Screw Fixation: Prevent Displacement in Greater Tuberosity Nondisplaced Fractures

Key Takeaway
Learn more about Screw Fixation: Prevent Displacement in Greater Tuberosity Nondisplaced Fractures and how to manage it. Greater tuberosity nondisplaced fractures are treated to prevent displacement, which rotator cuff pull can cause, leading to impingement and pain. Management typically involves minimally invasive screw fixation, using K-wires for temporary stabilization and cannulated lag screws for definitive osteosynthesis. Post-operative care includes early passive motion, tailored to the patient and repair quality.
Introduction & Epidemiology
Greater tuberosity (GT) fractures of the proximal humerus represent a distinct injury pattern, accounting for approximately 15-20% of all proximal humeral fractures. While often associated with anterior shoulder dislocations (occurring in 20-30% of such dislocations), isolated GT fractures can also result from a fall onto an outstretched arm or direct trauma to the shoulder. These injuries are particularly significant due to the critical anatomical role of the greater tuberosity as the insertion site for the supraspinatus and infraspinatus tendons, integral components of the rotator cuff.
The focus of this discourse is on two-part, extraarticular greater tuberosity fractures that are initially classified as "nondisplaced" or "minimally displaced" (e.g., Neer Type 1, AO/OTA 11-A1.1). Despite their initial radiographic appearance, these fractures carry a recognized risk of secondary displacement during the crucial early post-injury period, typically within the first one to two weeks. This phenomenon is largely attributed to the unopposed tensile forces exerted by the musculotendinous units of the rotator cuff, specifically the superior and posterior pull of the supraspinatus and infraspinatus, respectively.
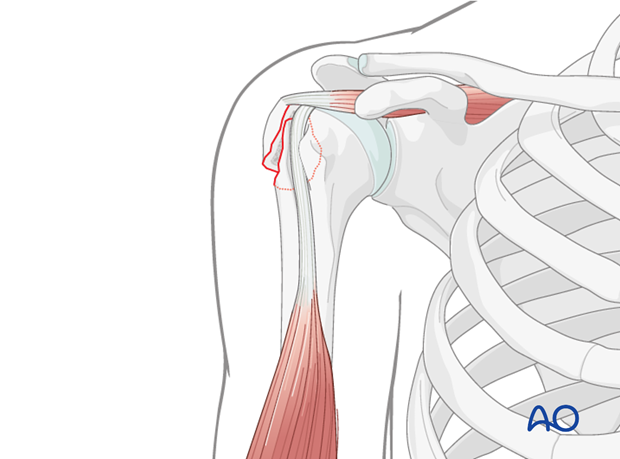
Unrecognized or untreated secondary displacement of the greater tuberosity fragment, particularly superiorly and posteriorly, can lead to significant clinical sequelae. A malunited or nonunited greater tuberosity in a displaced position can impinge upon the coracoacromial arch, leading to subacromial impingement syndrome, pain, and restricted glenohumeral motion, particularly during abduction and external rotation. This chronic impingement can further compromise rotator cuff function and potentially lead to degenerative changes within the subacromial space. Therefore, the decision-making process for these seemingly benign fractures must carefully weigh the risk of secondary displacement against the benefits and potential complications of prophylactic internal fixation. The objective of surgical intervention, when indicated, is to prevent displacement, restore anatomical alignment, and facilitate early, protected motion to optimize functional recovery and prevent long-term disability.
Surgical Anatomy & Biomechanics
Surgical Anatomy
The greater tuberosity is a prominent posterolateral eminence of the proximal humerus, serving as the primary insertion site for the supraspinatus, infraspinatus, and teres minor tendons of the rotator cuff. Understanding its intricate anatomy and surrounding neurovascular structures is paramount for safe and effective surgical intervention.
- Greater Tuberosity Morphology: The GT is divided into superior, middle, and inferior facets. The supraspinatus tendon inserts primarily onto the superior facet, while the infraspinatus tendon inserts onto the middle facet. The teres minor, though less frequently involved in isolated GT fractures, inserts onto the inferior facet. The specific location and size of the fracture fragment are critical, as larger fragments carrying significant portions of the rotator cuff insertions are more susceptible to displacement. The anterior aspect of the GT is continuous with the bicipital groove, which houses the long head of the biceps tendon.
- Rotator Cuff Attachments: The tendinous insertions create strong traction forces on the GT fragment. The supraspinatus acts as a primary abductor, pulling the fragment superiorly. The infraspinatus, a powerful external rotator, exerts a posterior and superior vector. The collective action of these muscles, particularly in an active patient, can readily displace an unstable GT fracture.
-
Neurovascular Structures:
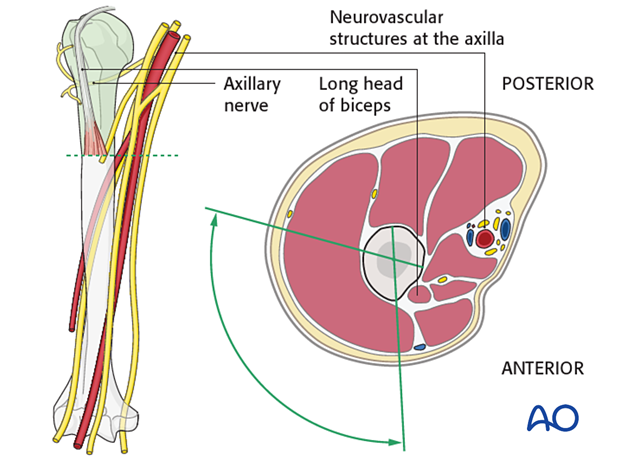
- Axillary Nerve: This nerve (C5, C6) is the most critical structure at risk during proximal humerus surgery. It courses from the quadrangular space, wrapping around the surgical neck of the humerus, typically 5-7 cm distal to the acromion. It innervates the deltoid and teres minor muscles and provides sensory supply to the regimental badge area. Injury to the axillary nerve can lead to deltoid paralysis and significant functional impairment. Surgical approaches involving deltoid splitting must respect this anatomical constraint, usually limiting the split to no more than 5 cm from the acromial edge.
- Musculocutaneous Nerve: Originating from the lateral cord of the brachial plexus (C5-C7), this nerve innervates the biceps brachii, coracobrachialis, and brachialis. It becomes superficial near the elbow. Proximally, it supplies the coracobrachialis, which can be encountered in a deltopectoral approach.
- Cephalic Vein: This large superficial vein runs in the deltopectoral groove and is a key landmark in the deltopectoral approach. It must be identified and protected, or ligated if necessary, to prevent significant hemorrhage.
- Anterior and Posterior Circumflex Humeral Arteries: These vessels, branches of the axillary artery, encircle the surgical neck of the humerus. The anterior circumflex humeral artery runs deep to the long head of the biceps tendon, while the posterior circumflex humeral artery accompanies the axillary nerve through the quadrangular space. Injury to these vessels can lead to significant bleeding.
-
Biomechanics
The biomechanical environment of a greater tuberosity fracture is dominated by the forces exerted by the rotator cuff.
- Displacement Vectors: As previously noted, the supraspinatus pulls the fragment superiorly, while the infraspinatus contributes a posterior and superior vector. In the context of a nondisplaced fracture, these forces act as ongoing deforming forces that can propagate an initially stable fracture into a displaced one. The magnitude of these forces is significant, especially during active shoulder motion, highlighting the need for stable fixation if operative management is chosen.
- Fracture Stability: The stability of the fracture fragment is influenced by its size, the degree of comminution, and the integrity of the remaining soft tissue attachments. A smaller, more comminuted fragment with compromised soft tissue attachments is inherently less stable and more prone to displacement.
- Impingement: A GT fragment that heals in a displaced position, particularly with superior displacement of >5 mm to 1 cm, can directly impinge against the undersurface of the acromion and the coracoacromial ligament during arm elevation and rotation. This mechanical impingement can restrict glenohumeral motion, cause pain, and lead to secondary rotator cuff pathology or bursitis. The objective of fixation is to restore the normal anatomical relationship of the greater tuberosity to the humeral head and the subacromial space, thereby preserving pain-free motion.
- Screw Fixation Biomechanics: The aim of screw fixation is to provide interfragmentary compression and rotational stability. Cannulated screws, often partially threaded, are typically inserted from the lateral cortex of the GT, traversing into the dense cancellous bone of the humeral head. For optimal purchase and stability, two screws are generally preferred, inserted with divergent or parallel trajectories. This construct resists the shear and tensile forces exerted by the rotator cuff, providing a stable environment for bone healing. In osteoporotic bone, screw pullout strength can be a concern, necessitating careful consideration of screw type, length, and trajectory, sometimes complemented by suture augmentation.
Indications & Contraindications
The decision for operative versus non-operative management of a nondisplaced greater tuberosity fracture hinges on a careful assessment of the fracture characteristics, patient factors, and the potential for secondary displacement and its clinical consequences.
Operative Indications (for initially Nondisplaced/Minimally Displaced GT Fractures at Risk of Secondary Displacement)
While the definition of "nondisplaced" often implies conservative management, specific scenarios warrant prophylactic surgical stabilization to prevent secondary displacement and optimize outcomes:
-
Risk of Secondary Displacement:
- Fragment size: Typically, fragments greater than 1 cm in size, especially if they involve a significant portion of the supraspinatus or infraspinatus insertion, are considered at higher risk.
- Associated rotator cuff tear: If an underlying rotator cuff tear (e.g., supraspinatus) is identified, even a minimally displaced GT fracture may benefit from fixation during the cuff repair to ensure optimal healing of both.
- Significant comminution around the base of the GT fragment, compromising stability.
- Radiographic evidence of subtle instability or impending displacement on stress views or dynamic imaging.
-
Patient Factors:
- Young, active, and high-demand individuals who require excellent shoulder function and are less tolerant of potential malunion or impingement.
- Athletes or laborers needing to return to specific overhead activities.
- Patients with poor compliance anticipated for strict non-operative rehabilitation protocols.
-
Associated Injuries Requiring Surgery:
- Concomitant shoulder instability (e.g., anterior dislocation) requiring surgical stabilization (e.g., Bankart repair), where the GT fracture can be addressed concurrently.
- Other concomitant proximal humerus fractures requiring open reduction and internal fixation (ORIF).
- Arthroscopic visualization confirming instability or potential for displacement of the fragment, or revealing articular involvement not evident on conventional imaging.
-
Failed Non-Operative Management:
- Documented secondary displacement of the fragment during the initial post-injury observation period despite appropriate non-operative management.
Non-Operative Indications
-
Truly Stable, Minimally Displaced Fractures:
- Fragments less than 5 mm displacement, with no evidence of significant rotator cuff traction and no demonstrable instability on stress radiographs.
- Smaller fragments (e.g., avulsion fractures) that are unlikely to displace further.
-
Patient Factors:
- Elderly, low-demand patients with significant medical comorbidities precluding surgical intervention.
- Patients who accept the potential risks of malunion or nonunion with conservative management, provided it is minimal.
- Patients with poor bone quality (severe osteoporosis) where surgical fixation may be tenuous and carry a high risk of hardware failure.
-
Contraindications for Surgery (Relative or Absolute):
- Active infection in the shoulder region.
- Severe medical comorbidities that pose an unacceptably high anesthetic or surgical risk (e.g., unstable cardiac disease, severe coagulopathy).
- Extremely poor bone quality where adequate screw purchase cannot be achieved, making fixation futile.
- Non-compliance with post-operative rehabilitation.
Table of Indications
| Feature | Operative Management | Non-Operative Management |
|---|---|---|
| Fracture Displacement | Initially nondisplaced, but with high risk of secondary displacement (e.g., fragment >1 cm, strong rotator cuff pull). Secondary displacement observed during conservative trial. | Truly nondisplaced/minimally displaced (<5mm), stable fragment. |
| Fragment Characteristics | Large fragment size, significant comminution compromising stability, involvement of critical rotator cuff insertion (e.g., supraspinatus footprint). | Small, non-comminuted fragment. |
| Associated Injuries | Concomitant rotator cuff tear (requiring repair), shoulder instability (requiring stabilization), other proximal humerus fractures. | Isolated GT fracture without significant associated soft tissue injury or instability requiring surgery. |
| Patient Demands | Young, active, high-demand individuals; athletes; laborers requiring optimal function and return to specific activities. | Elderly, low-demand individuals; sedentary lifestyle; patients with medical comorbidities precluding surgery. |
| Bone Quality | Adequate bone quality for stable hardware purchase. | Severe osteoporosis or osteopenia where fixation would be unstable, high risk of pullout. |
| Compliance | Expected good compliance with post-operative rehabilitation. | Poor compliance anticipated for rehabilitation; patient preference for non-operative management after informed consent. |
| Risk Tolerance | Low tolerance for potential malunion, impingement, pain, or functional deficit. | High tolerance for potential malunion (if minimal), or complications of surgery outweigh benefits. |
| Imaging | CT scan shows subtle instability, large fragment. MRI confirms rotator cuff pathology. Intra-operative arthroscopy reveals instability or articular involvement. | Radiographs/CT confirm stable, truly nondisplaced fracture without significant soft tissue compromise. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial to anticipate potential challenges and ensure optimal surgical outcomes.
Pre-Operative Planning
-
Imaging Review:
- Plain Radiographs: Standard AP, scapular Y, and axillary lateral views are essential. Special views, such as internal/external rotation views or Velpeau/trauma axillary views, can help better characterize displacement and comminution.
- Computed Tomography (CT) Scan: A CT scan, especially with 3D reconstructions, is invaluable. It provides detailed information regarding fracture morphology, comminution, fragment size, degree of displacement, articular involvement (if any, though less common in pure GT fractures), and bone loss. This helps in determining screw trajectories and the overall fixation strategy.
- Magnetic Resonance Imaging (MRI): While not routinely required for isolated GT fractures, an MRI can be beneficial if there is suspicion of associated rotator cuff tears (e.g., full-thickness supraspinatus tear), significant tendinopathy, or other soft tissue injuries that might influence management or require concurrent repair.
-
Surgical Strategy:
- Approach Selection: The choice between a minimally invasive percutaneous approach (often for screw fixation alone) or an open deltopectoral approach depends on the need for direct visualization, ease of reduction, and the presence of associated injuries (e.g., rotator cuff repair). For isolated, nondisplaced fractures at risk of secondary displacement, a minimally invasive technique with percutaneous screw fixation under fluoroscopic guidance is often preferred.
- Fixation Choice: Cannulated screws (typically 3.5mm or 4.0mm partially threaded) are commonly used due to their ease of insertion over a guidewire and ability to achieve interfragmentary compression. The number of screws (usually two for rotational stability) and their trajectory are determined by fragment size, bone quality, and desired construct stability. Suture augmentation may be considered, especially in osteoporotic bone or when there's an associated rotator cuff repair.
- Hardware Sizing: Pre-operative templating based on CT scans can help estimate screw lengths and diameters, though definitive sizing occurs intraoperatively.
- Anesthesia: General anesthesia is standard. An interscalene brachial plexus block can be a valuable adjunct for both intraoperative pain control and post-operative analgesia, facilitating earlier rehabilitation.
Patient Positioning
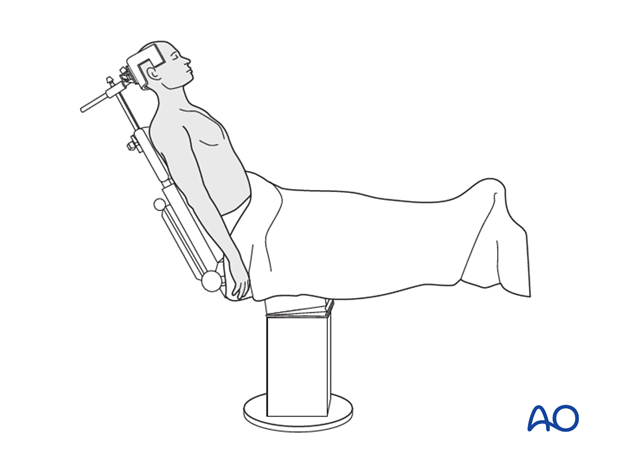
The beach chair position is the most commonly employed patient position for shoulder arthroscopy and open proximal humerus fracture fixation due to several advantages:
-
Setup:
- The patient is placed in a semi-recumbent position, typically with the head elevated 30-70 degrees relative to the torso.
- The head is secured in a headrest (e.g., Mayfield or equivalent) to prevent movement and protect cervical spine alignment, especially if an interscalene block has been administered.
- The torso is supported by a backrest, and the buttocks are positioned near the break in the operating table to allow for adjustable back flexion.
- The operative arm is draped free, often supported by a sterile arm holder or bolster, allowing full range of motion intraoperatively for fluoroscopic views and assessment of reduction.
- Ensure padding of all pressure points (heels, sacrum, occiput, ulnar nerves) to prevent nerve palsies or skin breakdown.
-
-
Advantages:
- Improved Exposure: Gravity assists in caudal displacement of the humerus, optimizing visualization of the GT.
- Fluoroscopic Access: Facilitates intraoperative fluoroscopy in multiple planes (AP, lateral, axillary).
- Simultaneous Arthroscopy: Allows for concurrent arthroscopic evaluation of the glenohumeral joint and subacromial space, which can be useful for assessing articular involvement, associated soft tissue injuries, or confirming reduction.
- Physiological Position: More comfortable for the patient post-operatively.
-
Disadvantages/Precautions:
- Hypotension: The semi-recumbent position can lead to significant drops in blood pressure due to gravitational pooling of blood in the lower extremities. This mandates careful anesthetic management, fluid resuscitation, and monitoring of cerebral perfusion, particularly in elderly or vasculopathic patients.
- Cerebral Hypoperfusion: The height difference between the heart and brain necessitates careful blood pressure management to ensure adequate cerebral perfusion pressure.
- Air Embolism: Though rare, the potential for venous air embolism exists, especially with an open incision above heart level.
- Cervical Spine Issues: Careful attention to neck position is vital to avoid traction or compression neuropathies.
Safe Zones for Screw Insertion
Understanding the neurovascular safe zones is critical for percutaneous screw insertion to minimize iatrogenic injury. These zones define areas where instrumentation can be safely introduced without damaging vital structures.
*
Anterior Deltoid:
The anterior deltoid can be split longitudinally, usually no more than 5 cm from the acromion, to avoid injury to the axillary nerve. This split allows for access to the anterior aspect of the GT.
*
Lateral Deltoid:
Percutaneous screw insertion from the lateral aspect of the greater tuberosity typically traverses the lateral deltoid. It is imperative to stay superior to the course of the axillary nerve, which generally runs 5-7 cm distal to the acromion. A limited deltoid split or blunt dissection can be used.
*
Posterior Deltoid:
Less commonly used for GT fractures, but similar precautions regarding the axillary nerve apply.
Fluoroscopic guidance is non-negotiable for percutaneous screw placement, allowing for real-time visualization of instrumentation trajectory relative to bony landmarks and helping to avoid articular penetration and minimize soft tissue dissection.
Detailed Surgical Approach / Technique
The goal of screw fixation for a nondisplaced greater tuberosity fracture, particularly an extraarticular two-part fracture at risk of displacement (AO/OTA 11-A1.1), is to prevent secondary displacement, maintain anatomical reduction, and facilitate early, protected motion. The approach is typically minimally invasive, leveraging percutaneous techniques under fluoroscopic guidance.
1. Patient Preparation and Positioning
-
Beach Chair Position:
As described in the pre-operative planning section, the patient is positioned in a beach chair, with the head securely fixed and the operative arm draped free. This setup allows full mobility of the arm and optimal fluoroscopic access.
 - Sterile Field: The entire shoulder, upper arm, and axilla are prepped and draped to allow for wide exposure and unhindered movement of the C-arm.
2. Surgical Incision and Exposure
- Minimally Invasive Percutaneous Approach: For an isolated, nondisplaced GT fracture, a minimally invasive approach is usually sufficient. This typically involves one or two small skin incisions (approximately 1-2 cm) directly over the planned entry points for the guidewires and screws on the lateral aspect of the greater tuberosity.
- Deltoid-Splitting (Limited): The skin incision is made, and then a limited, blunt deltoid-splitting approach is performed. Care must be taken to stay within the "safe zone" for the axillary nerve, typically not extending more than 5 cm distally from the lateral acromial edge. Blunt dissection minimizes muscle trauma and preserves nerve structures.
- Open Deltopectoral Approach (If necessary): If significant soft tissue stripping is needed for reduction, or if there are associated injuries requiring a more extensive exposure (e.g., large rotator cuff tear, complex comminution, failed closed reduction), a standard deltopectoral approach may be utilized. This involves an incision along the deltopectoral groove, identifying and protecting the cephalic vein, and developing the interval between the deltoid and pectoralis major. While providing excellent visualization, it is more invasive and generally reserved for more complex scenarios.
3. Fracture Reduction and Temporary Fixation
- Confirmation of Reduction: Even in initially nondisplaced fractures, it is crucial to confirm anatomical reduction under fluoroscopy. The greater tuberosity fragment must be flush with the humeral head articular surface and the adjacent cortical bone. Rotator cuff traction can cause subtle gapping or malrotation.
- Gentle Manipulation: If minor displacement is noted, gentle manipulation can be achieved using a periosteal elevator or a K-wire as a joystick. The arm position may be adjusted (e.g., abduction, external rotation) to relax the rotator cuff and facilitate reduction.
-
Temporary K-wire Fixation:
Once anatomical reduction is confirmed, one or more K-wires (e.g., 1.6 mm or 2.0 mm) are inserted to temporarily stabilize the fragment.
- Placement: The K-wires are typically inserted from the lateral aspect of the greater tuberosity, traversing the fragment and engaging the dense cancellous bone of the humeral head.
-
Trajectory:
Ensure the K-wires are placed so that they provide stability without impinging on the planned trajectory of the definitive screws or violating the articular surface. Fluoroscopic confirmation in AP, lateral, and axillary views is essential to verify correct K-wire placement and articular clearance.
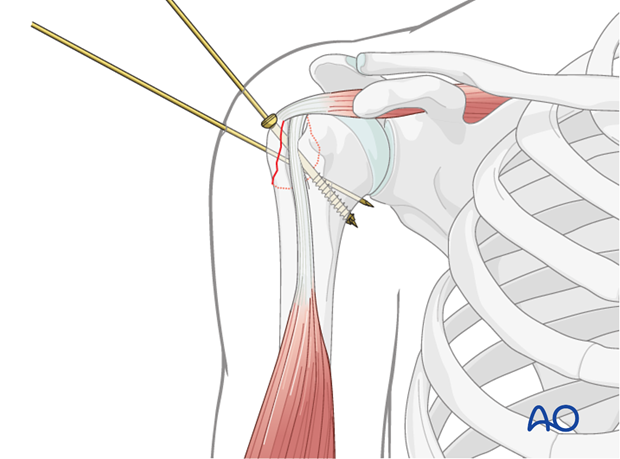
4. Definitive Screw Fixation
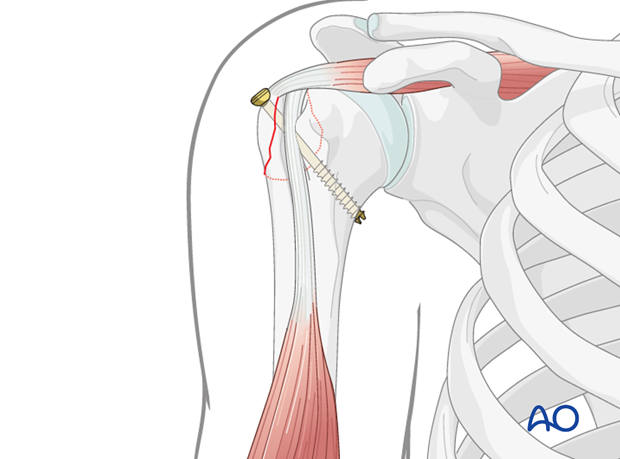
- Screw Selection: Cannulated partially threaded screws (e.g., 3.5mm, 4.0mm, or 4.5mm) are the preferred implants for GT fractures. The partial threading allows for interfragmentary compression as the screw is advanced. Fully threaded cortical screws can also be used, particularly in dense bone, but their ability to compress is limited.
-
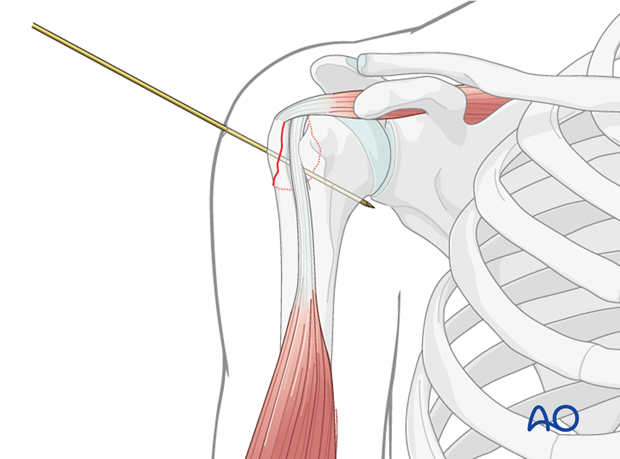
Guidewire Insertion:
- Under continuous fluoroscopic guidance, one or two guidewires are inserted through the same or separate small stab incisions, following the desired screw trajectories.
- The guidewires are typically aimed from the lateral aspect of the GT, distally into the humeral head. The trajectory should be oblique, providing maximum purchase in both the fragment and the main humeral shaft.
- Confirm guidewire position and length in AP, lateral, and axillary views. It is critical to ensure the guidewire does not penetrate the articular surface of the humeral head. Repositioning is necessary if articular violation is suspected.
- Measurement: Once the guidewires are optimally placed, a depth gauge is used to measure the appropriate screw length. Select a screw length that provides adequate purchase within the humeral head without being too long and risking penetration of the medial cortex or neurovascular structures.
-
Drilling and Tapping:
- For partially threaded screws, the near cortex (lateral cortex of GT) is typically over-drilled with the appropriate drill bit to allow the screw head to seat and the threads to engage the far cortex (humeral head), thereby achieving compression.
- Tapping may be performed, especially in dense cortical bone, to facilitate screw insertion and prevent stripping of the bone threads.
-
Screw Insertion:
- The cannulated screws are carefully advanced over the guidewires.
- As the screws are tightened, interfragmentary compression should be observed, further stabilizing the fracture.
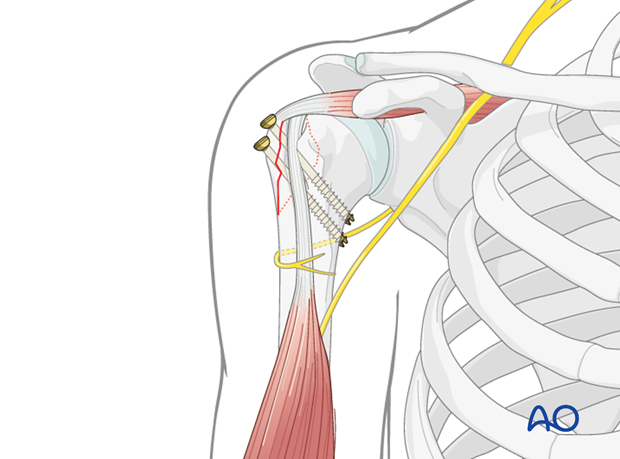
- Typically, two screws are used, inserted in parallel or slightly divergent fashion, to provide both compression and rotational stability. Divergent trajectories offer enhanced resistance to rotational forces.
-
Fluoroscopic Verification:
After screw insertion, repeat fluoroscopic images in multiple planes (AP, lateral, axillary) are crucial to confirm:
- Anatomical reduction of the greater tuberosity.
- Correct screw position and length.
- Absence of articular penetration by any part of the hardware.
-
Overall stability of the construct.
5. Adjunctive Procedures (If Indicated)
- Rotator Cuff Repair: If a significant rotator cuff tear is identified pre-operatively or intra-operatively (e.g., arthroscopically), concurrent repair using suture anchors or transosseous sutures can be performed. This can enhance the stability of the GT fragment, especially if the cuff attachment is compromised.
- Arthroscopic Evaluation: Arthroscopy can be valuable to visually confirm reduction from within the joint, assess for any articular damage, identify and address associated intra-articular pathologies, and directly visualize the rotator cuff.
6. Wound Closure
- Irrigation: The surgical site is thoroughly irrigated with sterile saline.
- Deltoid Closure: If a deltoid split was performed, the muscle fascia is loosely reapproximated.
- Subcutaneous Closure: The subcutaneous tissues are closed in layers.
- Skin Closure: The skin incisions are closed with sutures or staples. A sterile dressing is applied.
Complications & Management
Despite meticulous surgical technique, complications can arise following screw fixation of greater tuberosity fractures. Awareness of these potential issues and strategies for their management is crucial for optimal patient care.
Common Complications and Management Strategies
| Complication | Incidence | Salvage Strategy / Management |
|---|---|---|
| 1. Secondary Displacement / Malunion | The primary risk for initially nondisplaced fractures, can occur if fixation is inadequate, bone quality is poor, or rehabilitation is too aggressive. Higher rates reported with non-operative management of "at-risk" fractures. |
Conservative:
For asymptomatic or minimally symptomatic malunion with acceptable function, observation and physical therapy.
Surgical: For symptomatic malunion (pain, impingement, restricted ROM): - Corrective Osteotomy: If displacement is significant and fragment is viable. - Hardware Removal + Debridement: If impingement is primarily due to prominent hardware or scarred tissue. - Arthroscopic Acromioplasty: To decompress subacromial space. - Arthroplasty: In severe, chronic cases with articular degeneration. |
| 2. Nonunion | Relatively uncommon with stable fixation, but can occur with inadequate reduction, poor bone quality, infection, or insufficient vascularity. |
Conservative:
For asymptomatic nonunion, observation.
Surgical: For symptomatic nonunion: - Revision ORIF with Bone Grafting: Autograft or allograft to promote healing. - Suture Augmentation: To enhance fixation stability. - Arthroplasty: As a salvage procedure in chronic, failed cases. |
| 3. Screw Penetration (Articular) | Variable, depends heavily on surgical precision and fluoroscopic control. Can be 1-5% in some series. Leads to chondral damage, pain, and accelerated osteoarthritis. |
Intraoperative:
Immediate detection and repositioning or removal of the offending screw.
Postoperative (Symptomatic): - Arthroscopic Screw Removal: Often preferred due to minimal invasiveness. - Open Screw Removal: If arthroscopic removal is not feasible. - Debridement of Articular Cartilage: If significant damage is present. |
| 4. Neurovascular Injury |
Axillary Nerve:
Most common (0.5-2%), due to traction, direct trauma during deltoid split (>5cm distal to acromion), or guidewire/screw placement. Manifests as deltoid weakness/atrophy, "regimental badge" sensory loss.
Other Nerves: Less common. |
Conservative:
For neuropraxia, observation, electrodiagnostic studies (EMG), physical therapy. Recovery often takes 6-12 months.
Surgical: For suspected transection or persistent deficit: - Nerve Exploration and Repair/Grafting: If indicated by EMG or clinical progression. |
| 5. Infection | Low (0.5-2%), but potentially devastating. Presents as pain, redness, warmth, swelling, purulent discharge. |
Superficial:
Oral antibiotics, local wound care.
Deep (early): Extensive irrigation & debridement, IV antibiotics (culture-specific), potentially retaining stable hardware. Deep (late/recalcitrant): Hardware removal, prolonged IV antibiotics, debridement. Chronic: May require staged reconstruction. |
| 6. Shoulder Stiffness / Adhesive Capsulitis | Relatively common (5-20%) after shoulder trauma and surgery, particularly with prolonged immobilization or inadequate rehabilitation. |
Conservative:
Aggressive physical therapy, stretching, modalities.
Medical: NSAIDs, corticosteroid injections (subacromial or intra-articular). Surgical: - Manipulation Under Anesthesia (MUA): To restore range of motion. - Arthroscopic Capsular Release: For refractory cases. |
| 7. Hardware Irritation / Prominence | Common, especially with subcutaneous placement of screw heads in thin patients. Can cause palpable discomfort or bursal irritation. |
Conservative:
Observation if mild.
Surgical: - Hardware Removal: Typically performed after fracture union (6-12 months post-op) if symptoms are persistent. |
| 8. Rotator Cuff Pathology | Pre-existing or iatrogenic tears, tendinitis. |
Conservative:
Physical therapy, NSAIDs, injections.
Surgical: - Arthroscopic Debridement or Repair: For symptomatic tears or impingement. |
Post-Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is paramount for optimizing functional recovery and preventing complications such as stiffness or secondary displacement after screw fixation of a greater tuberosity fracture. The protocol must be individualized based on fracture stability, fixation strength, bone quality, associated injuries, and patient compliance.
Phase 1: Protection and Early Passive Motion (Weeks 0-6)
Goals:
* Protect the healing fracture and fixation.
* Control pain and inflammation.
* Prevent shoulder stiffness and maintain soft tissue mobility.
* Promote early bone healing.
Management:
*
Immobilization:
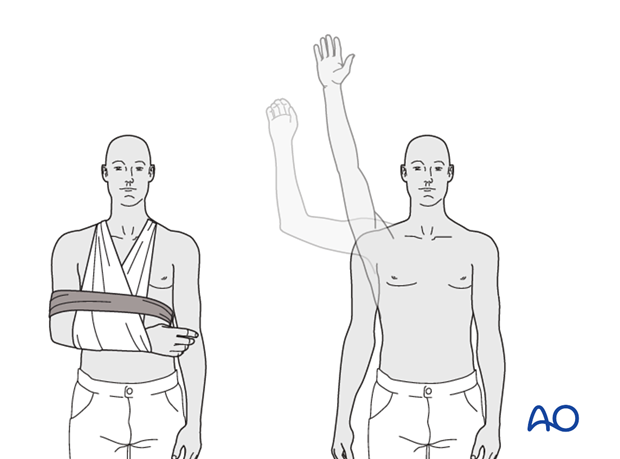
The arm is typically placed in a sling for comfort and protection. This can be a simple arm sling or a sling with an abduction pillow, depending on surgeon preference and the specific fixation stability. The sling is worn continuously, except during exercises and hygiene.
*
Pain Management:
Multimodal analgesia, including NSAIDs, acetaminophen, and judicious use of opioids.
*
Initiation of Motion:
*
Passive Range of Motion (PROM):
Begins within the first week.
*
Pendulum Exercises:
Gentle, gravity-assisted swings of the arm in flexion, extension, and circular motions. Patient is instructed to relax the shoulder entirely.
*
Supine PROM:
With the aid of the non-operative hand or a therapist, gentle flexion to 90-120 degrees, external rotation to 0-30 degrees (avoiding stress on the posterior cuff and GT), and internal rotation to the abdomen.
*
Avoid:
Active abduction, active external rotation, or any active motion that puts direct stress on the rotator cuff and fracture site. No lifting, pushing, or pulling.
*
Elbow, Wrist, Hand Exercises:
Active range of motion for these joints to prevent stiffness and maintain circulation.
*
Cryotherapy:
Application of ice to reduce swelling and pain.
Phase 2: Gradual Active Motion and Light Strengthening (Weeks 6-12)
Goals:
* Restore full passive range of motion.
* Initiate active range of motion (AROM).
* Begin isometric strengthening.
* Improve neuromuscular control.
Management:
*
Sling Discontinuation:
Gradually wean off the sling as pain allows and active control improves, typically by 6 weeks.
*
Active Range of Motion (AROM):
* Progress from active-assisted range of motion (AAROM) to full AROM as tolerated, including flexion, abduction, and rotation.
* Use pulleys, dowel sticks, and wall walks to assist with motion.
* Continue PROM to ensure no regression.
*
Isometric Strengthening:
* Begins at approximately 6-8 weeks.
* Gentle isometric contractions for the rotator cuff (internal rotation, external rotation, abduction) and deltoid, performed against a wall or therapist's hand, without movement. Start with low intensity and gradually increase.
*
Scapular Stabilization Exercises:
Focus on periscapular muscle strengthening to provide a stable base for glenohumeral motion.
*
Avoid:
Heavy lifting, overhead activities, and activities involving sudden jerking motions.
Phase 3: Advanced Strengthening and Return to Activity (Weeks 12-24+)
Goals:
* Maximize strength, endurance, and power.
* Restore full functional range of motion.
* Improve proprioception and neuromuscular control.
* Gradual return to sport-specific or work-related activities.
Management:
*
Progressive Strengthening:
* Begin with light resistance exercises using elastic bands or light dumbbells for rotator cuff and deltoid muscles.
* Progress to isotonic exercises for all major shoulder muscle groups.
* Eccentric strengthening exercises.
* Focus on full range of motion against resistance.
*
Endurance Training:
Low-resistance, high-repetition exercises.
*
Proprioceptive Training:
Balance and coordination exercises (e.g., using unstable surfaces, throwing and catching light objects).
*
Sport/Work-Specific Training:
Gradually introduce activities relevant to the patient's desired level of function, mimicking movements, and gradually increasing intensity and resistance.
*
Return to Activity:
Full return to high-demand activities or contact sports is typically allowed around 4-6 months post-surgery, provided the patient has achieved full strength, range of motion, and radiographic evidence of fracture union. This decision should be made in consultation with the surgeon and therapist.
Criteria for Progression:
Progression through the rehabilitation phases is guided by:
* Pain levels (minimal to no pain with exercises).
* Achievement of specific range of motion goals.
* Demonstrated strength gains.
* Radiographic evidence of fracture healing (callus formation, bridging bone).
* Patient compliance and understanding of the protocol.
Close communication between the surgeon, physical therapist, and patient is essential for a successful rehabilitation journey.
Summary of Key Literature / Guidelines
The management of greater tuberosity fractures, particularly those initially deemed "nondisplaced" but at risk of secondary displacement, has evolved with advances in imaging, surgical techniques, and a better understanding of fracture biomechanics. While historically many such fractures were managed non-operatively, a growing body of literature supports early surgical intervention in selected cases to prevent adverse outcomes.
1. Rationale for Operative Intervention in Nondisplaced GT Fractures:
The primary rationale for fixing initially nondisplaced greater tuberosity fractures stems from the potential for secondary displacement. Studies consistently demonstrate that the deforming forces of the rotator cuff (supraspinatus and infraspinatus) can lead to significant superior and posterior migration of the fragment. A systematic review by Xu et al. (2014) highlighted that despite initial non-displacement, up to 30-40% of GT fractures can displace secondarily, leading to malunion, impingement, and functional deficits. Operative fixation aims to counteract these forces, ensuring anatomical healing and preventing impingement.
2. Displacement Thresholds and Clinical Significance:
The acceptable degree of displacement for GT fractures remains a topic of debate, but general consensus suggests that superior displacement greater than 5 mm to 10 mm can lead to subacromial impingement and is an indication for surgical intervention in active patients. Several authors, including Neer, have suggested a 5mm threshold for symptomatic malunion. This threshold serves as a guiding principle, although individual patient factors (age, activity level, hand dominance) heavily influence the decision-making process. The literature indicates that patients with malunited greater tuberosity fractures, even seemingly minimal displacement, can experience persistent pain, weakness, and limited range of motion, particularly in abduction and external rotation.
3. Comparison of Operative vs. Non-Operative Outcomes:
For truly stable, minimally displaced GT fractures (e.g., <3-5 mm displacement, without significant rotator cuff pull), non-operative management with appropriate immobilization and early rehabilitation can yield good results, especially in elderly, low-demand patients. However, for those "at-risk" fractures, studies have shown improved outcomes with surgical fixation. For instance, a prospective study by Maren et al. (2015) demonstrated better functional scores (e.g., Constant score) and lower rates of secondary displacement in operatively treated "at-risk" GT fractures compared to a closely observed non-operative group. The key is appropriate patient and fracture selection.
4. Surgical Techniques and Preferred Implants:
Cannulated screw fixation, either percutaneous or through a limited open approach, is a widely accepted and effective method for stabilizing GT fractures. The use of partially threaded screws allows for interfragmentary compression, which is crucial for fracture healing. The literature supports using at least two screws to provide rotational stability. Studies by Meier et al. (2010) and other biomechanical analyses have demonstrated the superior stability of two-screw constructs over single-screw fixation. The growing trend towards minimally invasive techniques, often aided by arthroscopy, has been shown to reduce soft tissue morbidity while achieving stable fixation and allowing for simultaneous assessment and repair of associated rotator cuff pathology.
5. Role of Arthroscopy:
Arthroscopic assistance has gained prominence for GT fracture fixation. It allows for direct visualization of the articular surface to ensure accurate reduction and rule out articular involvement or intra-articular screw penetration. Furthermore, it facilitates the assessment and repair of concomitant rotator cuff tears, which are frequently associated with GT fractures. Evidence suggests that arthroscopically assisted reduction and fixation can lead to comparable or superior outcomes to open techniques, with the added benefits of reduced soft tissue dissection and improved diagnostic capabilities.
6. Rehabilitation Protocols:
Consensus guidelines, such as those from the AO Foundation, emphasize a phased rehabilitation protocol. The initial phase focuses on protection and early passive motion to prevent stiffness without compromising fixation. Subsequent phases gradually introduce active motion and progressive strengthening. Adherence to a structured rehabilitation program is critical for achieving optimal functional recovery and preventing complications like stiffness, as highlighted by numerous clinical outcomes studies.
7. Long-Term Outcomes:
Long-term studies on surgically fixed GT fractures generally report good to excellent functional outcomes, with low rates of reoperation for symptomatic malunion or nonunion when anatomical reduction and stable fixation are achieved. However, potential issues like hardware irritation necessitating removal, and the risk of shoulder stiffness, remain considerations that require patient counseling.
In conclusion, the current literature strongly supports a proactive approach to initially nondisplaced greater tuberosity fractures that demonstrate features placing them at high risk for secondary displacement. While non-operative management remains appropriate for truly stable fractures in low-demand patients, prophylactic screw fixation in selected cases, guided by meticulous pre-operative planning, precise surgical technique (often minimally invasive with fluoroscopic and/or arthroscopic assistance), and a structured rehabilitation protocol, offers superior results in preventing malunion and optimizing long-term shoulder function.
You Might Also Like
