Why Straight Nails Excel for Surgical Neck Impaction Fixation

Key Takeaway
This topic focuses on Why Straight Nails Excel for Surgical Neck Impaction Fixation, Neck impaction fixation often utilizes straight or bent intramedullary nails for proximal humeral fractures. Straight nails provide superior fixation in osteoporotic bone and avoid critical fracture lines by positioning medial to them. They also facilitate direct lesser tuberosity fixation. Bent nails may interfere with the rotator cuff footprint or pass through fracture lines. Precise nail entry point and axillary nerve protection are critical for successful neck impaction fixation.
Introduction & Epidemiology
Proximal humeral fractures represent a significant portion of all fractures, accounting for approximately 4-5% of all adult fractures and ranking as the third most common fracture in the elderly population, following hip and distal radius fractures. The incidence of these injuries demonstrates a clear bimodal distribution: high-energy trauma in younger, active individuals, and low-energy falls in osteoporotic elderly patients. With an aging global demographic, the prevalence of osteoporosis-related fractures of the proximal humerus is projected to rise substantially, posing an increasing socioeconomic burden.
Management strategies for proximal humeral fractures span a spectrum from non-operative treatment to various surgical interventions, including open reduction and internal fixation (ORIF) with plates and screws, intramedullary (IM) nailing, hemiarthroplasty, and reverse total shoulder arthroplasty. The optimal treatment choice is multifactorial, depending on patient age, activity level, bone quality, fracture morphology (classified by Neer or AO systems), and the surgeon's expertise.
Intramedullary nailing has emerged as a preferred method for specific fracture patterns, particularly displaced two-part surgical neck fractures, certain three-part fractures, and increasingly, even select four-part fractures in the appropriate patient. The principle of load sharing, inherent to IM fixation, is particularly advantageous in osteopenic bone, offering a biomechanically superior construct compared to load-bearing plates in certain scenarios. Additionally, the minimally invasive nature of IM nailing potentially reduces soft tissue dissection, preserves vascularity to the humeral head, and may lead to improved functional outcomes and lower complication rates compared to extensive open approaches.
This discourse aims to elucidate the specific advantages of straight intramedullary nails for surgical neck impaction fixation, contrasting their design and biomechanical characteristics with those of bent nails. We will critically examine how the unique features of straight nails mitigate common challenges associated with proximal humeral fracture fixation, including interference with the rotator cuff footprint, superior fixation in osteoporotic bone, avoidance of fracture lines, and optimized screw fixation patterns.
Surgical Anatomy & Biomechanics
A thorough understanding of the complex anatomy and biomechanics of the proximal humerus is paramount for successful surgical intervention.
Surgical Anatomy
The proximal humerus comprises several critical structures:
*
Humeral Head:
The articular portion, articulating with the glenoid. Its vascularity is supplied predominantly by the arcuate artery, a branch of the anterior circumflex humeral artery, and contributions from the posterior circumflex humeral artery and ascending branch of the anterior humeral circumflex artery. Disruption of these delicate vessels is a significant concern in displaced fractures, predisposing to avascular necrosis (AVN).
*
Anatomical Neck:
The demarcation between the humeral head and the tuberosities. Fractures here often carry a higher risk of AVN.
*
Surgical Neck:
The region distal to the tuberosities, representing a common site for fractures. This is the primary focus for impaction fixation with intramedullary nails.
*
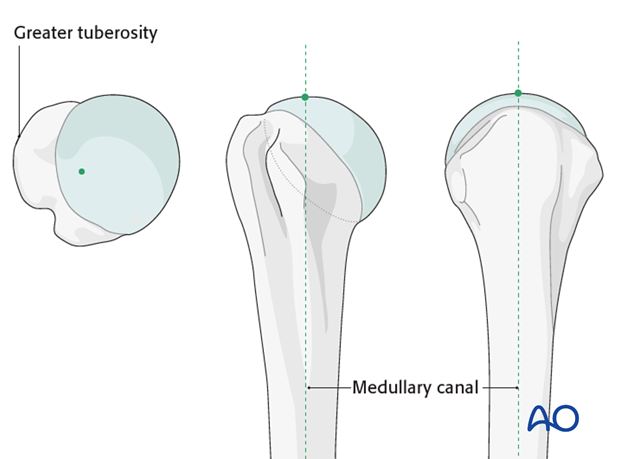
Greater Tuberosity:
Site of insertion for the supraspinatus, infraspinatus, and teres minor tendons. Its superior aspect, the rotator cuff footprint, is a critical zone.
*
Lesser Tuberosity:
Site of insertion for the subscapularis tendon.
*
Bicipital Groove:
Located between the greater and lesser tuberosities, housing the long head of the biceps tendon.
The rotator cuff musculature (supraspinatus, infraspinatus, teres minor, subscapularis) plays a crucial role in shoulder stability and motion. The supraspinatus tendon inserts onto the superior facet of the greater tuberosity. Its footprint is a vital area, and any iatrogenic damage or disruption can compromise shoulder function.
Bone Density and Quality
The proximal humerus exhibits heterogeneous bone density. The superior humeral head, particularly the medial calcar, generally possesses higher cancellous bone density compared to the greater tuberosity, which, in osteoporotic patients, can be significantly demineralized. This variation in bone quality has direct implications for implant purchase and stability. Fixation devices that engage denser bone regions are inherently more stable, particularly against pull-out forces.
Biomechanics of Proximal Humerus Fractures
Proximal humeral fractures result from complex loading patterns. The deltoid muscle exerts a superiorly directed force, while the rotator cuff muscles exert compressive and rotational forces. In impaction fractures of the surgical neck, the humeral head is driven into the metaphysis. These fractures can be either valgus-impacted (angulated laterally) or varus-impacted (angulated medially). Valgus impaction is often more stable due to the inherent bony buttress. Varus impaction, however, is a common and challenging pattern, prone to collapse under axial loading and deltoid pull, leading to nonunion or malunion.
Intramedullary Nailing Biomechanics
Intramedullary nails function as load-sharing devices, meaning they bear a portion of the load while the bone itself carries the remainder. This contrasts with load-bearing plates, which assume the majority of the load. In osteoporotic bone, load sharing is advantageous as it reduces stress shielding and allows for more physiological loading of the bone, potentially promoting healing.
The trajectory and placement of an IM nail critically influence its biomechanical performance:
*
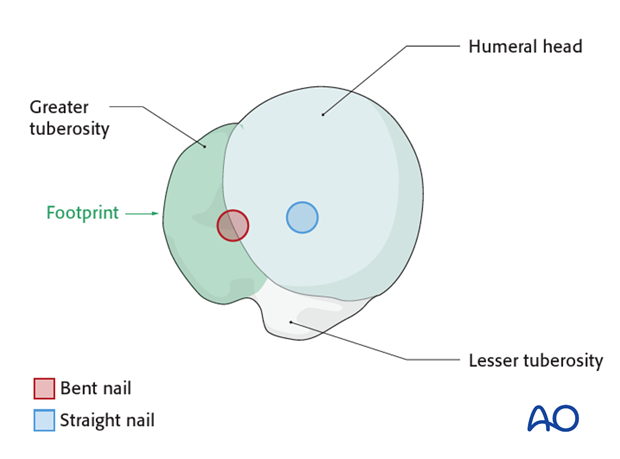
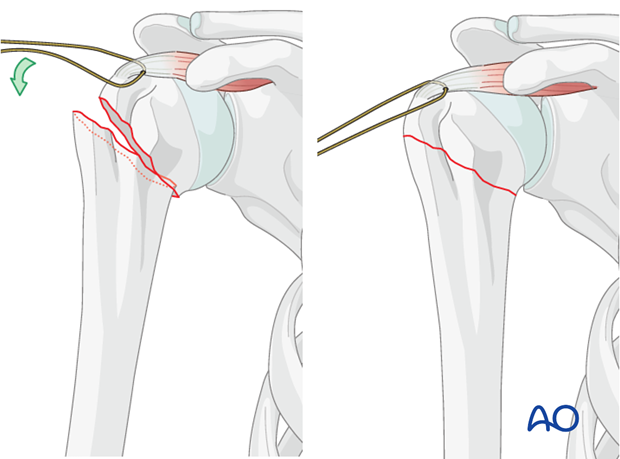
Rotator Cuff Footprint Interference:
A primary advantage of straight nails relates to their entry point. The entry point for a
bent nail
typically lies more laterally, often through the bony attachment of the rotator cuff (the supraspinatus footprint on the greater tuberosity). This creates a permanent bony defect in the footprint, which cannot be reconstructed, potentially compromising rotator cuff function and leading to impingement. In contrast, the entry point for a
straight nail
is typically more medial and slightly posterior, lying
under
the rotator cuff. This requires an incision through the substance of the rotator cuff tendon itself, ideally splitting the fibers in line with their natural orientation. This soft tissue incision can then be meticulously repaired side-to-side, preserving the bony footprint and minimizing long-term rotator cuff dysfunction or impingement. This distinction highlights a crucial advantage for anatomical preservation and functional recovery.
*
Fixation in Osteoporotic Bone, Fifth Anchoring Point:
Straight nails, due to their design, permit a more central trajectory within the humeral head. This allows for screw fixation into the denser cancellous bone of the superior humeral head, providing a robust fifth anchoring point, which is particularly beneficial in osteoporotic bone. Bent nails, designed with a lateral curve, tend to follow a path through the greater tuberosity, a region often characterized by lower bone density, especially in elderly, osteopenic patients. Engaging stronger bone through the superior humeral head with a straight nail provides superior pull-out resistance and anti-rotation stability.
*
Interference with Fracture Lines:
In complex proximal humeral fractures, particularly those involving the greater tuberosity, the trajectory of bent nails often passes directly through the fracture line between the greater tuberosity and the humeral head. This can lead to less stable fixation of the tuberosity fragments and potential displacement. Straight nails, by contrast, maintain a more medial trajectory within the humeral head, penetrating medial to such fracture lines, thereby preserving the integrity of the fracture construct and enabling more effective direct fixation of fragments.
*
Fixation Pattern of Screws:
Straight nails, by virtue of their more medial and central alignment within the medullary cavity, allow for optimized multiplanar screw configurations. This central placement facilitates direct fixation of displaced humeral head fragments, promoting anatomical reduction and robust construct stability. This trajectory allows screws to engage the denser bone of the calcar and superior humeral head more effectively, preventing varus collapse and superior migration. The ability to achieve direct fixation of the humeral head fragment, especially in valgus-impacted or varus-impacted surgical neck fractures, is critical for maintaining reduction and preventing complications such as screw cut-out.
Indications & Contraindications
The judicious selection of patients for intramedullary nailing of proximal humeral fractures requires careful consideration of fracture morphology, patient factors, and the inherent advantages and limitations of the implant.
Indications for Operative Fixation (General)
Operative intervention for proximal humeral fractures is generally considered for:
*
Displaced Fractures:
Displacement exceeding 1 cm or angulation greater than 45 degrees, particularly in functionally demanding patients.
*
Unstable Fracture Patterns:
High risk of secondary displacement with non-operative management.
*
Articular Involvement:
Head-splitting fractures, although nailing may be a relative contraindication here depending on fragment size.
*
Neurovascular Compromise:
Acute, non-resolving neurovascular deficit requiring surgical exploration and stabilization.
*
Open Fractures:
To prevent infection and achieve stable skeletal fixation.
*
Polytrauma Patients:
To facilitate early mobilization and rehabilitation.
*
Failed Non-operative Treatment:
Persistent pain, malunion, or nonunion.
Specific Indications for Intramedullary Nailing
Straight intramedullary nails are particularly well-suited for:
*
Two-part Surgical Neck Fractures:
Displaced or unstable.
*
Three-part Fractures:
Involving the surgical neck and one tuberosity (most commonly the greater tuberosity), where anatomical reduction and stable fixation of the tuberosity can be achieved.
*
Four-part Fractures (Select Cases):
Primarily in younger patients with good bone quality, where reduction of all fragments, especially the articular segment, is achievable.
*
Valgus-Impacted Surgical Neck Fractures:
Where the nail can augment the inherent stability and resist further varus collapse.
*
Varus-Impacted Surgical Neck Fractures:
Requiring robust reduction and fixation to prevent collapse.
*
Osteoporotic Bone:
The load-sharing nature of IM nails, combined with the ability of straight nails to engage denser bone in the superior humeral head, makes them advantageous in patients with poor bone quality, where plating may be prone to pull-out.
*
Metaphyseal Commotion:
Where plating may require extensive periosteal stripping.
Contraindications for Intramedullary Nailing
-
Absolute Contraindications:
- Active infection (local or systemic).
- Severe comminution of the articular surface (head-split fracture where fragments are too small to hold screws).
- Severe soft tissue compromise precluding safe surgical incision.
- Anatomical neck fractures where insufficient bone stock for proximal locking screws exists.
- Patients medically unfit for surgery.
-
Relative Contraindications:
- Extremely proximal fractures where adequate distal locking is difficult.
- Significant head impression fractures (e.g., Hill-Sachs lesion equivalent), which may necessitate alternative fixation or arthroplasty.
- Very severe, unreducible four-part fractures, where primary arthroplasty (hemi or reverse) may yield better outcomes.
- Extensive comminution preventing stable reduction.
Operative vs. Non-Operative Indications
| Indication Type | Operative Treatment (IM Nailing often considered) | Non-Operative Treatment (Generally accepted) |
|---|---|---|
| Fracture Pattern | Displaced 2-part surgical neck, 3-part (surgical neck + tuberosity), select 4-part | Minimally displaced or non-displaced 2-part, stable valgus-impacted fractures |
| Displacement | > 1 cm translation | < 1 cm translation |
| Angulation | > 45 degrees (especially varus) | < 45 degrees |
| Instability | High risk of secondary displacement | Stable, low risk of displacement |
| Bone Quality | Good to poor (IMN can be advantageous in osteoporosis) | Can be good to poor (depends on stability) |
| Patient Factors | Younger, active patients; polytrauma; desire for early functional recovery | Elderly, low functional demand; significant medical comorbidities precluding surgery |
| Complications | Open fractures, neurovascular compromise (acute) | No acute neurovascular compromise |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for optimizing surgical outcomes and minimizing complications during intramedullary nailing of proximal humeral fractures.
Pre-Operative Planning
-
Imaging Review:
- Standard Radiographs: True AP, scapular Y, and axillary views are essential to characterize fracture morphology (Neer/AO classification), degree of displacement, angulation, and involvement of the tuberosities.
- Computed Tomography (CT) Scan: Highly recommended for complex fractures, particularly 3- and 4-part patterns, to assess articular involvement, the precise orientation of fracture lines, tuberosity displacement, and comminution. 3D reconstructions can provide invaluable insights into fragment geometry and aid in planning reduction strategies and screw trajectories.
-
Implant Selection and Templating:
- Nail Length and Diameter: Based on radiographic measurements of the contralateral humerus or intra-operative assessment. The nail should extend sufficiently into the diaphysis for adequate distal locking, ideally two to three cortical diameters distal to the fracture, while not impinging on the elbow joint. The diameter should fit snugly within the medullary canal.
- Screw Configuration: Plan the number and trajectory of proximal and distal locking screws. For straight nails, consider the optimal entry point and trajectory to engage the superior, denser bone of the humeral head and potentially capture specific fragments. Assess options for impaction screws or calcar screws.
-
Surgical Strategy:
- Reduction Maneuvers: Anticipate specific maneuvers required to achieve anatomical reduction, such as traction, external rotation, impaction, or the use of joysticks/K-wires.
- Approach: Confirm the planned surgical approach (e.g., deltoid-splitting) and potential challenges.
- Contingency Planning: Prepare for potential intraoperative difficulties, such as irreducible fragments, poor bone quality requiring cement augmentation, or conversion to plating/arthroplasty.
- Patient Counseling: Discuss the surgical procedure, potential risks (e.g., infection, nerve injury, avascular necrosis, nonunion, impingement), expected rehabilitation pathway, and realistic functional outcomes.
Anesthesia
General anesthesia is typically administered. A regional interscalene brachial plexus block can be a valuable adjunct for both intraoperative pain control and excellent post-operative analgesia, reducing the need for systemic opioids.
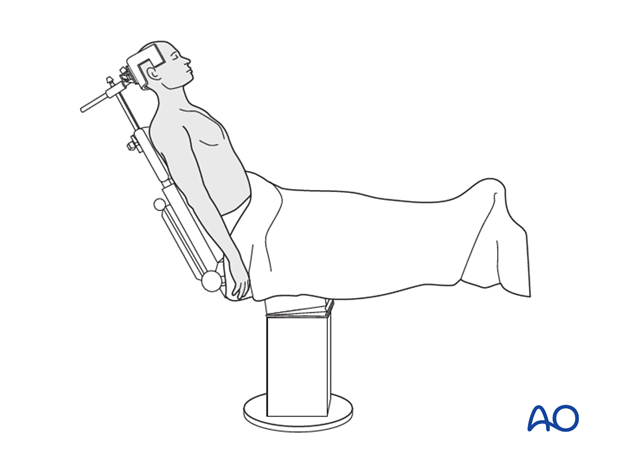
Patient Positioning
The
beach chair position
is generally preferred for IM nailing of the proximal humerus.
*
Advantages:
* Provides excellent access to the shoulder girdle.
* Allows for easy manipulation of the arm for reduction and fluoroscopic imaging in multiple planes (AP, lateral, axillary).
* Facilitates visualization of the entry point and distal locking.
* Reduces venous pooling in the head, potentially minimizing blood loss.
*
Setup:
* The patient is positioned semi-recumbent at approximately 45-70 degrees.
* The head is secured to prevent excessive movement.
* The operative arm is draped free, allowing for full range of motion.
* A beanbag or shoulder positioner can be used to stabilize the torso.
* Ensure appropriate padding at pressure points.
* The image intensifier (C-arm) should be positioned to allow for clear AP, lateral, and axillary views without repositioning the patient. The C-arm should be able to rotate around the patient's shoulder.
*
- This image often depicts patient positioning for shoulder surgery or initial manipulation.
*
Alternative:
The supine position with a bolster under the ipsilateral shoulder can also be used, though it may provide less optimal access for certain maneuvers and fluoroscopic views.
Detailed Surgical Approach / Technique
The surgical technique for intramedullary nailing of the proximal humerus, especially with a straight nail, emphasizes a minimally invasive approach, anatomical reduction, and stable internal fixation.
Surgical Principles
- Indirect Reduction: Minimize soft tissue stripping to preserve the vascularity of the humeral head fragments.
- Stable Fixation: Achieve a robust construct that resists varus collapse, rotation, and shear forces.
- Preservation of Rotator Cuff Function: Crucial for long-term shoulder function.
- Early Mobilization: Enable guided post-operative rehabilitation.
Surgical Approach
A
limited deltoid-splitting approach
is typically used for IM nailing.
1.
Incision:
A small (3-5 cm) skin incision is made over the most superolateral aspect of the shoulder, centered approximately 1-2 cm posterior to the posterolateral corner of the acromion. This position is typically in line with the supraspinatus muscle fibers.
*
- This image likely shows the skin incision or a landmark for the entry point.
2.
Deltoid Split:
The deltoid muscle fibers are carefully split longitudinally, typically no more than 4-5 cm, to avoid injury to the axillary nerve, which runs approximately 5-7 cm distal to the acromion.
3.
Exposure of Rotator Cuff:
The underlying supraspinatus tendon is identified.
*
Key Advantage of Straight Nails:
The entry point for a straight nail typically lies under the rotator cuff, specifically through the supraspinatus tendon, medial to its bony footprint on the greater tuberosity. This requires a carefully placed incision, which should be made in the line of the tendon fibers to minimize damage. The fibers are then spread, not cut transversally. This approach prevents disruption of the critical bony attachment of the rotator cuff. After nail insertion, this soft tissue incision can be effectively closed by side-to-side sutures, promoting healing and preserving rotator cuff integrity.
*
Contrast with Bent Nails:
The entry point for a bent nail is often more lateral, directly through the bony attachment of the rotator cuff on the greater tuberosity. This creates a permanent bony defect in the supraspinatus footprint, which cannot be reconstructed and can lead to persistent rotator cuff dysfunction and impingement. This distinction underscores a primary advantage of the straight nail design for preserving shoulder biology and function.
*

- This image clearly illustrates the difference in entry points between bent and straight nails, highlighting the preservation of the rotator cuff footprint with the straight nail.
Entry Point Preparation
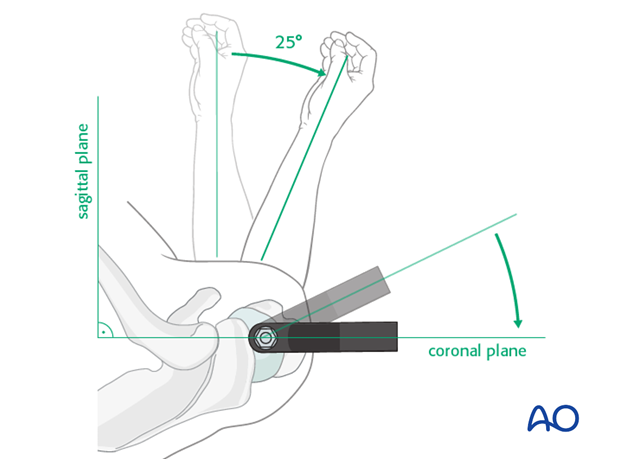
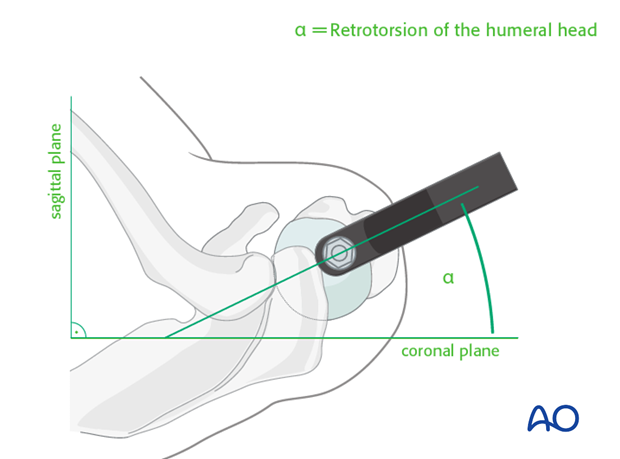
- Identification: The entry point for a straight humeral nail is typically located approximately 5-10 mm medial to the greater tuberosity and 5-10 mm posterior to the bicipital groove, at the apex of the humeral head curvature. This places it centrally within the humeral head, facilitating a straight trajectory down the medullary canal.
- Cuff Incision: A small incision (approximately 1 cm) is made through the supraspinatus tendon, splitting its fibers in line with the tendon, down to the bone.
- Awl/Drill: A starting awl or blunt trocar is used to create an opening in the bone at the identified entry point.
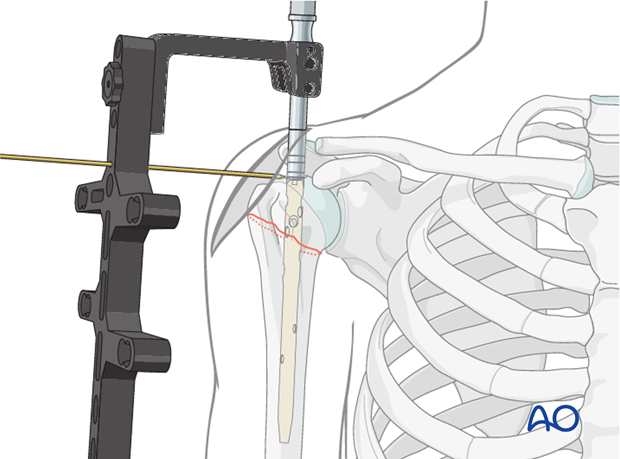
Guide Wire Insertion and Reaming
-
Guide Wire:
A guidewire is carefully inserted through the bone opening, aiming down the central axis of the medullary canal. Fluoroscopy (AP and lateral views) is essential to confirm proper guidewire placement, ensuring it is centered in both planes and extends to the distal metaphysis.
-
- This image is likely showing the guide wire being inserted or its initial placement.
-
-
Reduction Maneuvers:
With the guidewire in place, various techniques are employed to achieve fracture reduction. This may involve:
- Traction: Longitudinal traction on the arm to disimpact fragments.
- External Rotation: Often required to correct internal rotation malalignment.
- Impaction: Gentle impaction may be necessary for valgus-impacted fractures to achieve optimal stability.
- Joystick/K-wires: K-wires inserted percutaneously into displaced fragments (e.g., greater tuberosity) can serve as joysticks to manipulate and reduce fragments.
- Sutures: Heavy non-absorbable sutures can be passed around tuberosity fragments to aid in reduction and hold them against the nail.
-
- This image could depict a reduction maneuver, possibly using a joystick or applying traction. -
- Another image showing reduction or provisional fixation.
-
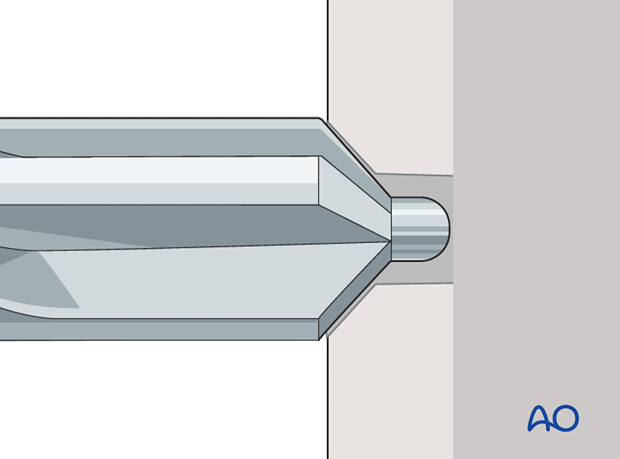
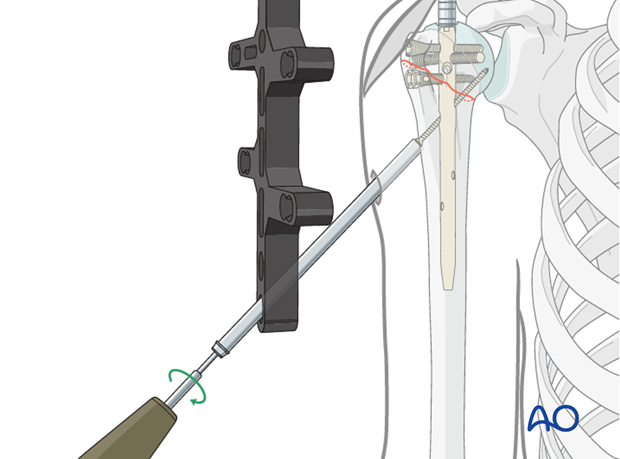
Reaming:
Once satisfactory reduction is achieved, the medullary canal is reamed sequentially over the guidewire to the desired diameter, typically 1.0-2.0 mm larger than the chosen nail diameter. This creates space for nail insertion and minimizes stress on the bone during insertion.
-
- This image clearly shows the reaming process. -
- Another image of reaming or initial nail insertion.
-
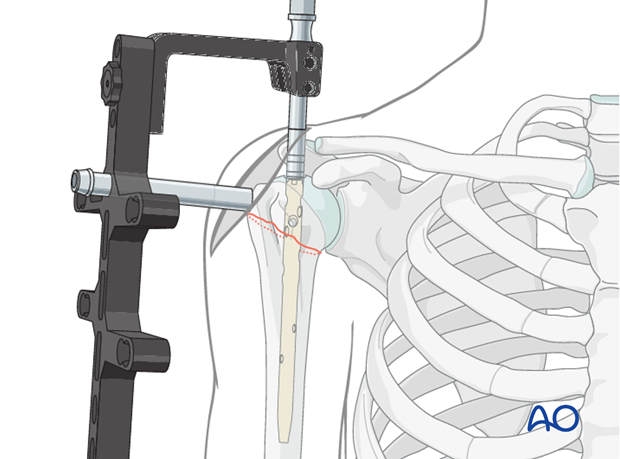
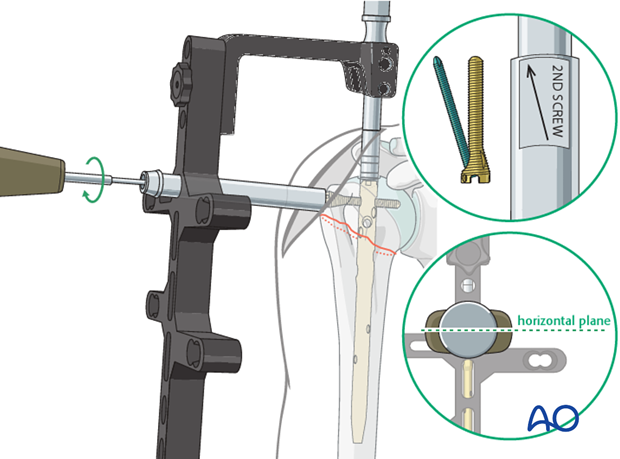
Nail Insertion and Proximal Locking
- Nail Insertion: The straight intramedullary nail is then carefully inserted over the guidewire, using gentle impaction if necessary. The nail should be advanced until its proximal end is flush with or slightly proud of the humeral head, ensuring that the proximal locking screw holes are optimally positioned within the humeral head.
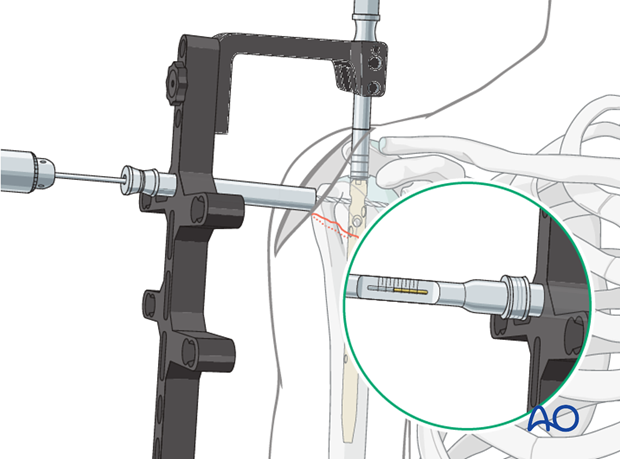
-
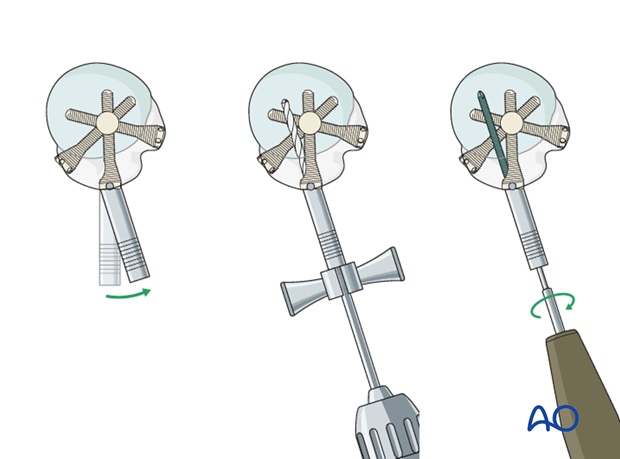
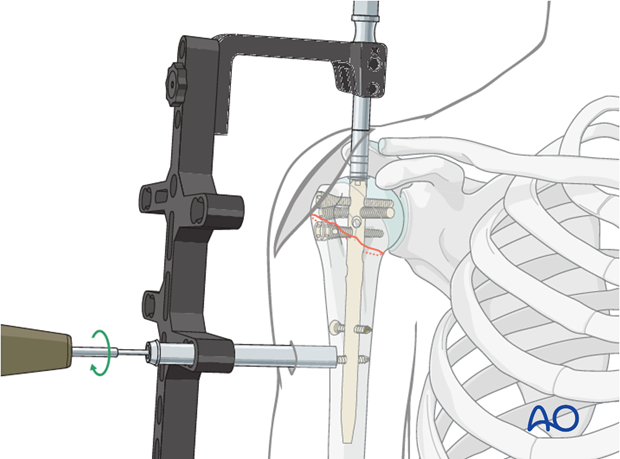
Proximal Locking Screw Placement:
This is where the biomechanical advantages of straight nails become particularly evident.
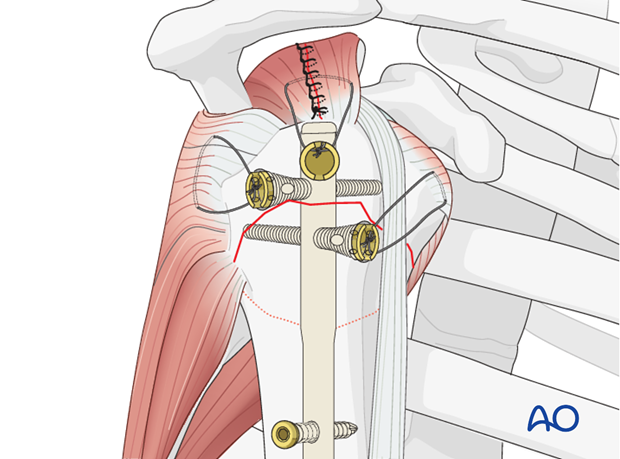
- Engagement of Denser Bone: Straight nails run more medially in the axis of the medullary cavity. This trajectory allows the proximal locking screws to engage the denser cancellous bone of the superior humeral head and the medial calcar. This provides a significantly more robust "fifth anchoring point" (in addition to typical multiplanar screws) compared to bent nails, which often traverse the less dense greater tuberosity. This superior purchase is critical for resisting varus collapse and screw cut-out, especially in osteoporotic bone.
- Avoidance of Fracture Lines: In proximal humeral fractures involving the greater tuberosity, the straight trajectory ensures that the nail and its proximal screws penetrate the humeral head medial to the fracture line between the greater tuberosity and the humeral head. This preserves the integrity of the fracture fragment and enables direct, stable fixation of tuberosity fragments to the main humeral head block, which is challenging with bent nails that often run through these critical fracture planes.
-
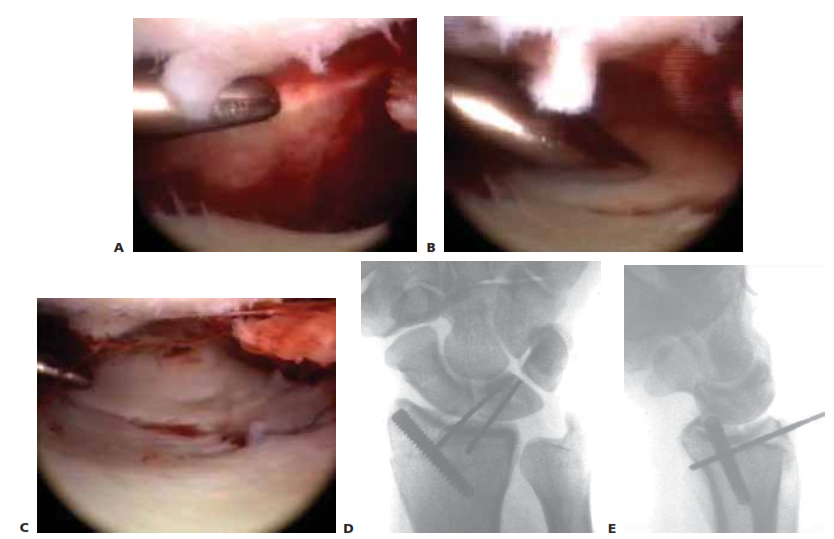
- This image demonstrates the superior fixation in osteoporotic bone by straight nails engaging denser superior humeral head compared to bent nails going through the weaker greater tuberosity. -
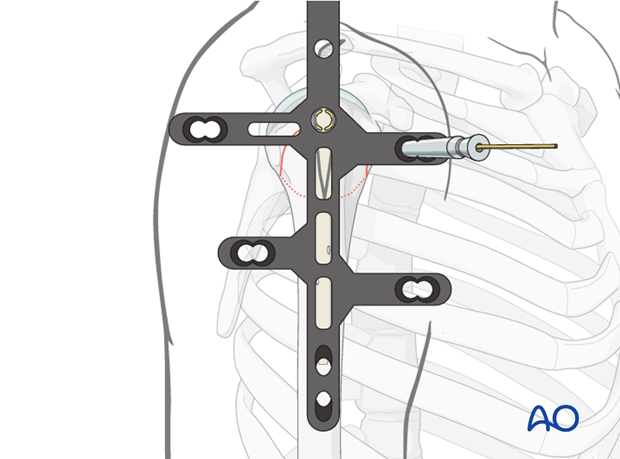
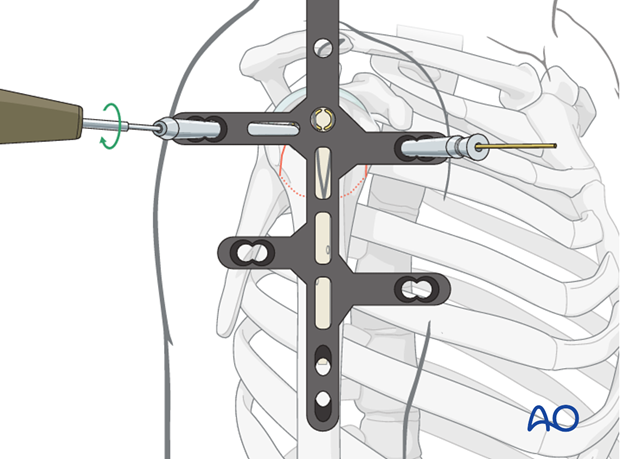
- This image also illustrates how straight nails avoid fracture lines of the greater tuberosity by penetrating medial to them. - Optimal Screw Pattern: Straight nails enable a highly stable, multiplanar locking screw configuration. It is possible to perform a direct fixation of the humeral head fragments, preventing rotation and superior migration. The aiming device guides the placement of these screws, typically 2-4 in number, in various planes to maximize stability. Calcar screws, specifically designed to engage the medial calcar, are particularly important for resisting varus collapse.
-
- This image shows the insertion of a proximal locking screw. -
- A fluoroscopic image demonstrating the position of proximal locking screws. -
- Another view of proximal locking screws in place.
Distal Locking
- Technique: Distal locking is performed to prevent rotational instability and maintain nail length. This can be achieved using a targeting jig or freehand technique with fluoroscopic guidance.
-
Screw Placement:
Typically two distal locking screws are inserted, ensuring bicortical purchase. Anteroposterior and mediolateral views are critical to confirm optimal screw position and length, avoiding neurovascular structures.
-
- This image illustrates the process of distal locking.
-
Final Assessment and Closure
-
Fluoroscopic Confirmation:
Obtain final AP, lateral, and axillary fluoroscopic views to confirm:
- Anatomical reduction of the fracture.
- Optimal position of the intramedullary nail.
- Correct length and position of all proximal and distal locking screws, ensuring no intra-articular penetration or distal impingement.
-
- Final AP fluoroscopic image. -
- Final lateral fluoroscopic image. -
- Another final fluoroscopic view, possibly an axillary.
-
Wound Closure:
- The incision in the supraspinatus tendon should be meticulously repaired with strong, non-absorbable side-to-side sutures. This is crucial for preserving rotator cuff function and preventing impingement symptoms.
- The deltoid muscle is reapproximated.
- Subcutaneous tissues and skin are closed in layers.
-
- This image might show the final closed incision or a post-operative X-ray.
Complications & Management
Despite advancements in surgical techniques and implant design, intramedullary nailing of proximal humeral fractures is associated with a range of potential complications. A thorough understanding of these complications and their management is essential.
General Surgical Complications
- Infection: Superficial or deep surgical site infection. Management involves débridement, antibiotics, and potentially implant removal for chronic deep infections.
- Neurovascular Injury: Damage to the axillary nerve (most common, due to deltoid split or distal locking), radial nerve (due to distal locking), or axillary artery/vein. Careful surgical technique, limited deltoid split, and meticulous distal locking are preventive measures.
- Bleeding/Hematoma: Post-operative hematoma can cause pain and nerve compression.
- Anesthetic Complications: Standard risks associated with general or regional anesthesia.
Intramedullary Nailing Specific Complications
-
Malunion/Nonunion:
- Incidence: Varies widely, but nonunion rates can range from 0-10% and malunion (especially varus) can be higher.
- Pathogenesis: Inadequate reduction, unstable fixation, poor bone quality, premature aggressive rehabilitation, or disruption of vascularity. Varus collapse is a particular concern, especially with non-impacted fractures or insufficient calcar support.
-
Management:
- Asymptomatic Malunion: Often managed non-operatively.
- Symptomatic Malunion/Nonunion: Requires revision surgery, which may include osteotomy, removal of hardware, bone grafting, exchange nailing, plate fixation, or conversion to arthroplasty (hemiarthroplasty or reverse shoulder arthroplasty), depending on the specific deformity and patient factors.
-
Screw Cut-Out/Perforation:
- Incidence: Reported incidence can be as high as 10-20%, particularly for proximal screws.
- Pathogenesis: Primarily due to inadequate screw purchase in osteoporotic bone, secondary varus collapse of the humeral head, or improper screw length (too short for purchase, too long for intra-articular perforation). This complication is less likely with straight nails due to their ability to engage denser bone and provide more robust fixation.
- Management: Varies from observation for asymptomatic intra-articular penetration to hardware removal, revision fixation, or conversion to arthroplasty for symptomatic cut-out or significant collapse.
-
Avascular Necrosis (AVN) of the Humeral Head:
- Incidence: Highly dependent on fracture type, with 4-part fractures having the highest risk (up to 30-40%). Can occur with 3-part fractures as well (5-15%).
- Pathogenesis: Primarily related to the initial traumatic disruption of the blood supply to the humeral head, often exacerbated by extensive soft tissue stripping during surgery.
-
Management:
- Early AVN (asymptomatic): Observation.
- Symptomatic AVN with Collapse: Often requires arthroplasty (hemiarthroplasty or reverse shoulder arthroplasty) once symptoms develop and the head collapses.
-
Rotator Cuff Impingement/Pain:
- Incidence: Can be 5-15%, especially if the nail entry point is prominent or if the rotator cuff incision is not adequately repaired. Less frequent with straight nails due to soft tissue entry and repairable defect, compared to bony footprint damage by bent nails.
- Pathogenesis: Prominent nail, unrepaired rotator cuff defect, scar tissue formation, or iatrogenic damage to the cuff.
- Management: Physical therapy, anti-inflammatory medications. If persistent and severe, hardware removal (especially a prominent nail) or revision cuff repair may be necessary.
-
Loss of Reduction:
- Incidence: More common in highly comminuted fractures or in patients with poor bone quality.
- Pathogenesis: Inadequate primary reduction, unstable construct, or early aggressive rehabilitation.
- Management: Revision fixation if the initial reduction or fixation was inadequate, or conversion to arthroplasty if reconstructive options are limited.
-
Hardware Failure:
- Incidence: Low (1-5%).
- Pathogenesis: Fatigue fracture of the nail or screws, typically due to persistent nonunion, malunion, or excessive stress on the implant.
- Management: Requires revision surgery, including hardware removal, débridement of nonunion, bone grafting, and re-fixation or arthroplasty.
-
Stiffness/Limited Range of Motion:
- Incidence: Very common to some degree.
- Pathogenesis: Immobilization, scar formation, pain, or post-traumatic arthritis.
- Management: Aggressive physical therapy. Manipulation under anesthesia or arthroscopic capsular release may be considered for refractory stiffness.
Table of Common Complications and Management
| Complication | Incidence (Range) | Salvage Strategy |
|---|---|---|
| Malunion/Nonunion | 0-10% (Nonunion) | Asymptomatic: Observe. Symptomatic: Revision ORIF with bone graft, exchange nailing, corrective osteotomy, conversion to hemiarthroplasty (HA) or reverse shoulder arthroplasty (RSA). |
| Screw Cut-Out/Perforation | 10-20% | Asymptomatic: Observe. Symptomatic intra-articular: Hardware removal, potential for revision fixation, HA/RSA. Varus collapse: Revision ORIF, HA/RSA. |
| Avascular Necrosis (AVN) | 5-40% (fracture dependent) | Early/Asymptomatic: Observe. Symptomatic with collapse: HA/RSA. |
| Rotator Cuff Impingement/Pain | 5-15% | Physical therapy, NSAIDs. If refractory: Hardware removal (especially prominent nail/screws), arthroscopic débridement, or cuff repair/revision. |
| Loss of Reduction | Variable | Early revision fixation (ORIF, exchange nailing), HA/RSA if irrecoverable. |
| Hardware Failure | 1-5% | Hardware removal, débridement of nonunion, bone grafting, re-fixation (with new implant), HA/RSA. |
| Infection | < 5% | Superficial: Oral antibiotics. Deep: Surgical débridement, IV antibiotics, hardware retention (if stable) or removal (if unstable/persistent infection), reimplantation. |
| Nerve Injury (Axillary, Radial) | < 1-5% | Conservative management (observation, EMG/NCS), neurolysis if non-recovering, nerve repair/graft if transected. |
| Stiffness/ROM Restriction | Variable | Aggressive physical therapy. Manipulation under anesthesia (MUA), arthroscopic capsular release for refractory cases. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following intramedullary nailing of proximal humeral fractures is crucial for optimizing functional outcomes, restoring range of motion (ROM), and regaining strength, while simultaneously protecting the healing fracture and the surgical repair. The protocol is typically phased, progressing from passive to active motion and then to strengthening, with careful consideration of fracture stability, bone quality, and patient compliance.
Phase I: Immobilization and Early Passive Range of Motion (0-6 Weeks)
-
Goals:
- Protect the healing fracture and surgical fixation.
- Control pain and swelling.
- Prevent shoulder stiffness and maintain glenohumeral joint mobility.
-
Immobilization:
- The arm is typically immobilized in a sling for 4-6 weeks, with periods of removal for hygiene and exercises. The duration depends on the fracture stability achieved intraoperatively and surgeon preference.
-
Pain Management:
- Utilize analgesics (NSAIDs, acetaminophen, neuropathic pain agents as appropriate) and cryotherapy.
-
Early Passive Range of Motion (PROM):
- Initiate gentle pendular exercises (Codman's exercises) within the first few days, performed multiple times daily. These should be truly passive, minimizing active muscle contraction.
- Passive external rotation (ER) to tolerance (typically 0-30 degrees), flexion, and abduction can be initiated with the assistance of a therapist or pulley system, respecting pain and surgeon's precautions. Avoid aggressive stretching.
- Emphasis on maintaining PROM of the elbow, wrist, and hand.
-
Precautions:
- No active abduction or external rotation for 6-8 weeks , to protect the healing rotator cuff repair and prevent varus collapse.
- Avoid lifting, pushing, or pulling with the affected arm.
- Avoid weight-bearing through the arm.
Phase II: Active-Assisted and Active Range of Motion (6-12 Weeks)
-
Goals:
- Gradually increase active range of motion.
- Initiate gentle isometric strengthening.
- Improve neuromuscular control.
-
Progression Criteria:
- Clinical and radiographic signs of early fracture healing (callus formation).
- Minimal pain.
- Achievement of passive ROM goals from Phase I.
-
Active-Assisted Range of Motion (AAROM):
- Progress from PROM to AAROM for flexion, abduction, and external rotation, using pulleys, a wand, or the unaffected arm.
-
Active Range of Motion (AROM):
- Once AAROM is comfortable and controlled, gradually introduce AROM exercises within pain-free limits.
-
Isometric Strengthening:
- Gentle isometric exercises for the rotator cuff (internal/external rotation, abduction) and deltoid can be initiated, performed without resistance against a wall or the patient's own hand.
-
Scapular Stabilization:
- Exercises to improve scapular control and posture are critical for shoulder mechanics.
-
Precautions:
- Continue to avoid heavy lifting or sudden movements.
- Gradual progression is key; avoid pushing into pain.
Phase III: Strengthening and Return to Function (12+ Weeks)
-
Goals:
- Restore full range of motion.
- Progressive strengthening of rotator cuff and deltoid.
- Improve endurance and functional capacity.
- Prepare for return to daily activities, work, and sports.
-
Progression Criteria:
- Solid radiographic fracture healing.
- Good pain control.
- Achieved functional AROM.
-
Progressive Resistance Exercises:
- Gradually introduce resistance exercises using elastic bands, light weights, or machine weights for all planes of motion (flexion, abduction, internal/external rotation).
- Focus on eccentric control and concentric strength.
-
Advanced Scapular Stabilization:
- Incorporate dynamic scapular exercises.
-
Proprioception and Neuromuscular Control:
- Exercises to improve joint position sense and motor control.
-
Sport-Specific/Work-Specific Training:
- For athletes or those with physically demanding occupations, incorporate tailored exercises to simulate specific activities.
-
Return to Activity:
- Gradual return to light activities can begin around 3-4 months post-op, with full unrestricted activities generally permitted around 6 months, assuming complete fracture healing and adequate strength.
Individualization
Rehabilitation protocols must be individualized based on:
*
Fracture Type and Stability:
More complex or unstable fractures may require a more conservative and prolonged immobilization period.
*
Bone Quality:
Osteoporotic bone necessitates a more cautious progression.
*
Patient Age and Activity Level:
Younger, more active patients may have faster healing and desire a quicker return to high-level activities.
*
Surgeon Preference:
Based on intraoperative findings and overall assessment.
*
Pain Levels and Compliance:
Rehabilitation should always be pain-guided, and patient adherence to the protocol is paramount for success.
Summary of Key Literature / Guidelines
The management of proximal humeral fractures has been an area of extensive research and evolving treatment paradigms. Current literature and guidelines support the judicious use of intramedullary nailing, particularly straight nails, for specific fracture patterns.
Evidence for IMN in Proximal Humerus Fractures
Numerous studies have investigated the efficacy of intramedullary nailing for proximal humeral fractures:
*
Systematic Reviews and Meta-Analyses:
These reviews generally conclude that IM nailing provides comparable, and in some aspects superior, outcomes to plate fixation for certain fracture types, particularly two-part and select three-part surgical neck fractures. IM nails tend to demonstrate advantages in terms of reduced soft tissue dissection, potentially lower infection rates, and better load-sharing characteristics, which are beneficial in osteoporotic bone.
*
Functional Outcomes:
Studies evaluating functional scores (e.g., Constant score, ASES score) often show similar or slightly better outcomes for IM nails compared to plates, particularly in the short to medium term.
*
Complication Rates:
While both plating and nailing have distinct complication profiles, some studies suggest IM nailing may have a lower incidence of certain complications like deltoid detachment, extensive periosteal stripping, and potentially fewer reoperations due to hardware-related issues if the nail is well-seated and non-prominent. However, specific complications like rotator cuff irritation or screw cut-out remain concerns, albeit potentially mitigated by straight nail designs.
Comparison of IMN vs. Plate Fixation
The debate between intramedullary nailing and plate fixation for proximal humeral fractures is ongoing, with no single superior treatment for all fracture types:
*
Load Sharing vs. Load Bearing:
IM nails are load-sharing devices, distributing stress across the fracture site and the implant, which is biomechanically advantageous in osteoporotic bone. Plates are load-bearing, creating a stress-shielding effect that can lead to bone atrophy or implant failure in poor bone stock.
*
Minimally Invasive Potential:
IM nailing can often be performed through a smaller incision with less soft tissue dissection compared to extensive open plating, potentially preserving vascularity to the humeral head.
*
Screw Cut-out and Varus Collapse:
While both techniques are susceptible, the ability of straight IM nails to engage denser bone (superior humeral head) and provide more stable impaction can theoretically reduce the risk of screw cut-out and varus collapse compared to plates, especially when placed in weaker tuberosity bone.
*
Rotator Cuff Integrity:
As highlighted in the surgical approach, straight nails offer a significant advantage by allowing a soft tissue entry point through the supraspinatus tendon that can be repaired, preserving the critical bony footprint, unlike the common bony disruption caused by bent nail entry or lateral plate placement.
Straight vs. Bent Nails: Specific Evidence
The specific advantages of straight nails, as discussed in detail above, are supported by biomechanical studies and clinical observations:
*
Biomechanics:
Studies have demonstrated that straight nails, due to their more central trajectory, offer superior resistance to varus collapse and screw pull-out in models simulating osteoporotic bone. The ability to engage the dense superomedial aspect of the humeral head provides a stronger anchorage point.
*
Clinical Outcomes:
While direct randomized controlled trials specifically comparing straight vs. bent nails are less common, clinical series reporting on straight nails highlight their efficacy in minimizing rotator cuff complications and achieving stable fixation, particularly in challenging fracture patterns and osteoporotic bone. The reduced impingement symptoms and preserved rotator cuff function are consistently cited advantages.
Guidelines and Consensus
- AO Foundation Principles: The AO (Arbeitsgemeinschaft für Osteosynthesefragen) principles emphasize anatomical reduction, stable internal fixation, preservation of blood supply, and early, pain-free mobilization. IM nailing, particularly with modern straight nail designs, aligns well with these principles for appropriate fracture types. The AO guidelines acknowledge the role of IM nailing for displaced two- and three-part surgical neck fractures.
- AAOS Guidelines: While specific AAOS (American Academy of Orthopaedic Surgeons) guidelines for straight vs. bent nails may not be extensively detailed, general recommendations for proximal humerus fractures emphasize individualized treatment based on patient factors, fracture characteristics, and a shared decision-making process. The benefits of minimally invasive approaches and stable constructs in osteoporotic bone are generally recognized.
Future Directions
Future research will likely focus on:
* Further refining IM nail designs and materials to enhance stability and reduce complications.
* Developing patient-specific instrumentation or navigation techniques to optimize nail placement and screw trajectories.
* Long-term comparative outcome studies between different IM nail designs and other fixation methods.
* Integrating bone augmentation techniques (e.g., calcium phosphate cement) more routinely to enhance screw purchase in severely osteoporotic bone, potentially improving IM nail outcomes.
In conclusion, the straight intramedullary nail offers distinct biomechanical and clinical advantages for the fixation of surgical neck impaction fractures of the proximal humerus. Its unique design optimizes the entry point to preserve rotator cuff integrity, allows for superior engagement of denser humeral head bone, avoids critical fracture lines, and facilitates a robust multiplanar screw configuration. These attributes position straight nails as an excellent choice for achieving stable fixation and favorable outcomes, particularly in the increasingly prevalent osteoporotic patient population.
You Might Also Like