Aarticular Part Subgroup Fractures: Key Decisions for Optimal Care
Key Takeaway
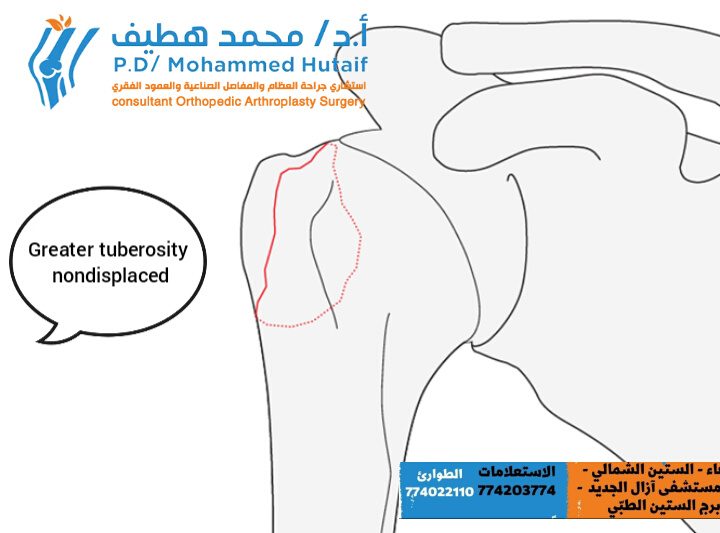
Learn more about Aarticular Part Subgroup Fractures: Key Decisions for Optimal Care and how to manage it. The "aarticular part subgroup" of proximal humerus fractures includes several types: non-displaced greater tuberosity fractures, healing well conservatively; displaced greater tuberosity fractures, often requiring surgery if displacement exceeds 5mm; tuberosity fractures associated with glenohumeral dislocations; and stable surgical neck fractures with impaction, typically managed conservatively.
Introduction & Epidemiology
Fractures of the proximal humerus constitute approximately 4-5% of all adult fractures, with a bimodal distribution peaking in young males involved in high-energy trauma and elderly osteoporotic females sustaining low-energy falls. Within this broad category, fractures of the greater tuberosity (GT) represent a distinct and clinically significant subgroup of extra-articular proximal humerus fractures, accounting for roughly 15-20% of all proximal humerus fractures. While often described as Neer two-part fractures, their unique anatomical location and functional implications warrant focused attention.
The greater tuberosity serves as the critical insertion site for the supraspinatus, infraspinatus, and often the superior aspect of the teres minor tendons, collectively comprising a significant portion of the rotator cuff. Its integrity is paramount for effective shoulder abduction, external rotation, and overall glenohumeral kinematics. Consequently, any significant displacement of a greater tuberosity fragment can lead to mechanical impingement against the coracoacromial arch, disruption of the rotator cuff's moment arm, and subsequent functional disability, pain, and potentially debilitating rotator cuff arthropathy if left unaddressed.
Initial assessment often involves standard radiographic series including anterior-posterior (AP), scapular Y, and axillary views. However, the true extent of displacement, comminution, and articular involvement can be underestimated on plain radiographs, necessitating computed tomography (CT) scans for definitive evaluation. Magnetic resonance imaging (MRI) may be indicated if there is a strong suspicion of concomitant rotator cuff tears or biceps tendon pathology, particularly in the setting of chronic or complex presentations.
A critical delineation in the management of greater tuberosity fractures is based on the degree of fragment displacement. Fractures with minimal or no displacement, typically defined as less than 5 mm, generally respond favorably to non-operative management due to their inherent stability and rich vascular supply. However, superior, posterior, or combined posterosuperior displacement exceeding this 5 mm threshold is widely considered significant and often necessitates surgical intervention to restore anatomical alignment, optimize rotator cuff function, and mitigate the risk of chronic pain and impingement. This distinction guides the fundamental decision-making process for optimal patient care.
Surgical Anatomy & Biomechanics
Surgical Anatomy
The greater tuberosity is a prominent bony projection located on the lateral aspect of the humeral head, superior and lateral to the bicipital groove. It forms the most superior and lateral extent of the proximal humerus. Its intricate anatomy is directly related to its critical function as the primary insertion site for the majority of the rotator cuff musculature.
-
Facets:
The greater tuberosity is traditionally described as having three distinct facets for rotator cuff tendon insertion:
- Superior facet: Receives the insertion of the supraspinatus tendon. This is the most superior aspect and crucial for abduction.
- Middle facet: Receives the insertion of the infraspinatus tendon. Important for external rotation.
-
Inferior facet:
Receives the insertion of the teres minor tendon. Also contributes to external rotation.
The precise arrangement is often described as a "footprint" rather than distinct linear insertions, with significant interdigitation of fibers.
- Relationship to Humeral Head: The greater tuberosity is contiguous with the humeral head's articular cartilage anteriorly and superiorly. While traditionally classified as extra-articular, severe comminution or avulsion patterns can occasionally involve a small portion of the articular margin, impacting reduction goals.
- Bicipital Groove: Located medially to the greater tuberosity, separating it from the lesser tuberosity. The long head of the biceps tendon (LHBT) courses within this groove, enclosed by the transverse humeral ligament. Greater tuberosity fractures can be associated with LHBT subluxation or dislocation, or rupture of the transverse humeral ligament.
- Vascularity: The proximal humerus receives its primary vascular supply from the anterior and posterior circumflex humeral arteries, which form an anastomotic ring around the surgical neck. Branches, notably the arcuate artery (ascending branch of the anterior circumflex humeral artery) and branches from the posterior circumflex humeral artery, supply the humeral head and tuberosities. While the greater tuberosity generally has a robust blood supply, severe displacement or extensive soft tissue stripping during surgical approaches must be considered to avoid devascularization of smaller fragments.
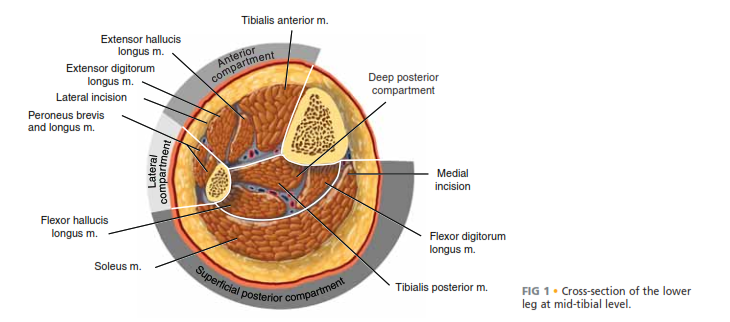
- Neurological Considerations: The axillary nerve is a critical structure that courses circumferentially around the surgical neck of the humerus, approximately 5-7 cm distal to the acromion. It innervates the deltoid and teres minor muscles. Damage to the axillary nerve can occur during surgical exposure, particularly with deltoid-splitting approaches that extend too distally, or due to aggressive manipulation. Other nerves, such as the musculocutaneous and radial nerves, are generally at lower risk but must be respected during surgical dissection.
Biomechanics
The functional integrity of the greater tuberosity is paramount for normal shoulder biomechanics, primarily due to its role as the attachment point for the rotator cuff.
- Rotator Cuff Function: The supraspinatus initiates and contributes significantly to abduction. The infraspinatus and teres minor are primary external rotators. Avulsion of the greater tuberosity effectively detaches these critical force vectors from the humerus.
-
Displacement Mechanisms:
The strong musculotendinous pull of the rotator cuff is the primary driver of fracture displacement.
- Supraspinatus: Causes superior migration of the fragment.
- Infraspinatus/Teres Minor: Cause posterior migration of the fragment, often in conjunction with superior displacement, leading to the classic posterosuperior displacement pattern.
- These forces can lead to significant retraction of the fragment, making closed reduction challenging and often necessitating open reduction.
- Impingement: A displaced greater tuberosity fragment, particularly when superiorly or posterosuperiorly displaced, can mechanically impinge on the coracoacromial arch (acromion, coracoacromial ligament, coracoid). This impingement during abduction and elevation directly causes pain and restricts range of motion.
- Rotator Cuff Mechanics: Displacement of the greater tuberosity alters the length-tension relationship of the attached rotator cuff tendons, diminishing their mechanical advantage. Even small amounts of proximal displacement can shorten the rotator cuff tendon-muscle unit, leading to muscle weakness and dysfunction. The 5 mm displacement threshold is clinically significant because beyond this point, the mechanical efficiency of the rotator cuff is noticeably compromised, and the risk of impingement increases substantially.
- Articular Impact: While extra-articular, significant superior displacement can lead to the GT fragment abutting the glenoid articular surface during abduction, further impeding motion and potentially causing chondral damage over time.
Understanding these anatomical relationships and biomechanical forces is critical for guiding both surgical approach and reduction/fixation strategies, aiming to restore the anatomical footprint of the rotator cuff and optimize shoulder function.
Indications & Contraindications
The decision-making process for greater tuberosity fractures hinges on a thorough evaluation of fracture characteristics, patient factors, and potential comorbidities. The primary goal is to restore the anatomical position of the tuberosity to optimize rotator cuff function and prevent impingement.
Non-Operative Indications
Non-operative management is typically favored for fractures that are inherently stable and unlikely to lead to long-term functional deficits.
-
Non-Displaced or Minimally Displaced Fractures:
This subgroup comprises fractures of the greater tuberosity which are truly not displaced, or displaced by less than 5 mm.
-
 - These fractures typically heal very well under conservative treatment and do not tend to displace further during the healing period.
- The integrity of the rotator cuff's origin is preserved, minimizing the risk of impingement or significant functional compromise.
- Careful radiographic follow-up is essential to detect any delayed displacement.
-
- Elderly, Low-Demand Patients: Individuals with significant comorbidities or low functional expectations, where the risks associated with surgery (anesthesia, infection, hardware complications) may outweigh the potential benefits of operative fixation.
- Medically Unfit Patients: Patients with severe, uncontrolled medical conditions (e.g., severe cardiac or pulmonary disease, uncontrolled diabetes) that preclude safe surgical intervention.
Operative Indications
Surgical intervention is generally recommended when there is a high likelihood of functional impairment, pain, or mechanical instability with non-operative management.
-
Displaced Fractures:
Displacement of the greater tuberosity fragment exceeding 5 mm in any plane (superior, posterior, or combined posterosuperior).
-
 - The typical displacement of the greater tuberosity is posterosuperiorly. A displacement more than 5 mm is usually considered significant and should be treated surgically to prevent impingement and restore rotator cuff function.
-
-
Associated Injuries:
- Glenohumeral Dislocation: When the greater tuberosity fracture is associated with an irreducible glenohumeral dislocation, or if the fragment itself blocks reduction.
- Rotator Cuff Tear: If there is a concomitant full-thickness rotator cuff tear that warrants repair.
- Long Head Biceps Tendon Instability: Fractures extending into the bicipital groove causing instability of the LHBT.
- Young, Active Patients: In active individuals where restoration of optimal shoulder function is a high priority, even borderline displacement may prompt surgical consideration.
- Open Fractures: Although rare for isolated greater tuberosity fractures, any open fracture warrants surgical debridement and fixation.
- Progressive Displacement: Documented progression of displacement during non-operative treatment, indicating instability.
Contraindications
-
Absolute Contraindications:
- Severe, life-threatening medical comorbidities that render the patient unfit for surgery.
- Active local or systemic infection.
- Non-reconstructible bone loss or severe comminution that precludes stable fixation.
-
Relative Contraindications:
- Extremely poor bone quality (severe osteoporosis) that may not provide adequate purchase for fixation, necessitating careful implant selection.
- Extensive soft tissue compromise or devitalization.
- Patient non-compliance with post-operative rehabilitation.
Table: Operative vs. Non-Operative Indications for Greater Tuberosity Fractures
| Factor | Non-Operative Management | Operative Management |
|---|---|---|
| Displacement | < 5 mm in any plane (non-displaced or minimally displaced) | > 5 mm in any plane (superior, posterior, or posterosuperior) |
| Associated Injuries | Isolated fracture, stable joint | Irreducible glenohumeral dislocation, significant concomitant rotator cuff tear, LHBT instability |
| Patient Age/Demand | Elderly, low-demand, sedentary lifestyle | Young, active, high-demand, athletes |
| Comorbidities | Significant comorbidities increasing surgical risk | Medically fit, manageable comorbidities |
| Bone Quality | Adequate for healing without surgical intervention | Adequate for implant purchase and stable fixation |
| Fracture Stability | Stable, no progressive displacement on follow-up | Unstable, progressive displacement, or unable to achieve/maintain reduction |
| Open Fracture | N/A | All open fractures |
Pre-Operative Planning & Patient Positioning
Pre-Operative Planning
Meticulous pre-operative planning is crucial to anticipate potential challenges and optimize surgical outcomes.
-
Comprehensive Imaging Review:
- Plain Radiographs: AP, scapular Y, and axillary views are standard. Evaluate the degree and direction of displacement, comminution, and any associated glenohumeral dislocation.
- Computed Tomography (CT) Scan: Essential for a detailed three-dimensional understanding of the fracture pattern. It accurately quantifies displacement (both superior and posterior), assesses comminution of the tuberosity, identifies subtle articular involvement, and aids in surgical approach and implant selection. This is particularly important for differentiating between truly non-displaced fractures and those with subtle displacement that may not be apparent on plain films.
- Magnetic Resonance Imaging (MRI): Consider if there is suspicion of concomitant rotator cuff pathology (pre-existing tear, extension of the avulsion to a larger cuff tear), biceps tendon pathology, or capsular injury, especially in younger patients or those with high-energy mechanisms.
-
Patient Assessment:
- Medical History: Thorough review of comorbidities (cardiac, pulmonary, endocrine, neurological), allergies, and current medications (especially antiplatelets/anticoagulants which may need to be adjusted).
- Functional Assessment: Pre-injury activity level, hand dominance, and patient expectations.
- Physical Examination: Document neurological status (deltoid innervation, axillary nerve function), vascular status, and any pre-existing shoulder pathology.
-
Implant Selection:
Based on the fracture pattern, bone quality, and surgeon preference. Options include:
- Suture anchors (for smaller, comminuted fragments or poor bone quality).
- Transosseous sutures.
- Cannulated screws (for larger, single fragments).
- Proximal humerus locking plates (less common for isolated GT but may be used for specific patterns or associated fractures).
- Consider availability of specific GT fixation systems.
- Surgical Approach Planning: Determine the most appropriate surgical approach (deltopectoral vs. anterosuperior/deltoid-splitting) based on the vector of displacement and desired access.
- Contingency Planning: Anticipate potential difficulties such as poor bone quality, difficulty achieving reduction, or presence of larger rotator cuff tears requiring extensive repair. Prepare for alternative fixation strategies or adjunctive bone graft if necessary.
Patient Positioning
The choice of patient position significantly impacts surgical exposure, intraoperative fluoroscopy, and surgeon comfort.
-
Beach Chair Position:
- Advantages: Excellent visualization of the anterior and superior shoulder. Allows for easy conversion to arthroscopy if indicated. Gravity assists in retracting the humerus inferiorly for better exposure. Fluoroscopy (AP and axillary views) is generally straightforward.
- Disadvantages: Potential for hypotension (head-up position), brachial plexus traction injury, and difficult posterior access if needed.
- Setup: Patient is positioned semi-recumbent at 45-70 degrees. The head is stabilized in a headrest (e.g., 'Mayfield' type or donut). The torso is supported. The operative arm is draped free or placed on an arm board. Ensure adequate padding at pressure points and neurovascular structures. The patient's hips should be at the break in the table to allow for slight trendelenburg if needed.
-
Lateral Decubitus Position:
- Advantages: Provides good access to both anterior and posterior aspects of the shoulder. Less risk of hypotension. Often preferred if an arthroscopic approach is combined or if greater posterior access is anticipated.
- Disadvantages: Requires more extensive draping and positioning for fluoroscopy. Can be challenging to maintain stable arm position for open reduction.
- Setup: Patient is positioned on their non-operative side. Axillary roll placed to protect the neurovascular bundle. Ipsilateral hip and knee are flexed. The operative arm is suspended in traction, typically with 10-15 lbs, often using a traction tower, allowing for controlled manipulation. Ensure adequate padding of all pressure points.
Fluoroscopy Setup: Regardless of positioning, ensure a clear fluoroscopic image can be obtained in at least two orthogonal planes (AP and axillary/Y-view) without repositioning the patient or C-arm significantly. The C-arm should be pre-draped and positioned for ease of use.
Detailed Surgical Approach / Technique
The primary surgical goal is anatomical reduction of the greater tuberosity fragment(s) and stable fixation, allowing for early controlled motion and restoration of rotator cuff mechanics.
General Principles
- Anatomic Reduction: Crucial for restoring the rotator cuff footprint and preventing impingement.
- Stable Fixation: Must be robust enough to withstand early rehabilitation forces.
- Preservation of Vascularity: Minimize soft tissue stripping, especially from the rotator cuff attachments to the fragment.
- Careful Neurovascular Dissection: Protect the axillary nerve and other vital structures.
Surgical Approach
The choice of approach depends on the fracture morphology, displacement, and surgeon's preference.
-
Anterosuperior (Deltoid-Splitting) Approach:
- Indications: Ideal for isolated greater tuberosity fractures with superior or posterosuperior displacement. Provides direct access to the tuberosity.
- Incision: A curvilinear incision is made from the anterior aspect of the acromion, extending distally approximately 5-7 cm.
- Dissection: The deltoid muscle fibers are carefully split longitudinally in line with their fibers.
- Internervous Plane: The deltoid is supplied by the axillary nerve, which enters its deep surface 5-7 cm distal to the acromion. Crucially, the deltoid split should not extend beyond 5 cm from the acromial border to avoid iatrogenic injury to the axillary nerve.
- Exposure: After splitting the deltoid, the rotator cuff tendons and the displaced greater tuberosity fragment are exposed. The subacromial bursa is typically opened and debrided.
-
Deltopectoral Approach:
- Indications: Useful if extensive anterior exposure is required, or if there are associated fractures of the humeral head/neck, or when conversion to arthroplasty is a possibility. Less commonly used for isolated GT fractures due to indirect access.
- Incision: A longitudinal incision is made from the coracoid process, extending distally along the deltopectoral groove.
- Dissection: The interval between the deltoid (lateral) and pectoralis major (medial) is identified. The cephalic vein typically lies within this groove and can be retracted medially with the pectoralis or laterally with the deltoid.
- Exposure: The conjoint tendon (coracobrachialis and short head of biceps) is identified and retracted medially. The anterior capsule and subscapularis tendon are then encountered. The GT fragment is accessed via a capsulotomy or by retracting the rotator interval.
Reduction Techniques
Once exposed, the greater tuberosity fragment is reduced anatomically.
-
Direct Manipulation:
- Bone hooks, K-wires (used as joysticks), or small periosteal elevators can be used to grasp and maneuver the fragment.
-
(Figure illustrating direct reduction with a hook or K-wire). - Often, the fragment is retracted superiorly and posteriorly. Traction on the rotator cuff tendons (supraspinatus, infraspinatus) can help bring the fragment distally and anteriorly.
- Soft Tissue Release: In chronic or severely retracted cases, gentle release of adhesions or scar tissue around the fragment may be necessary to facilitate reduction.
-
Visualization:
Ensure anatomical reduction by direct visualization and fluoroscopic confirmation in multiple planes (AP, Y-view, axillary). The goal is to restore the contour of the humeral head and the rotator cuff footprint.
-
(Intraoperative fluoroscopic image confirming reduction of the fragment).
-
Fixation Methods
The choice of fixation method depends on fragment size, bone quality, comminution, and surgeon experience.
-
Suture Fixation (Transosseous Sutures or Suture Anchors):
- Indications: Often preferred for smaller, more comminuted fragments, or when bone quality is poor. Mimics a rotator cuff repair by reapproximating the tendon-bone interface.
-
Technique:
Strong non-absorbable sutures (e.g., #2 FiberWire) are passed through the rotator cuff tendon attached to the fragment.
- Transosseous: Sutures are then passed through drill holes in the humeral shaft (distal to the fracture) and tied over a bony bridge or a cortical button on the medial cortex of the humerus.
- Suture Anchors: One or more suture anchors are placed into the humeral head, typically just distal to the fracture line or into the cancellous bone. The sutures from the anchors are then passed through the rotator cuff tendon attached to the fragment and tied to achieve compression and stable fixation. A "suture bridge" technique with medial and lateral anchors can provide excellent broad compression.
-
(Image demonstrating suture anchor fixation or transosseous sutures for GT fracture).
-
Screw Fixation:
- Indications: Suitable for larger, solitary, non-comminuted fragments where adequate bone stock allows for bicortical or strong unicortical purchase.
- Technique: One or two partially threaded cannulated screws (e.g., 3.5mm or 4.0mm) are typically inserted from superior or lateral to medial, engaging the cortical bone of the humeral head or medial shaft. The screws should be placed to achieve interfragmentary compression and avoid violating the articular surface. Proper screw length is critical.
-
Plate Fixation:
- Indications: Less common for isolated greater tuberosity fractures but may be considered for highly comminuted patterns, very large fragments, or in conjunction with other proximal humerus fractures requiring plate stabilization. Specific greater tuberosity plates or small fragment plates can be used.
- Technique: A small locking plate can be applied to the lateral aspect of the humerus, with locking screws engaging the greater tuberosity fragment and the humeral shaft. This offers angular stability, particularly valuable in osteoporotic bone.
-
(Illustration of screw or small plate fixation for GT fracture).
- Combined Techniques: Often, a combination of methods is employed, such as suture anchors for initial reduction and fixation of the rotator cuff, supplemented by a screw for larger bony fragments if deemed necessary for additional stability.
Intraoperative Assessment
- Fluoroscopy: Obtain AP, Y-view, and axillary fluoroscopic images to confirm anatomical reduction and satisfactory implant placement. Ensure no screws are intra-articular and that the fragment is appropriately reduced.
- Range of Motion: Carefully assess the glenohumeral range of motion to ensure no impingement of hardware or malreduced fragment, and that the fixation is stable through a physiological arc.
- Rotator Cuff Tension: Confirm that the rotator cuff is under appropriate tension without excessive gapping at the repair site.
Wound Closure
Layered closure is performed. The deltoid split (if used) is carefully reapproximated. The subcutaneous tissue and skin are closed. A sterile dressing is applied.
Complications & Management
Despite meticulous surgical technique, complications can arise, necessitating vigilant post-operative monitoring and appropriate management strategies.
Table: Common Complications, Incidence, and Management Strategies
| Complication | Incidence (Approx.) | Contributing Factors | Management/Salvage Strategy
|
Rotator Cuff Tear/Dysfunction
| 10-20% | Nonunion/malunion, residual impingement, re-tear, or associated cuff pathology | Arthroscopic debridement and/or hardware removal if impingement. Rotator cuff repair (open or arthroscopic) for symptomatic tears. Physical therapy for functional deficits. |
|
Shoulder Stiffness/Contracture
| Common (up to 30%) | Prolonged immobilization, inadequate rehabilitation, patient apprehension, pain-avoidance. | Aggressive physical therapy, potentially with MUA (Manipulation Under Anesthesia) and/or arthroscopic capsular release for refractory cases. Analgesia and anti-inflammatories. |
|
Nerve Injury
| < 5% | Iatrogenic (axillary nerve most common during deltoid split or aggressive retraction). | Observation for neurapraxia (most resolve spontaneously). EMG/NCS for diagnosis. Surgical exploration and neurolysis/repair for persistent deficits or confirmed transection. |
|
Infection
| < 2% | Poor surgical asepsis, prolonged surgery, compromised soft tissue. | Superficial: Oral antibiotics, wound care. Deep: Surgical debridement, IV antibiotics (often for 6 weeks), hardware retention if stable (less likely if septic), or removal. |
|
Hardware-Related Issues
| 5-10% | Screw cutout, prominence, migration, breakage, intra-articular placement. | Hardware removal if symptomatic (prominence, impingement). Revision fixation if failure results in loss of reduction. Revision of intra-articular hardware. |
|
Malunion
| 5-15% | Inadequate reduction or loss of reduction post-operatively. | Mild: Observation, physical therapy. Symptomatic/severe: Corrective osteotomy and refixation. Arthroscopic debridement for impingement. |
|
Nonunion
| < 5% | Inadequate fixation, severe comminution, soft tissue interposition, biological factors (e.g., smoking, poor nutrition). | Revision surgery with decortication, bone grafting (autograft or allograft), and rigid internal fixation. |
|
Adhesive Capsulitis
| 5-10% | Post-surgical inflammation, prolonged immobilization. | Physical therapy, anti-inflammatory medications, intra-articular steroid injections. MUA or arthroscopic capsular release for refractory cases. |
General Management Principles for Complications
- Early Detection: Regular clinical and radiographic follow-up is critical.
- Patient Education: Inform patients about potential complications and the importance of adhering to rehabilitation protocols.
- Conservative Management First: Many minor complications (e.g., mild stiffness, temporary paresthesias) can be managed non-surgically.
- Timely Intervention: Do not delay surgical intervention for complications that will not resolve spontaneously or are causing progressive morbidity (e.g., symptomatic hardware, progressive nonunion).
- Multidisciplinary Approach: Involve physical therapists, pain management specialists, and infectious disease specialists as needed.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a cornerstone of successful recovery after greater tuberosity fracture fixation. The protocol must be tailored to the specific fracture pattern, bone quality, stability of fixation, and patient compliance. The overarching goals are to protect the repair, restore range of motion, regain strength, and optimize functional return.
Phase I: Protection & Early Motion (Weeks 0-6)
Goals:
* Protect the healing fracture and surgical repair.
* Minimize pain and inflammation.
* Prevent shoulder stiffness (especially adhesive capsulitis).
* Maintain mobility of elbow, wrist, and hand.
Guidelines:
*
Immobilization:
Sling for comfort and protection (e.g., shoulder immobilizer). Removed for exercises and hygiene. Duration of sling use varies by surgeon, but typically 4-6 weeks for sleep and crowded environments.
*
Passive Range of Motion (PROM):
*
Pendulum Exercises:
Initiate within the first week (e.g., Codman's exercises) to encourage gentle glenohumeral motion and reduce pain.
*
Supine Passive Flexion:
Progressively increase forward flexion with assistance (e.g., using the contralateral hand or a stick) to tolerance, typically up to 90-120 degrees.
*
Supine Passive External Rotation:
With the elbow adducted, passively rotate the arm externally to neutral or 30 degrees, depending on stability and pain. Avoid active external rotation.
*
Passive Internal Rotation:
To tolerance.
*
Scapular Stabilization:
Gentle isometric scapular exercises.
*
Elbow, Wrist, Hand Exercises:
Active range of motion and grip strengthening to prevent stiffness and edema.
*
Precautions:
*
NO active abduction or external rotation against gravity.
The rotator cuff repair is still vulnerable.
* Avoid lifting, pushing, pulling with the affected arm.
* Avoid unsupported or sudden movements.
Phase II: Progressive Active Motion & Light Strengthening (Weeks 6-12)
Goals:
* Gradually restore active range of motion (AROM).
* Initiate gentle isometric and light isotonic strengthening.
* Improve shoulder proprioception and neuromuscular control.
Guidelines:
*
Active-Assisted Range of Motion (AAROM):
Progress from PROM to AAROM using pulleys, sticks, or the unaffected arm.
*
Active Range of Motion (AROM):
Gradually introduce unassisted active movements as pain permits and stability allows.
* Progressive abduction and external rotation.
*
Isometric Strengthening:
* Submaximal isometric contractions of rotator cuff (internal rotation, external rotation, abduction) and deltoid, performed in multiple directions against an immovable object (wall, therapist's hand).
* Start gently and increase intensity as tolerated.
*
Light Isotonic Strengthening:
* Begin with very light resistance bands or weights for internal/external rotation and scapular musculature.
* Focus on proper form and control.
*
Proprioception:
Wall slides, rhythmic stabilization exercises.
*
Precautions:
* Avoid heavy lifting.
* Continue to protect the repair from sudden, forceful movements.
* Progress resistance slowly and deliberately.
Phase III: Advanced Strengthening & Return to Activity (Weeks 12+)
Goals:
* Restore full strength, power, and endurance.
* Return to sport-specific or occupation-specific activities.
* Achieve maximal functional recovery.
Guidelines:
*
Progressive Resistive Exercises:
* Increase intensity and resistance for all major shoulder muscle groups (rotator cuff, deltoid, scapular stabilizers).
* Introduce multi-planar movements.
* Eccentric strengthening.
*
Functional Training:
* Incorporate exercises that mimic daily activities or sport-specific movements.
* Plyometric exercises for athletes.
* Overhead activities as tolerated, ensuring good scapulohumeral rhythm.
*
Endurance Training:
High-repetition, low-resistance exercises.
*
Return to Activity:
* Gradual return to unrestricted activities, typically between 4-6 months post-surgery, but highly dependent on individual progress, fracture healing, and functional assessment.
* For overhead athletes or those in demanding occupations, a longer return-to-play/work protocol is often necessary, sometimes extending to 9-12 months.
*
Ongoing Home Program:
Emphasize the importance of maintaining a lifelong home exercise program to prevent recurrence and maintain shoulder health.
Key Considerations for Rehabilitation
- Individualized Approach: Protocols must be flexible and adapted to the patient's pain, healing status, and progress.
- Pain as a Guide: While some discomfort is expected, sharp or increasing pain should prompt re-evaluation.
- Communication: Close collaboration between the surgeon and physical therapist is essential.
- Bone Healing: Radiographic confirmation of fracture healing is a prerequisite for advancing to heavier strengthening phases.
- Patient Compliance: Success heavily relies on the patient's adherence to the prescribed exercises and precautions.
Summary of Key Literature / Guidelines
Fractures of the greater tuberosity represent a well-studied subgroup of proximal humerus fractures, with a significant body of literature guiding treatment decisions. While classification systems like Neer provide a framework for proximal humerus fractures, isolated greater tuberosity fractures are typically classified as Neer 2-part fractures. The critical threshold for displacement has been a consistent theme in the literature.
Displacement Threshold
- Historical Context: The 5 mm displacement threshold for surgical intervention in greater tuberosity fractures is widely accepted and has been endorsed by numerous authors and consensus statements. This threshold is largely based on the biomechanical understanding that greater displacement significantly compromises rotator cuff mechanics, alters the length-tension relationship, and increases the risk of subacromial impingement.
- Biomechanical Studies: Several cadaveric and in vivo studies have demonstrated that superior or posterosuperior displacement of the greater tuberosity by more than 5 mm leads to a measurable decrease in rotator cuff efficiency and an increase in subacromial contact pressures during shoulder elevation. Some authors have even advocated for a lower threshold (e.g., 3 mm for posterior displacement) in very active patients to optimize outcomes.
- Clinical Outcomes: Retrospective and prospective studies consistently show superior functional outcomes (e.g., ASES, Constant scores) and lower rates of nonunion or symptomatic malunion in surgically treated patients with displaced (>5mm) greater tuberosity fractures compared to non-operative management.
Operative vs. Non-Operative Outcomes
- Non-displaced Fractures: The consensus remains strong for non-operative management of truly non-displaced or minimally displaced (<5mm) greater tuberosity fractures. Literature supports excellent healing rates and functional outcomes with a sling for comfort, followed by early mobilization. The risk of secondary displacement is low, making routine surgical fixation unnecessary and exposing patients to unnecessary risks.
-
Displaced Fractures:
For fragments displaced >5mm, surgical intervention has become the standard of care, particularly in younger, active individuals.
- Systematic Reviews and Meta-analyses: These have largely affirmed that surgical fixation for significantly displaced greater tuberosity fractures leads to better pain control, improved range of motion, and higher patient satisfaction compared to non-operative treatment, primarily by restoring anatomical alignment and preventing impingement.
- Controversies: While the 5mm threshold is generally accepted, some debate persists regarding the optimal treatment for "borderline" displacements (e.g., 3-5 mm), especially in less demanding or elderly patients, where the surgical risks may sometimes outweigh marginal functional gains. The discussion often shifts to shared decision-making, considering individual patient factors.
Fixation Techniques
- Suture Fixation: Transosseous sutures and suture anchors are well-established and highly effective techniques for fixing greater tuberosity fractures, particularly for smaller or comminuted fragments. They offer the advantage of broad compression of the rotator cuff footprint to the bone. Studies have shown good to excellent results with these techniques, emphasizing anatomical reduction and secure knot tying.
- Screw Fixation: Cannulated screws provide rigid fixation for larger, solitary fragments with good bone stock. The literature supports their use when applicable, with careful attention to avoid intra-articular penetration.
- Plate Fixation: While less frequently used for isolated greater tuberosity fractures, locking plates offer robust fixation in comminuted patterns or in the presence of osteopenia. Their use often extends to more complex proximal humerus fractures involving the surgical neck.
- Comparison: Head-to-head comparisons of fixation techniques are limited, but overall, the literature suggests that successful outcomes depend more on achieving and maintaining anatomical reduction and stable fixation than on the specific implant chosen, provided the implant is appropriate for the fracture pattern.
Rehabilitation Protocols
- Early Motion: Modern rehabilitation protocols emphasize early passive and active-assisted range of motion, typically initiated within the first few post-operative weeks, to prevent stiffness and improve outcomes. This is predicated on stable surgical fixation.
- Protection Phase: A period of protection (e.g., 4-6 weeks with restricted active abduction/external rotation) is consistently recommended to allow for initial biological healing of the bone-tendon interface.
- Progressive Strengthening: Gradual progression to active strengthening and functional exercises follows, with full return to strenuous activities typically at 4-6 months, though often longer for high-demand individuals.
Key Guidelines and Recommendations
- CT scan for diagnosis: Most guidelines recommend CT imaging for comprehensive evaluation of greater tuberosity fractures to accurately assess displacement and comminution.
- Surgical indication: Displaced (>5mm) greater tuberosity fractures, especially in active patients, generally warrant operative management.
- Anatomic Reduction: The paramount goal of surgery is to achieve anatomical reduction of the greater tuberosity to restore rotator cuff function and prevent impingement.
- Stable Fixation: The chosen fixation method should provide sufficient stability to allow for early controlled rehabilitation.
- Individualized Care: Patient age, activity level, comorbidities, and bone quality must always be factored into treatment decisions.
In conclusion, the current body of literature provides strong evidence for a treatment paradigm that prioritizes anatomical reduction and stable fixation for significantly displaced greater tuberosity fractures, while advocating for non-operative management of truly non-displaced injuries. The emphasis on careful pre-operative planning, meticulous surgical technique, and structured post-operative rehabilitation remains critical for optimizing long-term functional outcomes.
You Might Also Like