AOSpine Sacral Fracture Classification System: A Comprehensive Guide
Key Takeaway
The AOSpine sacral fracture classification system is a standardized framework for injury diagnosis. It categorizes sacral fractures based on three criteria: primary injury morphology (Types A, B, C, reflecting pelvic/spinopelvic stability), neurologic status (N0-N4), and case-specific modifiers (M1-M4). This aids precise communication and guides treatment strategies.
Introduction & Epidemiology
The effective management of sacral fractures necessitates a standardized lexicon for precise communication among surgeons, facilitating consistent injury diagnosis and guiding appropriate treatment strategies. The AOSpine sacral fracture classification system represents a concerted effort to establish such an internationally accepted framework. This system categorizes injuries based on three fundamental criteria: morphology of the injury , neurologic status , and case-specific modifiers . The primary injury morphology defines the overarching type, with secondary injuries and modifiers described parenthetically (e.g., (facet injury, neurologic status, case-specific modifiers)).
Morphology of the Injury: AOSpine Sacral Fracture Types
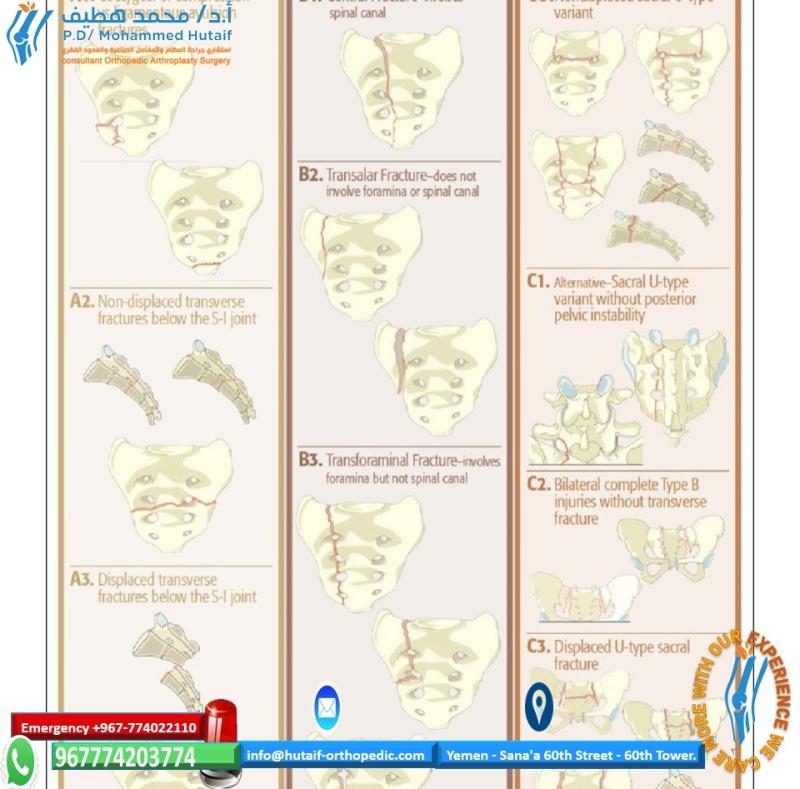
The AOSpine classification utilizes three basic categories (Types A, B, C) to describe the primary injury morphology, building upon historical classifications like Denis zones and Roy-Camille patterns. These types inherently reflect the degree of pelvic and spinopelvic instability.
-
Type A injuries are characterized by lower sacrococcygeal fractures that do not compromise posterior pelvic or spinopelvic stability. These are generally stable fractures of the distal sacrum or coccyx.
- A0: Avulsion fractures. Localized avulsion injuries.
-
A1: Transverse undisplaced coccygeal fractures.
Fractures of the coccyx without significant displacement.
-
A2: Displaced coccygeal fractures.
Coccygeal fractures with notable displacement.
-
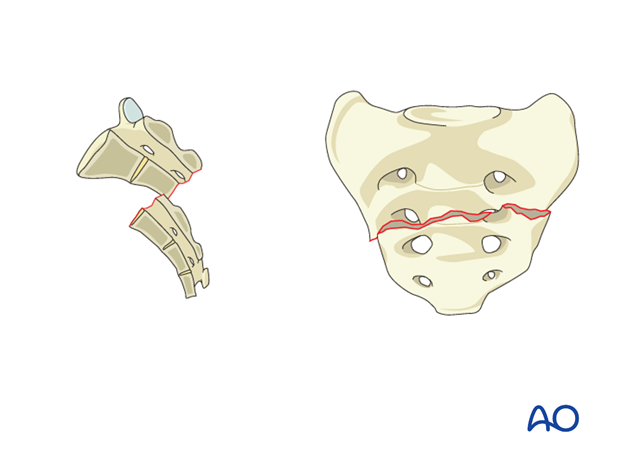
A3: Lower transverse sacral fractures (S3-S5).
Transverse fractures involving the lower sacral segments.
-
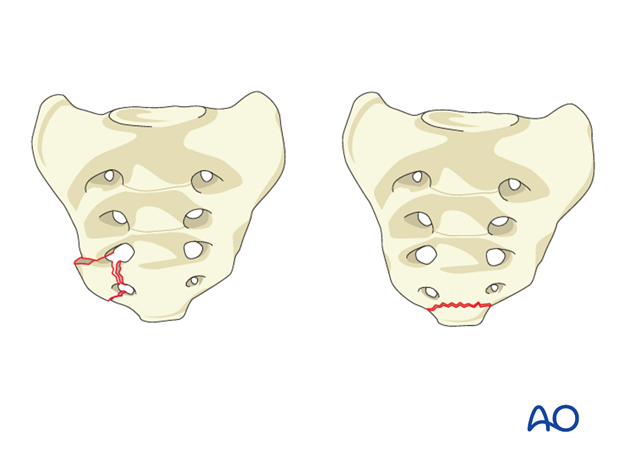
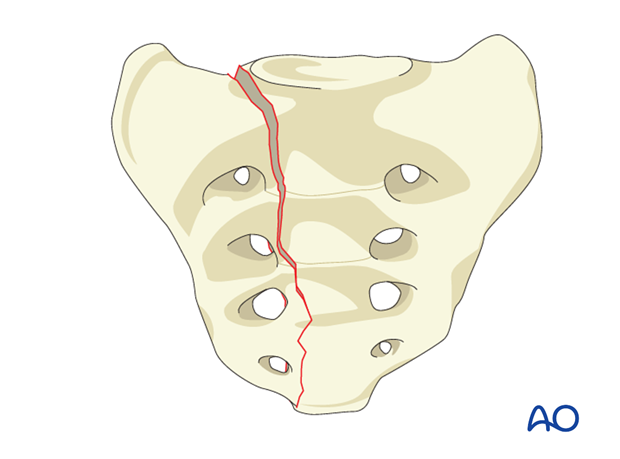
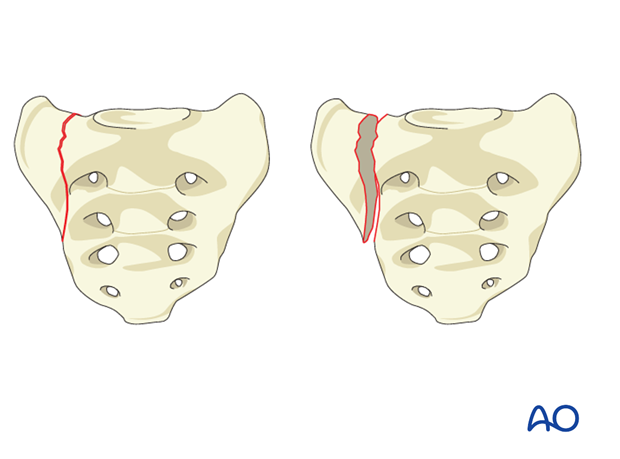
Type B injuries encompass unilateral longitudinal (vertical) sacral fractures, which primarily lead to posterior pelvic instability. These fractures typically do not impact spinopelvic stability. These patterns correspond to Denis Zone I (ala), Zone II (foraminal), and Zone III (central sacral canal) unilateral fractures.
-
B1: Unilateral sacral alar fracture (Denis Zone I).
Vertical fracture through the sacral ala lateral to the foramina.
-
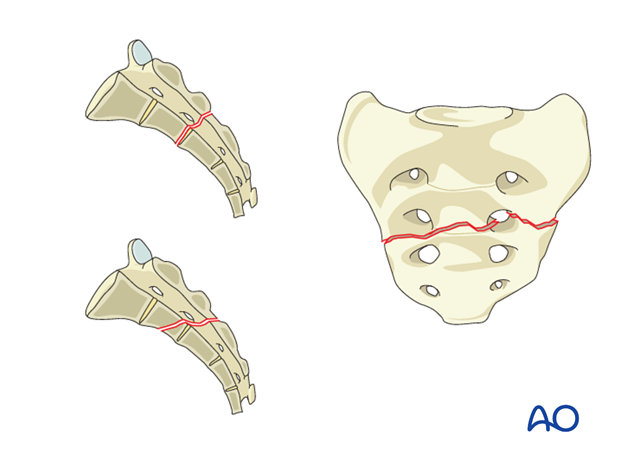
B2: Unilateral transforaminal fracture (Denis Zone II).
Vertical fracture passing through the sacral neuroforamina.
-
B3: Unilateral central sacral fracture (Denis Zone III).
Vertical fracture extending into the sacral canal, medial to the foramina.
-
B1: Unilateral sacral alar fracture (Denis Zone I).
Vertical fracture through the sacral ala lateral to the foramina.
-
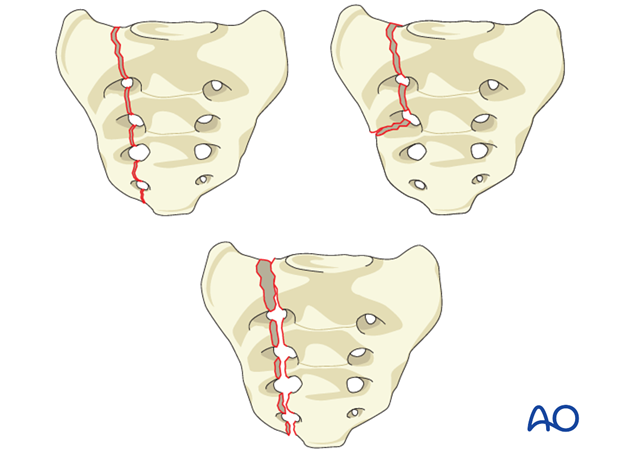
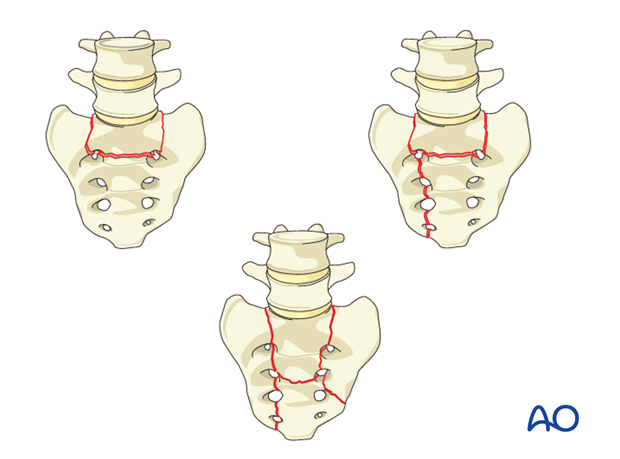
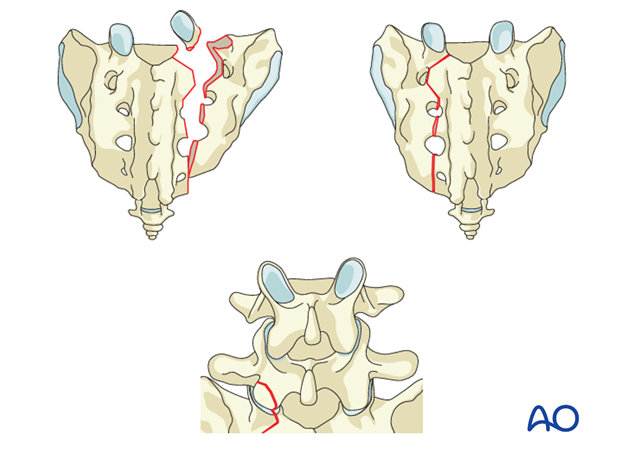
Type C injuries represent the most unstable patterns, characterized by spinopelvic instability. This category includes unilateral B injuries with L5-S1 facet involvement, bilateral longitudinal (vertical) sacral fractures, and U-fracture variations. Sacral U-fracture variations have also been historically classified by Roy-Camille.
-
C0: Isolated L5-S1 facet injury.
Disruption of the L5-S1 facet joint, which can occur with or without an associated sacral fracture.
-
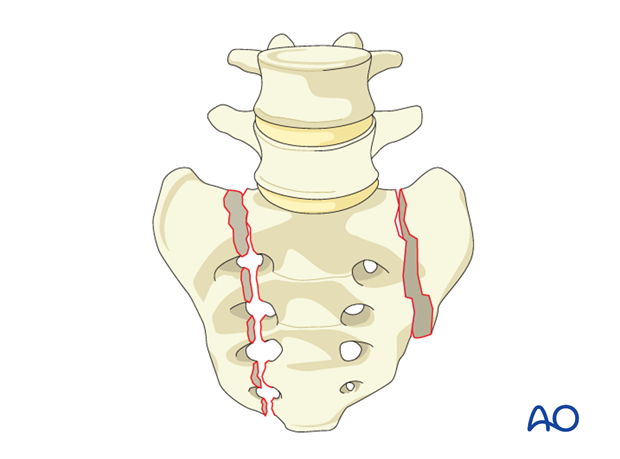
C1: Bilateral sacral alar fractures.
Bilateral vertical fractures through the sacral alae.
-
C2: Bilateral transforaminal fractures.
Bilateral vertical fractures passing through the sacral neuroforamina.
-
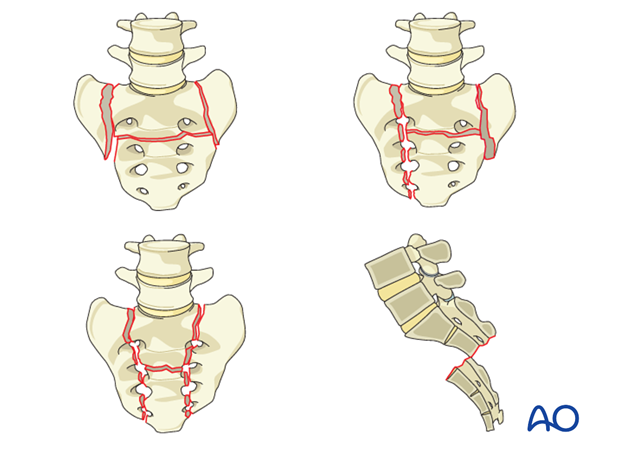
C3: U-type sacral fractures (spinopelvic dissociation).
These are often complex, transverse fractures across the body of S1 or S2, often combined with longitudinal fractures through the lateral masses, leading to complete separation of the spine from the pelvis. This includes H-type, U-type, and lambda-type fractures.
-
C0: Isolated L5-S1 facet injury.
Disruption of the L5-S1 facet joint, which can occur with or without an associated sacral fracture.
Neurologic Status
The neurologic status is a critical component of the AOSpine classification. It quantifies the presence and severity of neurological deficits, which significantly influence treatment decisions and prognosis.
*
N0:
Neurologically intact.
*
N1:
Transient neurological deficit.
*
N2:
Radicular deficit (single nerve root).
*
N3:
Incomplete cauda equina syndrome or multiple radicular deficits.
*
N4:
Complete cauda equina syndrome.
*
NX:
Neurologic status not assessable (e.g., intubated patient, severe TBI).
Case-Specific Modifiers
These modifiers provide additional context crucial for surgical planning.
*
M1:
Local soft tissue compromise (e.g., open fracture, severe degloving).
*
M2:
Significant associated visceral injuries (e.g., bowel, bladder, vascular).
*
M3:
Significant associated spinal column injuries above the sacrum.
*
M4:
Significant associated pelvic ring injuries (e.g., anterior ring disruption) not explicitly part of the sacral fracture type.
Epidemiology
Sacral fractures, while less common than other spinal or pelvic injuries, represent a significant clinical challenge. They constitute approximately 45-60% of all pelvic fractures. The incidence of sacral fractures has risen with an aging population due to increasing fragility fractures secondary to osteoporosis, alongside a sustained prevalence from high-energy trauma in younger demographics.
High-energy mechanisms, such as motor vehicle collisions, falls from height, and pedestrian versus auto accidents, are common etiologies in younger patients. These often result in complex, unstable patterns (AOSpine B and C types) and are frequently associated with other severe injuries, including pelvic ring fractures, long bone fractures, abdominal visceral injuries (e.g., bladder, rectum), and severe neurological deficits. Fragility fractures in the elderly, often resulting from low-energy falls, typically present as less overt, often U-type or H-type patterns (AOSpine C3) and can be missed on initial plain radiographs. While low-energy, these can still result in significant instability and severe pain. Accurate and timely diagnosis is paramount to prevent chronic pain, deformity, and progressive neurological compromise.
Surgical Anatomy & Biomechanics
A profound understanding of sacral anatomy and its biomechanical role is essential for managing sacral fractures.
Surgical Anatomy
The sacrum is a large, triangular bone formed by the fusion of five sacral vertebrae (S1-S5), articulating superiorly with L5 and laterally with the ilium at the sacroiliac (SI) joints.
-
Bony Architecture:
- Promontory: The anterior superior border of S1, articulating with the L5 vertebral body via the L5-S1 disc.
- Ala: The broad lateral mass of S1, articulating with the ilium.
- Sacral Foramina: Four pairs of anterior (ventral) and posterior (dorsal) sacral foramina transmit the ventral and dorsal rami of the sacral nerves, respectively.
- Sacral Canal: Houses the cauda equina, terminating at the sacral hiatus.
- Auricular Surface: The L-shaped articular surface on the lateral aspect of the sacrum, forming the SI joint with the ilium.
- Coccyx: Articulates with the apex of the sacrum, formed by the fusion of three to five small vertebrae.
-
Ligamentous Structures: The stability of the sacrum and pelvis is critically dependent on a robust network of ligaments.
-
Sacroiliac Ligaments:
- Anterior Sacroiliac Ligaments: Relatively thin, covering the anterior aspect of the SI joint.
- Interosseous Sacroiliac Ligaments: The strongest, connecting the sacral tuberosity to the iliac tuberosity, providing significant vertical and rotational stability.
- Posterior Sacroiliac Ligaments: Comprise short and long fibers. The short posterior SI ligaments resist posterior translation of the sacrum, while the long posterior SI ligaments limit anterior rotation of the sacrum.
-
Extrinsic Pelvic Ligaments:
- Sacrotuberous Ligament: Extends from the posterior inferior iliac spine, lower sacrum, and coccyx to the ischial tuberosity. Resists sacral nutation and prevents superior migration of the ischium.
- Sacrospinous Ligament: Extends from the lateral sacrum and coccyx to the ischial spine. Resists sacral nutation and separates the greater and lesser sciatic foramina.
- Iliolumbar Ligaments: Connect L4 and L5 transverse processes to the iliac crest, contributing to L5-S1 stability.
- Lumbosacral Ligaments: Crucial for maintaining spinopelvic alignment, especially the lumbosacral portion of the sacrotuberous ligament.
-
Sacroiliac Ligaments:
-
Neurological Structures: The sacral nerve roots (S1-S5) and the cauda equina are housed within the sacral canal and exit through the sacral foramina. The S1 and S2 nerve roots are particularly vulnerable to injury in transforaminal and central sacral fractures (Denis Zone II/III, AOSpine B2/B3, C2/C3). The lumbosacral trunk (L4, L5) passes anterior to the SI joint and can be affected by SI joint dislocations or severe alar fractures.
-
Vascular Structures: The lateral sacral arteries, branches of the internal iliac artery, run along the lateral masses of the sacrum, anterior to the sacral foramina, and are susceptible to injury during screw placement or extensive dissection. The median sacral artery descends along the anterior surface of the sacrum. The superior gluteal artery and vein exit the pelvis through the greater sciatic notch, superior to the piriformis muscle, and are at risk during posterior fixation, particularly with iliosacral screw placement.
Biomechanics
The sacrum is the keystone of the posterior pelvic ring, acting as a crucial load-transferring structure between the axial skeleton and the lower extremities.
- Load Transfer: Vertical forces from the spine are transmitted through the L5-S1 junction to the sacral body, then diverge bilaterally through the sacral alae and SI joints to the ilia and lower limbs. The strong posterior ligamentous complex (interosseous and posterior SI ligaments) resists shearing forces and stabilizes the SI joints.
-
Pelvic Ring Stability:
The pelvis functions as a closed ring. Disruption of any part, especially the posterior ring, can lead to overall instability.
- Posterior Pelvic Instability: Unilateral longitudinal sacral fractures (AOSpine Type B) primarily compromise posterior pelvic stability, allowing for vertical displacement and rotation of the hemipelvis. The anterior pelvic ring (pubic symphysis, rami) typically remains intact or suffers minor injury in these cases.
- Spinopelvic Instability: The most severe form, seen in AOSpine Type C injuries, particularly U-type fractures (C3) or bilateral longitudinal fractures (C1, C2). In these cases, the continuity between the lumbar spine and the pelvis is lost. The S1 segment effectively separates from the iliac wings, leading to gross instability and potential neurological devastation. Transverse sacral fractures high in S1 or S2 also contribute to spinopelvic dissociation by compromising the sacral body's ability to transmit axial load.
-
Influence of Fracture Pattern on Stability:
- Type A: Minimal biomechanical impact, as they are distal to the major load-bearing axis and robust ligamentous attachments.
- Type B: Unilateral disruption of the posterior arch, compromising SI joint integrity on the affected side. This leads to instability of the ipsilateral hemipelvis, manifested as vertical shear or external rotation.
- Type C: Critical loss of sacropelvic load-bearing capacity. Bilateral longitudinal fractures (C1, C2) disrupt both posterior arches, while U-type fractures (C3) create a floating spine atop a dissociated sacrum, leading to severe instability in all planes (vertical, rotational, transverse). L5-S1 facet injuries (C0) also directly disrupt spinopelvic continuity.
Indications & Contraindications
Management of sacral fractures ranges from non-operative strategies for stable injuries to complex surgical reconstruction for unstable patterns and neurological compromise.
Indications for Operative Management
Operative intervention is generally indicated for unstable sacral fractures, fractures associated with neurological deficits, or those causing significant pain and inability to mobilize.
- AOSpine Type B Fractures: Significant displacement (e.g., >1 cm vertical displacement), significant rotational instability, or persistent pain despite non-operative management.
- AOSpine Type C Fractures: All C-type fractures are inherently unstable and typically require surgical stabilization to restore spinopelvic integrity.
- Neurological Deficit (AOSpine N1-N4): Progressive neurological deficit, or a static deficit associated with fracture fragment impingement requiring decompression.
- Open Fractures: Require urgent debridement and stabilization.
- Polytrauma Patients: Early stabilization of unstable pelvic and sacral fractures helps reduce pain, blood loss, and facilitates mobilization, improving overall patient outcomes.
- Failed Non-Operative Management: Persistent severe pain or progressive deformity despite appropriate conservative care.
- Significant Displacement/Deformity: Displacement greater than 1 cm in any plane, or >10-15 degrees of angular deformity.
- Sacral Kyphosis: High transverse sacral fractures (often C3 variant) causing significant kyphosis of the sacrum.
Contraindications for Operative Management
-
Absolute Contraindications:
- Patient instability incompatible with surgery (e.g., severe coagulopathy, uncontrolled sepsis, moribund state). Resuscitation and stabilization take precedence.
-
Relative Contraindications:
- Severe local soft tissue conditions (e.g., severe infection, extensive burns, compromised skin integrity) in the planned surgical field.
- Significant medical comorbidities that significantly increase surgical risk, where the benefit of surgery does not outweigh the risk.
- Undisplaced, stable fractures (e.g., AOSpine Type A, some Type B0 or B1 without significant displacement) in a neurologically intact patient.
Operative vs. Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| AOSpine Fracture Type |
Type C (C0-C3):
All patterns due to spinopelvic instability.
Type B (B1-B3): With >1cm displacement, significant rotational instability, or >10-15° angular deformity. |
Type A (A0-A3):
All patterns, as they are inherently stable.
Type B (B1-B3): Undisplaced (<1cm), stable, and neurologically intact. |
| Neurological Status | Any N1-N4: Especially progressive deficits or static deficits with demonstrable neural compression. N4 (Complete CES): Urgent decompression often warranted, though prognosis is guarded. | N0 (Intact): In the absence of other surgical indications. |
| Displacement/Instability | Significant vertical (>1cm), anterior-posterior, or rotational displacement of sacral segments or hemipelvis. Gross instability on stress radiographs or examination. | Minimal or no displacement (<1cm). Absence of gross instability on examination or imaging. |
| Associated Injuries | Open fractures. Significant associated anterior pelvic ring injury that exacerbates posterior instability. Polytrauma patients benefiting from early stabilization. Associated visceral injuries requiring concurrent repair. | Isolated sacral fracture without significant associated injuries. |
| Patient Factors | Inability to mobilize due to pain despite adequate analgesia. Anticipated prolonged bed rest leading to complications. | Low demand patient with stable fracture and good pain control. Patient with severe comorbidities precluding surgery (relative contraindication). Frail elderly with stable fracture and acceptable pain, managed with cautious mobilization. |
| Fragility Fractures | Displaced, significantly unstable (C-type patterns), or symptomatic despite conservative management. Consideration for cement augmentation (sacroplasty) in some cases, though not a primary stabilization technique for true fracture instability. | Undisplaced, stable, or minimally displaced fragility fractures with adequate pain control. Initial management typically involves bed rest, analgesia, and gradual mobilization with a walker, progressing to weight-bearing as tolerated. |
| Failed Conservative Care | Persistent, severe, disabling pain, or progression of deformity/instability despite a trial of conservative management. | Resolution of pain and ability to mobilize with conservative measures (bed rest, analgesics, physical therapy, bracing if needed). |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is paramount for successful outcomes in sacral fracture management, mitigating risks and optimizing surgical efficiency.
Pre-Operative Imaging
- Plain Radiographs: Initial assessment with AP pelvis, inlet, and outlet views. These can identify gross displacements but are often insufficient to fully delineate sacral fracture patterns, especially non-displaced or vertically oriented fractures.
-
Computed Tomography (CT):
The gold standard for sacral fracture diagnosis.
- Axial, Coronal, Sagittal Reconstructions: Essential for visualizing fracture lines, displacement, comminution, and involvement of the sacral canal and foramina.
- 3D Reconstructions: Highly valuable for understanding complex fracture morphology, planning implant trajectories, and assessing spinopelvic relationships. They provide an intuitive representation of the injury and aid in communicating the pathology.
- Angiography (CT-A or conventional): Indicated if there is suspicion of arterial injury, particularly in hemodynamically unstable patients or those with expanding hematomas.
-
Magnetic Resonance Imaging (MRI):
Crucial for detailed assessment of soft tissue and neurological structures.
- Ligamentous Injury: Identifies disruption of the SI joint ligaments (interosseous, sacrotuberous, sacrospinous), which are key determinants of pelvic stability.
- Neural Element Compression: Visualizes nerve root impingement, edema, or contusion within the sacral canal or foramina.
- Hematoma/Edema: Detects pre-sacral hematomas or muscle edema.
- Occult Fractures: Particularly useful for detecting insufficiency fractures in osteoporotic patients that may be difficult to visualize on CT.
Patient Optimization
- Hemodynamic Stability: For high-energy trauma, ensure adequate resuscitation and control of hemorrhage. Pelvic binders may be used acutely for temporary stabilization.
- Neurological Assessment: A detailed pre-operative neurological examination is mandatory, documented thoroughly. This provides a baseline for intraoperative and post-operative comparison.
- Associated Injuries: Evaluate and manage all associated injuries (e.g., visceral, long bone fractures). Multidisciplinary involvement (general surgery, urology, vascular surgery) may be necessary.
- Infection Prophylaxis: Administer broad-spectrum intravenous antibiotics pre-operatively.
- DVT Prophylaxis: Implement appropriate DVT prophylaxis measures.
- Pain Management: Optimize pre-operative analgesia to facilitate patient cooperation and comfort.
Patient Positioning
The choice of patient position depends on the planned surgical approach and fracture type.
-
Prone Position:
- Most Common: Preferred for posterior approaches (iliosacral screw fixation, lumbopelvic fixation, tension band plating).
- Advantages: Excellent access to the posterior sacrum and ilium. Allows for easy C-arm access for inlet, outlet, and lateral views.
- Setup: Patients are positioned on a radiolucent operating table, typically on a Wilson frame or bolsters, ensuring the abdomen is free to minimize venous congestion. Care must be taken to pad all pressure points (cheeks, eyes, breasts, genitalia, knees, feet). Arms are typically abducted and supported.
- Considerations: Secure head and neck position. Ensure appropriate endotracheal tube and IV line management.
-
Lateral Position:
- Less common, but may be used for certain unilateral approaches or when combined with anterior approaches for other pelvic injuries.
-
Supine Position:
- Primarily for anterior approaches (rare for isolated sacral fractures, more common for combined anterior/posterior fixation for high transverse sacral fractures or complex pelvic ring injuries).
- Considerations: Limited access to the posterior sacrum. C-arm access is more challenging for posterior sacral views.
Intraoperative Fluoroscopy:
Crucial for all percutaneous and minimally invasive techniques. Ensure the C-arm can obtain adequate inlet, outlet, and lateral views of the sacrum and SI joints. Pre-operative acquisition of reference images with the C-arm in position on the patient can save time and reduce radiation exposure during the case.
Detailed Surgical Approach / Technique
The surgical management of sacral fractures aims to reduce displacement, decompress neural elements, and restore spinopelvic stability. The choice of technique is dictated by the AOSpine classification (morphology and instability pattern) and the presence of neurological deficits.
General Principles
- Reduction: Achieve anatomic or near-anatomic reduction of displaced fracture fragments and the pelvic ring.
- Decompression: Address any compression of sacral nerve roots or the cauda equina if neurological deficits are present or progressive.
- Stabilization: Provide rigid internal fixation to maintain reduction and allow for early mobilization.
Surgical Approaches and Fixation Techniques
1. Percutaneous Iliosacral (IS) Screw Fixation
- Indications: Primarily for AOSpine Type B fractures (unilateral longitudinal) and select C1/C2 fractures (bilateral longitudinal) without significant S1 body comminution or L5-S1 facet injury. Also used for SI joint disruption.
- Advantages: Minimally invasive, lower infection risk, less blood loss, faster recovery compared to open approaches.
-
Technique (Prone Position):
- Incision: Small stab incision over the posterior superior iliac spine (PSIS) or slightly medial/lateral depending on planned screw trajectory.
-
Reduction:
- For vertical shear injuries, reduction maneuvers can include longitudinal traction with a femoral traction pin or external fixator.
- Direct reduction via a posterior approach may be required in some cases (e.g., using a pointed reduction clamp or a Schanz pin as a joystick).
- Indirect reduction is often achieved by simply correcting the rotational and vertical malalignment of the hemipelvis.
-
Guidewire Placement (S1 and S2 trajectories):
-
S1 Trajectory:
Most common. The entry point is typically at or slightly inferior and lateral to the PSIS. The guidewire is advanced under fluoroscopic guidance (inlet, outlet, and lateral views).
- Inlet View: The wire should be directed from the posterior ilium across the SI joint into the S1 body, aiming at the junction of the S1 body and ala. Avoid anterior cortex perforation and nerve roots.
- Outlet View: The wire should be aimed towards the sacral promontory, avoiding penetration of the anterior sacral cortex and major vascular structures.
- Lateral View: The wire should be centered within the S1 vertebral body, anterior to the S1 dorsal foramen and posterior to the S1 anterior cortex.
- S2 Trajectory: May be used in conjunction with S1 screws for additional stability, or if S1 trajectory is compromised. The entry point is inferior to the PSIS, aiming for the S2 body. Similar fluoroscopic views are critical.
-
S1 Trajectory:
Most common. The entry point is typically at or slightly inferior and lateral to the PSIS. The guidewire is advanced under fluoroscopic guidance (inlet, outlet, and lateral views).
- Screw Insertion: Once guidewire position is confirmed in all three views, the bone is cannulated, measured, and a cannulated screw (typically 7.0-8.0 mm partially threaded) is inserted. Bicortical purchase across the S1 body into the contralateral ala (trans-sacral-iliac screw) provides superior stability for U-type or bilateral fractures.
- Risks: Iatrogenic S1 or L5 nerve root injury, superior gluteal artery injury (especially with superior placement), anterior cortex perforation, loss of reduction during screw insertion.
2. Lumbopelvic Fixation (LPF) / Spinopelvic Fixation
- Indications: Gold standard for AOSpine Type C fractures, particularly spinopelvic dissociation (C3, U-type fractures, H-type fractures), severe L5-S1 facet injuries (C0), or highly unstable bilateral sacral fractures (C1, C2) with S1 body comminution. Also indicated for high transverse sacral fractures causing sacral kyphosis.
- Advantages: Provides rigid fixation, restores spinopelvic alignment, and facilitates nerve decompression.
-
Technique (Prone Position):
- Incision: Midline posterior incision extending from L4/L5 to the sacrum, exposing the posterior elements of L4, L5, and the sacrum.
- Exposure: Subperiosteal dissection of the L4-L5 posterior elements and the posterior ilium to expose the PSIS and a portion of the iliac crest.
- Decompression (if needed): If neurological deficit is present and confirmed to be from direct compression (e.g., from a displaced S1 body fragment or lamina), a formal laminectomy and/or foraminotomy may be performed. This is often done prior to fixation.
- L5 Pedicle Screw Placement: Pedicle screws are inserted into L5 (and sometimes L4) bilaterally using standard freehand or navigated techniques.
-
Iliac Screw Placement (Galveston/Sacral Alar-Iliac (S2AI) Screws):
- Entry Point: Typically medial to the PSIS for S2AI, or along the inner table of the ilium for traditional Galveston.
- Trajectory (S2AI): The guidewire/screw is directed anteriorly, inferiorly, and laterally along the inner cortical surface of the ilium, aiming towards the anterior inferior iliac spine (AIIS). Avoid breach of the outer cortex, greater sciatic notch, and SI joint. S2AI screws are preferred as they allow for a more medial entry, reducing soft tissue prominence and irritation.
- Length: Screws should be long enough to achieve good purchase within the ilium (typically 70-100 mm).
- Reduction: After placing L5 pedicle screws and bilateral iliac screws, reduction of the sacral fracture (if necessary) and restoration of spinopelvic alignment can be achieved using rods. Temporary reduction clamps, joysticks, or specific reduction instruments may be used. For U-type fractures, the sacrum is often reduced by cantilever forces applied via the rods, restoring its sagittal contour.
- Rod Placement: Contoured rods connect the L5 pedicle screws to the iliac screws, creating a stable construct across the L5-S1 junction and the SI joints. Additional connectors may be used between L5 pedicle screws.
- Compression/Distraction: Apply appropriate compression or distraction to further stabilize the construct and restore lordosis/alignment.
- Bone Graft: Autograft or allograft may be placed at decorticated bone surfaces to promote fusion, although this is secondary to mechanical stability.
- Closure: Meticulous layered closure.
- Risks: Extensive soft tissue dissection, higher blood loss, increased infection risk, iliac screw prominence, superior gluteal neurovascular bundle injury, L5 nerve root injury.
3. Anterior Fixation
- Indications: Very limited for isolated sacral fractures. Occasionally used for direct reduction and plating of high transverse sacral fractures (C3 variants) in combination with posterior fixation.
- Approach: Open retroperitoneal approach (e.g., L5-S1 anterior approach).
- Risks: Major vessel injury, visceral injury, sympathetic nerve injury (retrograde ejaculation).
4. Transverse Sacral Fracture Fixation (often C3)
- Posterior Tension Band Plating/Wiring: For transverse fractures (AOSpine C3, or high Type A3) especially if there is significant kyphotic deformity. Plates are contoured across the posterior sacral elements.
- Lumbopelvic Fixation: As described above, this is often the most robust option for high transverse fractures leading to spinopelvic dissociation.
5. Open Direct Reduction and Plating
- Indications: Selected cases of Type B or C fractures with large, displaceable fragments amenable to direct visualization and plating, particularly when percutaneous options are not feasible or when decompression is required.
- Approach: Posterolateral approach, extending from the iliac crest to expose the sacrum and SI joint.
- Technique: Direct reduction using clamps, followed by screw fixation or plate osteosynthesis (e.g., SI plates).
- Risks: Greater soft tissue dissection, bleeding, infection.
Complications & Management
Sacral fracture management, whether operative or non-operative, carries significant risks. A comprehensive understanding of potential complications and their management is crucial.
Common Complications and Management Strategies
| Complication | Incidence (%) | Management / Salvage Strategies |
|---|---|---|
| Neurological Injury | 10-40% (pre-existing); 2-10% (iatrogenic) |
Prevention:
Meticulous pre-operative planning, precise guidewire/screw placement under fluoroscopy/navigation, intraoperative neuromonitoring (SSEP, EMG) for high-risk cases.
Management: Post-op neurological deficits warrant immediate investigation (CT/MRI) to rule out hardware impingement or hematoma. Urgent hardware removal/revision or decompression if indicated. Steroids for acute injury. Rehabilitative therapy. |
| Infection | 2-15% (deep); higher in open fractures or extensive LPF |
Prevention:
Strict aseptic technique, prophylactic antibiotics, careful tissue handling, meticulous wound closure, minimize operative time, negative pressure wound therapy for high-risk wounds.
Management: Superficial infections - local wound care, oral antibiotics. Deep infections - surgical debridement, IV antibiotics, possibly hardware removal (after fracture healing) or implant exchange. |
| Malunion / Nonunion | 5-15% |
Prevention:
Rigid fixation, anatomical reduction, bone grafting if indicated, protected weight-bearing.
Management: Symptomatic malunion/nonunion - revision surgery with osteotomy, reduction, and more stable fixation. Potentially bone grafting with biological augmentation. Asymptomatic - observation. |
| Hardware Failure | 5-20% (loosening, breakage, pullout) |
Prevention:
Proper screw size and length, bicortical purchase, robust construct (e.g., bilateral IS screws, lumbopelvic fixation for C-type fractures), appropriate patient weight-bearing restrictions.
Management: Symptomatic failure - revision surgery with stronger fixation, larger implants, or alternative fixation methods. Asymptomatic - observation (rarely). |
| Vascular Injury | Rare (<1%), but potentially life-threatening |
Prevention:
Thorough pre-operative imaging (CT-A), careful drilling/screw placement (esp. for anterior perforation risk), awareness of anatomical landmarks (superior gluteal artery).
Management: Urgent surgical exploration and repair by a vascular surgeon. Angioembolization for contained hematomas. |
| Pain (persistent) | Up to 30-50% |
Prevention:
Adequate reduction and stable fixation, addressing neurological compromise, appropriate post-operative rehabilitation.
Management: Multimodal pain management, physical therapy, nerve blocks, psychological support. Rule out hardware irritation or nonunion. Hardware removal if related. |
| Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) | 5-20% (DVT); 1-5% (PE) |
Prevention:
Pharmacological prophylaxis (LMWH, fondaparinux), mechanical prophylaxis (SCDs, IPC), early mobilization.
Management: Anticoagulation (therapeutic). IVC filter for recurrent PE or contraindication to anticoagulation. |
| Iliac Screw Prominence/Irritation | 5-10% (for LPF) |
Prevention:
Medial entry point (S2AI technique), proper screw length, low-profile hardware.
Management: Symptomatic hardware removal after fracture healing is complete. |
| Bladder/Rectal Injury | Rare (<1%), higher with open fractures |
Prevention:
Awareness of anterior anatomy, careful dissection, urological consultation for suspected injury.
Management: Primary repair by general or urological surgeon, appropriate drainage (suprapubic cystostomy), bowel diversion (colostomy) if needed. |
General Management Principles for Complications
- Early Detection: Vigilant post-operative monitoring for signs of neurological deterioration, infection, or wound issues.
- Prompt Investigation: Utilize appropriate imaging (X-ray, CT, MRI) to confirm the nature and extent of the complication.
- Aggressive Management: Do not delay intervention for critical complications like neurological compromise or sepsis.
- Multidisciplinary Approach: Collaborate with neurology, infectious disease, vascular surgery, and rehabilitation specialists as needed.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is integral to achieving optimal functional outcomes following sacral fracture fixation. The protocol must be tailored to the patient's age, comorbidities, fracture stability, and type of fixation.
Immediate Post-Operative Period (Day 0-7)
- Pain Management: Implement a multimodal analgesia regimen (opioids, NSAIDs, acetaminophen, nerve blocks) to control pain and facilitate early mobilization.
- Wound Care: Meticulous wound care. Monitor for signs of infection or dehiscence.
- DVT/PE Prophylaxis: Continue pharmacological and mechanical prophylaxis.
-
Early Mobilization:
- Stable Fixation (e.g., well-fixed IS screws for Type B, or robust LPF for Type C): Generally, protected weight-bearing (toe-touch or partial weight-bearing) is initiated immediately or within the first few days, using assistive devices (walker, crutches).
- Less Stable Fixation or Patient Factors: Some surgeons may opt for non-weight-bearing for 4-6 weeks in cases of marginal fixation, severe comminution, or patient non-compliance.
- Bed Mobility: Instruct on safe log-rolling for position changes to maintain spinal and pelvic alignment.
-
Physical Therapy (PT) Initiation:
- Transfers: Practice safe bed-to-chair transfers.
- Gait Training: Initiate gait training with appropriate weight-bearing restrictions.
- Gentle Range of Motion (ROM): Begin gentle lower extremity ROM exercises within pain limits.
Subacute Phase (Weeks 2-12)
- Progressive Weight-Bearing: Gradually increase weight-bearing as tolerated, guided by pain and radiographic signs of healing. This progression typically occurs between 6-12 weeks, contingent on fracture stability and the fixation construct.
-
Strengthening:
- Core Stability: Focus on deep abdominal and paraspinal muscle strengthening (pelvic tilts, bridging, gentle planks).
- Lower Extremity Strengthening: Exercises for hip abductors, adductors, quadriceps, and hamstrings.
- Flexibility/Stretching: Address any muscle tightness in the hips, hamstrings, and lower back.
- Balance Training: Begin proprioceptive and balance exercises.
- Activity Modification: Avoid high-impact activities, heavy lifting, or activities that place excessive shear stress across the SI joints.
- Bracing (Optional): A sacral or lumbosacral orthosis (LSO) may be used for patient comfort, proprioceptive feedback, or to reinforce adherence to weight-bearing restrictions, particularly in patients with less robust fixation or concerns for compliance.
Long-Term Rehabilitation (Months 3-12+)
- Return to Full Activity: Gradual return to activities of daily living (ADLs), work, and recreational activities. This transition is guided by clinical stability, absence of pain, and radiographic evidence of fracture union.
- Advanced Strengthening: Progress to more challenging functional exercises, sport-specific training if applicable.
- Endurance Training: Cardiovascular conditioning.
- Addressing Chronic Pain: If persistent pain is an issue, consider further investigation for nonunion, hardware irritation, or neuropathic pain. Referral to a pain management specialist may be appropriate.
- Education: Educate patients on body mechanics, posture, and strategies to prevent re-injury.
- Hardware Removal: In symptomatic patients, hardware removal may be considered after complete fracture healing (typically 12-18 months post-op), particularly for prominent iliac screws.
Summary of Key Literature / Guidelines
The evolution of sacral fracture classification and management has been driven by a growing body of literature emphasizing biomechanical understanding, refined surgical techniques, and improved functional outcomes.
- AOSpine Classification Validation: Studies by Vaccaro et al. (2016), Bellabarba et al. (2016), and others have validated the reliability and reproducibility of the AOSpine Sacral Fracture Classification system, demonstrating its utility in guiding surgical decision-making and predicting outcomes. This system has been shown to have higher inter- and intra-observer reliability compared to older systems like Denis and Isler.
- Spinopelvic Fixation for Instability: The literature strongly supports lumbopelvic fixation (LPF), particularly using S2AI screws, as the most stable construct for sacral spinopelvic dissociation (AOSpine C3 fractures) and highly unstable bilateral sacral fractures. Studies have consistently demonstrated its superior biomechanical stability compared to isolated iliosacral screw fixation for these complex injuries.
- Iliosacral Screws: Percutaneous iliosacral (IS) screw fixation remains the workhorse for unilateral unstable sacral fractures (AOSpine Type B) and stable bilateral patterns (AOSpine C1, C2 without significant S1 body involvement). Its minimally invasive nature and high union rates are well-documented. However, the importance of accurate trajectory to prevent iatrogenic nerve and vessel injury is constantly emphasized.
- Neurological Decompression: Prompt surgical decompression for sacral fractures with progressive neurological deficits, especially cauda equina syndrome, is widely advocated. While the degree of neurological recovery can be variable, early decompression is considered essential to maximize potential for improvement and prevent further deterioration.
- Fragility Fractures of the Sacrum (FFS): With the aging population, FFS is increasingly recognized. The AOSpine classification is being adapted to include specific FFS patterns. Management often involves a spectrum from conservative care to minimally invasive fixation (e.g., IS screws) or cement augmentation (sacroplasty), with surgical fixation gaining traction for displaced or unstable patterns. Studies highlight the challenge of diagnosing FFS, often requiring MRI for confirmation.
- Multidisciplinary Approach: Consensus guidelines from trauma and orthopedic societies consistently stress the importance of a multidisciplinary approach for complex sacral fractures, involving trauma surgeons, neurosurgeons, urologists, vascular surgeons, and rehabilitation specialists, especially in polytrauma settings.
- Complication Avoidance: Ongoing research focuses on improving navigation techniques (fluoroscopy, CT-navigation, robotic assistance) to minimize iatrogenic complications, particularly neurological and vascular injuries, during screw placement.
In summary, current guidelines emphasize a classification-driven approach to sacral fracture management, advocating for tailored surgical techniques based on the fracture's morphology, stability, and neurological status. The AOSpine system provides a robust framework for this decision-making process, aiming to standardize care and optimize patient outcomes. Continuous advancements in imaging, surgical techniques, and rehabilitation protocols continue to refine the management paradigm for these challenging injuries.
You Might Also Like

