Volar Bone Grafting for Scaphoid Nonunion: The Stark Technique
Key Takeaway
The Stark et al. volar grafting technique is a highly effective surgical intervention for scaphoid nonunions complicated by volar cortical bone loss and humpback deformity. This procedure utilizes a volar approach to excavate fibrous nonunion tissue, correct carpal malalignment using a structural corticocancellous graft, and stabilize the construct with Kirschner wires. Precise execution restores scaphoid length, prevents dorsal intercalated segment instability (DISI), and halts the progression of scaphoid nonunion advanced collapse (SNAC).
Introduction to Scaphoid Nonunion and Grafting Operations
Scaphoid fractures account for the vast majority of carpal bone fractures, and due to the tenuous retrograde blood supply to the proximal pole, nonunion remains a formidable clinical challenge. When a scaphoid fracture fails to unite, the biomechanical uncoupling of the proximal and distal carpal rows leads to predictable and progressive carpal instability.
The Stark et al. technique for scaphoid nonunion grafting is a foundational orthopedic procedure designed to address not only the biological failure of bone healing but also the structural collapse of the scaphoid. This technique is particularly indicated when there is a deficiency of the volar cortex, a condition that permits an exaggerated volar tilt of the distal fragment, clinically recognized as the "humpback" deformity. Left untreated, this deformity alters radiocarpal kinematics, leading to Dorsal Intercalated Segment Instability (DISI) and ultimately Scaphoid Nonunion Advanced Collapse (SNAC).
This comprehensive surgical guide details the indications, biomechanical rationale, and step-by-step execution of the Stark et al. volar grafting operation, providing orthopedic surgeons with the critical insights required to restore carpal anatomy and function.
Preoperative Planning and Biomechanics
The "Humpback" Deformity
Understanding the biomechanics of the scaphoid is paramount before undertaking a grafting operation. The scaphoid acts as a stabilizing tie-rod between the proximal and distal carpal rows. In the setting of a waist fracture nonunion, the distal fragment tends to flex under the palmar pull of the scaphotrapezial-trapezoid (STT) ligaments, while the proximal fragment extends with the lunate due to the intact scapholunate interosseous ligament.
Over time, the compressive forces across the wrist cause resorption of the volar cortex at the fracture site. This volar deficiency is the primary driver of the humpback deformity. The Stark technique specifically addresses this by utilizing a structural corticocancellous graft to prop open the collapsed volar defect, thereby restoring the anatomical length and alignment of the scaphoid.
Indications for the Stark Technique
- Established scaphoid waist nonunions with volar bone loss.
- Presence of a humpback deformity (intrascaphoid angle > 35 degrees on sagittal CT).
- Delayed unions where structural support is deemed necessary to prevent collapse.
- Cases where percutaneous fixation is contraindicated due to the need for open deformity correction.
Surgical Warning:
The Stark technique relies on a viable proximal pole. If preoperative Magnetic Resonance Imaging (MRI) or intraoperative punctate bleeding assessments reveal complete avascular necrosis (AVN) of the proximal pole, a vascularized bone graft (e.g., 1,2-Intercompartmental Supraretinacular Artery [1,2-ICSRA] graft or medial femoral condyle free flap) may be more appropriate than a non-vascularized corticocancellous graft.
Patient Positioning and Preparation
- Anesthesia: The procedure is typically performed under regional anesthesia (supraclavicular or axillary brachial plexus block) or general anesthesia, depending on patient preference and the need for an iliac crest bone graft harvest.
- Positioning: The patient is placed supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mm Hg after exsanguination with an Esmarch bandage.
- Fluoroscopy: A mini C-arm is positioned perpendicular to the hand table to allow for seamless intraoperative orthogonal imaging without disrupting the surgical field.
- Graft Site Prep: If an autologous iliac crest bone graft (ICBG) is planned, the ipsilateral anterior superior iliac spine (ASIS) is prepped and draped simultaneously.
Surgical Technique: Step-by-Step (Stark et al.)
1. The Volar Surgical Approach
Expose the scaphoid through a straight or zigzag volar incision over the distal flexor carpi radialis (FCR) tendon. The incision typically extends from the distal wrist crease proximally for about 4 to 5 cm.
- Incise the superficial fascia and open the FCR tendon sheath.
- Retract the FCR tendon ulnarly to protect the median nerve.
- Identify and protect the palmar cutaneous branch of the median nerve, which lies in the subcutaneous tissue ulnar to the FCR.
- Incise the floor of the FCR sheath to expose the underlying volar wrist capsule.
2. Capsulotomy and Exposure
After the wrist capsule is incised longitudinally, the critical radiocarpal ligaments (radioscaphocapitate and long radiolunate ligaments) are carefully retracted or split in line with their fibers.
Once the capsule is open, the wrist is dorsiflexed over a rolled towel. This maneuver brings the volar aspect of the scaphoid directly into the surgical field. Both parts of the scaphoid (proximal and distal fragments) and the articular surface of the radius can be seen readily.
3. Debridement and Excavation of the Nonunion
The nonunion site is often obscured by dense fibrous tissue and sclerotic bone margins.
- Remove a small, rectangular window of bone from the volar aspect of the distal fragment immediately adjacent to the fracture.
- Through this opening, clear fragments of fibrous tissue and dead bone. It is imperative to use a low-speed power burr or a sharp curet. High-speed burrs without adequate irrigation can cause thermal necrosis, further compromising the already tenuous biology of the scaphoid.

- Fashion a large cavity in the proximal and distal parts of the scaphoid. The goal is to expose healthy, bleeding cancellous bone in both fragments ("paprika sign"). The cavity should be geometrically prepared to accept a rectangular corticocancellous strut graft.
4. Deformity Correction and Joint Protection
The volar part of the cortex of the scaphoid often is deficient, and this deficiency permits an exaggerated volar tilt of the distal fragment, creating the “humpback” deformity of the scaphoid. Realignment and reduction of the fracture and restoration of the bone to the proper length are the most difficult parts of the procedure.
To achieve this, use a Chandler retractor to protect the articular cartilage of the radioscaphoid joint. The retractor is carefully inserted between the scaphoid and the radial styloid.

Clinical Pearl:
The Chandler retractor serves a dual purpose. Not only does it shield the pristine articular cartilage of the radius from the burr and curettes, but it also acts as a powerful lever. By applying gentle leverage, the surgeon can pry open the collapsed volar defect, correcting the angulation, malrotation, and displacement of the fragments.
Intraoperative radiographs (fluoroscopy) usually are necessary at this stage to confirm that the humpback deformity has been corrected, the intrascaphoid angle is restored to near zero, and the dorsal intercalated segment instability (DISI) posture of the lunate has been reduced.
5. Graft Harvesting and Insertion
Once the cavity is prepared and the deformity is corrected, the defect size is measured. A corticocancellous bone graft is harvested, typically from the anterior iliac crest, as it provides excellent structural integrity and rich osteogenic potential. Alternatively, distal radius autograft can be used if the defect is small, though it offers less structural support.
- The graft is fashioned into a wedge or rectangular strut, matching the dimensions of the excavated cavity.
- The cortical portion of the graft is oriented volarly to replace the deficient volar cortex and maintain the corrected length and alignment of the scaphoid.
- The cancellous portion of the graft is packed deeply into the excavated cavity to promote rapid osteointegration.

Carefully impact the cortical graft into the cavity while maintaining the reduction. The structural graft acts as a mechanical block, preventing the distal pole from collapsing back into flexion. Supplemental cancellous graft can be packed around the margins of the strut to fill any remaining voids.
6. Kirschner Wire Fixation
While modern variations of scaphoid nonunion surgery often utilize headless compression screws, the classic Stark technique relies on precise Kirschner wire (K-wire) fixation. K-wires are highly effective, minimize the risk of displacing the carefully positioned graft, and avoid the removal of additional bone stock required by screw tracks.
- Transfix the scaphoid with two 0.035-inch (0.9-mm) Kirschner wires.
- Insert them through the distal fragment, passing them across the graft and into the proximal fragment.
- During insertion, continuously protect the articular cartilages of the scaphoid and radius with the Chandler retractor.
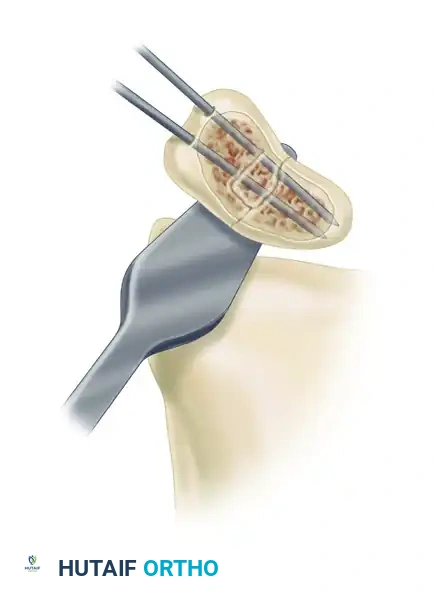
To ensure maximum stability of the construct, a third Kirschner wire may be inserted directly through the cortical bone graft to stabilize the graft itself within the scaphoid cavity, preventing extrusion or micromotion.

Surgical Pitfall:
Ensure that the K-wires do not penetrate the proximal articular surface of the scaphoid. Penetration into the radiocarpal or midcarpal joints will cause severe cartilage abrasion and early osteoarthritis. Confirm wire placement with multiple fluoroscopic views (PA, lateral, pronated oblique, and supinated oblique) before cutting the wires.
The K-wires are typically cut beneath the skin to prevent pin tract infections, though some surgeons prefer to leave them protruding slightly for easier removal in the clinic.
7. Closure
Once fixation is secure and fluoroscopy confirms anatomic restoration of the scaphoid and carpal alignment, the wound is thoroughly irrigated.
- The volar wrist capsule must be meticulously repaired with absorbable sutures (e.g., 3-0 Vicryl) to restore volar stability and prevent radiocarpal subluxation.
- The FCR tendon sheath is left open to prevent stenosis.
- The subcutaneous tissue and skin are closed in a standard fashion.
- A sterile dressing and a well-padded short-arm thumb spica splint are applied before tourniquet deflation to minimize hematoma formation.
Postoperative Protocol and Rehabilitation
The postoperative management following the Stark grafting operation requires strict adherence to immobilization protocols to ensure graft incorporation and bony union.
Phase 1: Immobilization (Weeks 0 to 6)
- The patient is maintained in a rigid short-arm thumb spica cast.
- Finger range of motion (ROM) exercises for the digits not immobilized are encouraged immediately to prevent stiffness and reduce edema.
- Elevation of the limb is critical for the first 48-72 hours.
- Radiographs are taken at 2 weeks and 6 weeks to monitor alignment and check for any hardware migration.
Phase 2: Clinical Assessment and Hardware Removal (Weeks 6 to 12)
- At 6 to 8 weeks, the cast is removed, and clinical healing is assessed (absence of tenderness in the anatomic snuffbox and over the volar scaphoid tubercle).
- If K-wires were left percutaneous, they are removed at this stage in the clinic. If buried, they may be removed under local anesthesia or left in place depending on surgeon preference and patient symptoms.
- A computed tomography (CT) scan formatted along the longitudinal axis of the scaphoid is highly recommended at 8 to 10 weeks to definitively confirm bony bridging across the graft site. Plain radiographs are often insufficient to accurately assess scaphoid union.
- Once early union is confirmed, the patient is transitioned to a removable thumb spica orthosis and begins gentle, active wrist and thumb ROM exercises under the guidance of a certified hand therapist.
Phase 3: Strengthening and Return to Activity (Months 3 to 6)
- Passive stretching and progressive strengthening exercises are initiated only after solid bony union is confirmed on CT.
- Patients are advised to avoid heavy lifting, contact sports, or activities that place high impact loads on the wrist for at least 4 to 6 months postoperatively.
- Maximum medical improvement regarding wrist range of motion and grip strength may take up to one year. It is common for patients to experience a slight, permanent reduction in terminal wrist flexion and extension compared to the contralateral side.
Complications and Management
Despite meticulous surgical technique, scaphoid nonunion grafting carries inherent risks:
- Persistent Nonunion: The most common complication. Risk factors include smoking, inadequate debridement of necrotic bone, failure to correct the humpback deformity, and unrecognized proximal pole AVN. Management may require revision grafting with a vascularized bone flap or salvage procedures (e.g., proximal row carpectomy or four-corner fusion) if SNAC changes have developed.
- Hardware Complications: K-wire migration, breakage, or pin tract infections. Buried wires reduce infection risk but require a minor secondary procedure for removal if they become symptomatic.
- Avascular Necrosis: Disruption of the remaining blood supply during aggressive volar dissection can lead to proximal pole necrosis. Careful preservation of the dorsal soft tissue envelope is mandatory.
- Wrist Stiffness: Prolonged immobilization inevitably leads to some degree of capsular contracture. Early digit motion and dedicated postoperative hand therapy are essential to mitigate this.
Conclusion
The Stark et al. grafting operation remains a cornerstone technique in the armamentarium of the orthopedic hand surgeon. By utilizing a volar approach to directly address the biomechanical collapse of the scaphoid, this procedure effectively corrects the humpback deformity, restores carpal kinematics, and provides a robust biological environment for fracture union. Mastery of the excavation process, precise graft shaping, and meticulous K-wire fixation are critical to achieving successful outcomes and preventing the devastating long-term consequences of scaphoid nonunion.
You Might Also Like

