / Guidelines
The management of pediatric supracondylar humerus fractures is guided by a robust body of literature, with the Gartland classification system serving as the universally accepted standard for guiding treatment decisions.
-
Gartland Classification (1959, modified by Wilkins):
This system remains the cornerstone.
- Type I: Nondisplaced. All cortical margins are intact, and the anterior humeral line passes through the middle third of the capitellum. These fractures are inherently stable.
- Type II: Displaced with an intact posterior cortical hinge. The anterior humeral line is displaced anterior to the capitellum.
- Type III: Completely displaced. No cortical contact between proximal and distal fragments.
- Type IV (Wilkins modification): Multidirectional instability (rare).
-
Evidence for Nonoperative Management:
- Numerous studies and consensus guidelines consistently support nonoperative management for Gartland Type I supracondylar humerus fractures. Immobilization in a long-arm cast or splint at 70-90 degrees of flexion with the forearm in neutral or pronation is the standard of care.
- Outcomes are overwhelmingly positive, with high rates of union, excellent functional range of motion, and a very low incidence of complications when managed appropriately.
- A critical review of the literature emphasizes the importance of meticulous neurovascular assessment before, during, and after immobilization.
- Shift Away from Traction: Historical methods involving overhead or side-arm traction for displaced fractures have largely been supplanted by closed reduction and percutaneous pinning (CRPP). This shift reflects the improved safety, efficiency, and comparable efficacy of CRPP, particularly for Type II and III fractures. Nonoperative management for Type I fractures, however, has consistently been the gold standard, not requiring traction.
- Role of Radiographic Parameters: The anterior humeral line and Baumann's angle are indispensable diagnostic and monitoring tools. The literature reinforces that maintaining these parameters within acceptable limits (as defined for Type I) is crucial for successful nonoperative outcomes. Persistent abnormal angles or displacement warrant consideration for operative intervention.
- Importance of Vigilant Follow-up: Consensus emphasizes the need for early follow-up (3-7 days post-injury) with repeat radiographs to detect any delayed loss of reduction as swelling subsides. This proactive approach helps prevent malunion and facilitates timely intervention if conversion to operative management becomes necessary.
- Avoiding Aggressive Rehabilitation: The literature strongly advises against passive manipulation or forced stretching during the rehabilitation phase for pediatric elbow fractures, especially supracondylar fractures, due to the risk of re-injury, heterotopic ossification, and prolonged stiffness. Active, gentle range of motion is the preferred and most effective strategy.
In conclusion, the nonoperative management of Gartland Type I supracondylar humerus fractures remains a highly effective and safe treatment strategy. Success hinges upon accurate initial diagnosis, strict adherence to immobilization principles, meticulous neurovascular monitoring, and appropriate post-immobilization rehabilitation. Any deviation from Type I criteria or the development of complications mandates prompt re-evaluation and consideration for operative intervention.
You Might Also Like

