Vascularized Bone Grafts for Scaphoid Nonunion
Key Takeaway
Vascularized bone grafts are a critical surgical intervention for recalcitrant scaphoid nonunions, particularly those complicated by proximal pole avascular necrosis or failed prior reconstructions. By restoring local blood supply alongside structural osteoconduction, pedicled grafts—such as the pronator quadratus flap—significantly enhance union rates. This guide details the indications, biomechanical principles, and step-by-step surgical techniques required to optimize outcomes in complex carpal nonunions and naviculocapitate fracture syndromes.
INTRODUCTION TO VASCULARIZED BONE GRAFTS IN CARPAL RECONSTRUCTION
The treatment of scaphoid nonunions remains one of the most formidable challenges in hand and wrist surgery. Because of the scaphoid’s unique retrograde intraosseous vascular anatomy—where the primary blood supply enters distally and flows proximally—fractures through the waist or proximal pole frequently disrupt perfusion to the proximal fragment. This ischemic environment heavily predisposes the patient to avascular necrosis (AVN) and recalcitrant nonunion.
While conventional non-vascularized autografts (such as the Matti-Russe technique or structural iliac crest grafts) are highly successful for well-perfused nonunions, their efficacy drops precipitously in the presence of proximal pole ischemia or in the revision setting. In these complex scenarios, the use of vascularized bone grafts (VBGs) has proven to be a highly effective, biologically superior method. By transferring living, perfused osteocytes and osteoblasts directly into the nonunion site, VBGs bypass the prolonged phase of creeping substitution, accelerating osteogenesis and maximizing the probability of union.
Since Braun’s seminal 1983 report detailing the success of a pronator quadratus pedicled graft harvested from the distal radius, the surgical armamentarium has expanded significantly. Today, multiple sources of pedicled flaps from the distal radius, ulna, and metacarpals have been described. Prominent examples include the 1,2 intercompartmental supraretinacular artery (1,2 ICSRA) graft, distal dorsolateral radius grafts, and microvascular free flaps such as the medial femoral condyle or iliac crest free flap.
Clinical Pearl: Although vascularized pedicled grafts are highly effective for promoting biological healing, careful patient selection is paramount. As noted by Kawai and Yamamoto, the presence of established radiocarpal arthrosis (Scaphoid Nonunion Advanced Collapse - SNAC) may severely compromise the functional outcome, even if radiographic union is achieved. In such cases, salvage procedures are preferred.
INDICATIONS AND PREOPERATIVE PLANNING
Primary Indications
- Avascular Necrosis (AVN): Scaphoid nonunions demonstrating a sclerotic, avascular proximal pole on MRI (lack of gadolinium enhancement) or intraoperative punctate bleeding assessment.
- Recalcitrant Nonunions: Cases that have failed to heal after previous surgical interventions (e.g., failed Herbert screw fixation with non-vascularized grafting).
- Proximal Pole Fractures: Very proximal fractures with a high predictive rate of ischemia and nonunion.
Contraindications
- Advanced Carpal Collapse: Established SNAC wrist (Stage II or III) with significant radiocarpal or midcarpal arthrosis.
- Active Infection: Any signs of osteomyelitis or soft tissue infection.
- Inadequate Bone Stock: Severe fragmentation of the proximal pole that cannot mechanically support a graft or fixation.
SURGICAL TECHNIQUE: PRONATOR QUADRATUS PEDICLE BONE GRAFT
The pronator quadratus (PQ) pedicled bone graft utilizes a block of cancellous bone from the volar distal radius, nourished by the muscular branches of the anterior interosseous artery (AIA) supplying the pronator quadratus muscle.
1. Patient Positioning and Approach
The patient is positioned supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm.
- Make a volar zigzag (Bruner-type) or longitudinal incision over the scaphoid tuberosity, extending proximally over the volar distal radius to expose both the nonunion site and the graft harvest site.
- Carefully retract the flexor carpi radialis (FCR) tendon ulnarly and the radial artery radially to protect the neurovascular structures.
- Identify and divide the radioscaphocapitate (RSC) ligament complex to expose the scaphoid. Crucial Step: Retain the divided ends of the RSC ligament; it must be meticulously repaired during closure to prevent postoperative carpal instability.
2. Preparation of the Nonunion Site
- Expose the scaphoid nonunion. Assess the proximal pole for punctate bleeding after tourniquet deflation (if necessary) to confirm the vascular status.
- Excise all fibrous tissue and sclerotic bone ends.
- Using a high-speed power burr under continuous saline irrigation, freshen the bone ends to form an oval cavity approximately 10 to 20 mm long, oriented parallel to the longitudinal axis of the scaphoid.
- Ensure that the cavity extends into healthy, bleeding cancellous bone in both the proximal and distal fragments.
3. Correction of Carpal Deformity
Scaphoid waist nonunions frequently collapse into a "humpback" deformity, leading to Dorsal Intercalated Segment Instability (DISI).
* Apply longitudinal traction force to the thumb.
* Simultaneously, use a periosteal elevator or joystick K-wires to extend the distal scaphoid pole and flex the proximal pole.
* This maneuver corrects the intercalated segment instability, restores the scaphoid's anatomical length, and opens the volar cavity to allow the grafted bone to be inserted snugly.
4. Graft Harvest
- Identify the pronator quadratus muscle on the volar aspect of the distal radius.
- Outline a block of corticocancellous bone measuring 15 to 20 mm long at the distal insertion of the PQ on the distal radius, in close proximity to the abductor pollicis longus (APL) tendon.
- Surgical Tip: Outline the margin of the intended graft by drilling multiple contiguous holes with a fine Kirschner wire (K-wire). This creates a perforation line that facilitates precise separation with a fine osteotome and prevents catastrophic propagation of a cortical fracture into the radiocarpal joint.
- Carefully elevate the bone block using a sharp, curved osteotome.
Surgical Warning: Ensure that the pronator quadratus muscle fibers are not detached from the harvested bone graft. The viability of the graft depends entirely on this musculoperiosteal attachment.
5. Pedicle Mobilization
- Dissect the pronator quadratus muscle proximally and toward the ulna to secure a robust muscle pedicle approximately 20 mm thick.
- Note: The main anterior interosseous vessels do not need to be formally identified or skeletonized, as the microvascular network within the muscle belly is sufficient to sustain the graft.
- If the muscle pedicle is too tight to allow tension-free transfer of the bone block into the scaphoid cavity, dissect the ulnar origin of the pronator quadratus subperiosteally from the ulna. This may require an additional small incision over the distal ulna to safely release the muscle origin and increase excursion.
6. Graft Inset and Fixation
- Pack additional autologous cancellous bone (harvested from the ilium or distal radius) into the deepest portions of the scaphoid cavity to maximize osteoconduction.
- Insert the vascularized PQ bone block snugly into the volar window of the scaphoid. Often, the cortical surface of the graft can be fashioned to sit flush with the volar cortex of the scaphoid.
- Fix the proximal scaphoid segment, the distal scaphoid segment, and the interposed graft using two 0.045-inch (1.16-mm) Kirschner wires.
- Observe correct placement of the wires through the volar window, ensuring they capture all three components securely without violating the radiocarpal or midcarpal articular surfaces.
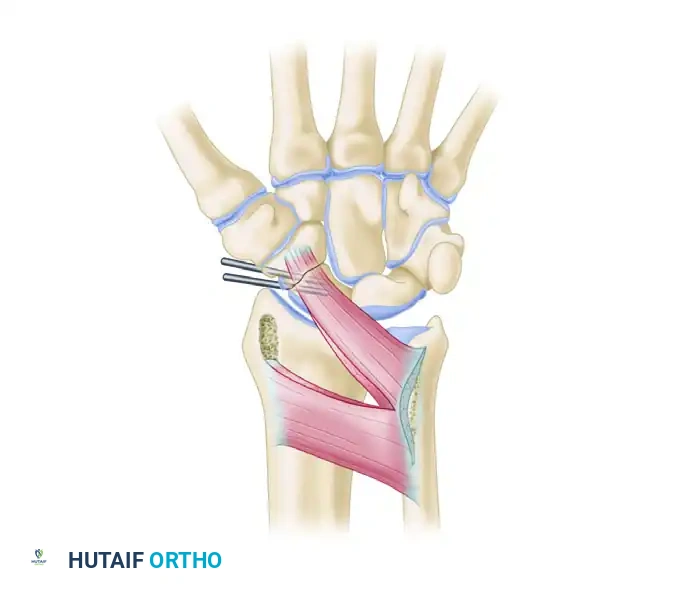
Figure 69-44: Pronator quadratus pedicle bone graft for scaphoid nonunion. The vascularized graft fills the excavated site of the nonunion and is rigidly fixed with Kirschner wires, restoring carpal alignment and providing a biological stimulus for union.
- Alternative Fixation: The K-wires can be inserted retrogradely or anterogradely after packing the cavity, but it is often easier to verify their trajectory before fully seating the graft. If a cortical strut is used to cap the volar window, stabilize it with one additional 0.028-inch (0.7-mm) K-wire.
- Cut the K-wires off beneath the skin to prevent pin-tract infections.
7. Closure
- Meticulously approximate the radioscaphocapitate capsule and ligaments with heavy absorbable sutures. Failure to repair the volar capsule can result in iatrogenic carpal instability.
- Close the subcutaneous tissues and skin in a standard fashion.
POSTOPERATIVE CARE AND REHABILITATION
Strict adherence to postoperative immobilization is critical to protect the delicate vascular pedicle and ensure bony union.
- Immediate Postoperative Phase: Immobilize the extremity in a rigid, long-arm thumb spica splint. The forearm should be positioned in supination (to relax the pronator quadratus pedicle), the wrist in neutral, and the thumb in palmar abduction.
- Two Weeks Postoperative: The surgical sutures are removed. The patient is transitioned into a well-molded long-arm thumb spica cast, which is worn for an additional 6 weeks.
- Eight Weeks Postoperative: Clinical and radiographic evaluation (often utilizing fine-cut CT scans) is performed to assess bridging trabeculae.
- Hardware Removal: The buried Kirschner wires are removed only after definitive radiographic evidence of fracture union is observed.
- Rehabilitation: Once immobilization is discontinued, patients are permitted to use the wrist and hand for light, activities of daily living (ADLs). Strenuous, load-bearing, and forceful activities are strictly discouraged for an additional 2 months to allow for complete graft incorporation and remodeling.
SALVAGE PROCEDURES: ARTHRODESIS OF THE WRIST
When evaluating old, ununited, or malunited fractures of the scaphoid, the surgeon must carefully assess the articular cartilage. If associated radiocarpal traumatic arthritis (SNAC wrist) is present, attempting a vascularized bone graft is generally contraindicated, as it will not relieve the patient's arthritic pain.
In these advanced stages, wrist arthrodesis (either partial or total) should be considered as a salvage procedure. Depending on the stage of the SNAC collapse, options include:
* Radial styloidectomy (for early Stage I).
* Proximal Row Carpectomy (PRC) or Scaphoid Excision and Four-Corner Fusion (for Stage II/III).
* Total Wrist Arthrodesis (for pan-carpal arthritis).
NAVICULOCAPITATE FRACTURE SYNDROME AND CAPITATE FRACTURES
Pathomechanics and Mechanism of Injury
Historically referred to as Fenton's syndrome, the naviculocapitate (scaphocapitate) fracture syndrome is a rare but severe complex carpal injury. It must always be considered among the associated injuries that can occur alongside a high-energy fracture of the scaphoid.
The mechanism of injury is highly specific and sequential:
1. Axial Compression: A massive axial load is applied to a forcefully dorsiflexed wrist.
2. Scaphoid Failure: The extreme dorsiflexion forces the scaphoid to fracture first, typically at the waist.
3. Capitate Impaction: As the wrist is forced into further dorsiflexion, the dorsal lip of the distal radius forcefully impacts the head of the capitate.
4. Capitate Fracture and Rotation: The shearing force fractures the capitate. As the carpus continues into extreme dorsiflexion, the proximal head of the capitate rotates 90 degrees.
5. Rebound Rotation: When the deforming force dissipates and the hand returns to a neutral position, the proximal fragment of the capitate is dragged further, resulting in a full 180 degrees of rotation. The articular surface of the capitate head now faces distally, while the fracture surface faces proximally toward the radius.
Clinical Presentation and Associated Injuries
This syndrome is indicative of a massive disruption of the carpal arcs. It is frequently associated with:
* Dorsal Perilunate Dislocations (PLD) or Fracture-Dislocations.
* Fractures of the distal end of the radius.
Surgical Management
Conservative management of naviculocapitate syndrome is universally destined to fail due to the severe displacement and rotation of the capitate head, which rapidly leads to avascular necrosis and catastrophic midcarpal arthrosis.
- Open Reduction: Urgent open reduction is mandatory. The surgeon must carefully expose the midcarpal joint, identify the inverted proximal capitate fragment, and manually derotate it 180 degrees back into its anatomical position within the lunate fossa.
- Internal Fixation: Once reduced, the capitate fracture is rigidly fixed, typically with headless compression screws or multiple K-wires. The scaphoid fracture is subsequently addressed, often requiring structural bone grafting and screw fixation to restore the radial column.
- Note: In cases of severe comminution or delayed presentation where the capitate head is entirely devoid of soft tissue attachments and grossly necrotic, some surgeons have historically advocated for primary excision of the proximal capitate pole, though modern techniques favor anatomical restoration whenever feasible to preserve midcarpal kinematics.
📚 Medical References
You Might Also Like

