Comprehensive Management of Knee Dislocations: Classification, Evaluation, and Surgical Reconstruction

Key Takeaway
Knee dislocations are severe, limb-threatening injuries requiring immediate neurovascular assessment. The Schenck classification categorizes these multiligamentous injuries to guide surgical reconstruction. Initial management prioritizes popliteal artery evaluation using the ankle-brachial index (ABI) and CT angiography. Surgical intervention involves phased or single-stage multiligament reconstruction, dictated by hemodynamic stability, vascular integrity, and soft-tissue conditions.
INTRODUCTION AND BIOMECHANICS
Traumatic knee dislocations represent one of the most devastating and limb-threatening injuries in orthopedic traumatology. Historically considered rare, the true incidence of multiligamentous knee injuries (MLKIs) is likely underestimated due to spontaneous reduction prior to clinical presentation. These injuries demand a high index of suspicion, meticulous clinical evaluation, and a multidisciplinary approach to prevent catastrophic outcomes, including limb amputation.
The biomechanics of a knee dislocation involve catastrophic failure of the primary static stabilizers of the knee. The knee joint relies on the intricate interplay of the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), lateral collateral ligament (LCL), and the posterolateral corner (PLC). Dislocation typically requires the rupture of at least two, and often three or four, of these major ligamentous structures.
Mechanisms of injury are broadly categorized by velocity:
* High-Velocity Injuries: Typically resulting from motor vehicle collisions or severe industrial accidents. These are frequently associated with open injuries, severe soft-tissue degloving, concomitant fractures, and a high incidence of neurovascular compromise.
* Low-Velocity Injuries: Often sustained during athletic participation (e.g., football, skiing) involving complex torsional forces.
* Ultra-Low-Velocity Injuries: Increasingly recognized in the morbidly obese population. A simple misstep or low-energy fall can generate massive sheer forces across the knee joint, leading to profound multiligamentous disruption and a surprisingly high rate of vascular injury.
Clinical Pearl: Never underestimate the ultra-low-velocity knee dislocation in an obese patient. The lever arm and sheer mass involved frequently result in severe intimal tearing of the popliteal artery despite the innocuous mechanism of injury.
CLASSIFICATION OF KNEE DISLOCATIONS
Classification systems for knee dislocations are essential for standardizing communication, guiding preoperative planning, and predicting outcomes. Historically, dislocations were classified by the position of the tibia relative to the femur (Kennedy Classification) or by the mechanism of injury. However, the modern standard relies on the anatomic status of the ligaments.
Positional Classification (Kennedy)
This system describes the direction of tibial displacement relative to the femur:
* Anterior (40%): The most common type, typically resulting from forced hyperextension. The posterior capsule tears first, followed by the PCL and ACL. Popliteal artery traction injuries are highly prevalent.
* Posterior (33%): Usually caused by a direct blow to the proximal tibia with the knee flexed (e.g., dashboard injury). The PCL fails first.
* Medial (4%): Caused by severe valgus forces.
* Lateral (18%): Caused by severe varus forces.
* Rotatory (5%): Posterolateral rotatory dislocations are notorious for being irreducible due to the medial femoral condyle buttonholing through the medial capsule.
Anatomic Classification (Schenck Classification)
The Schenck classification, modified by Wascher, is the most widely utilized system as it focuses on identifying which specific structures are injured, directly informing surgical reconstruction timing and techniques.
- KD-I: Multiligamentous injury with one cruciate ligament intact. Usually, the PCL is intact with the ACL and a collateral ligament torn. Less commonly, the ACL is intact with a complete PCL tear.
- KD-II: Both the ACL and PCL are torn, but both collateral ligaments remain intact.
- KD-III: Both cruciates are torn, along with one collateral ligament complex.
- KD-IIIM: ACL, PCL, and MCL/posteromedial corner torn; lateral side intact.
- KD-IIIL: ACL, PCL, and LCL/posterolateral corner torn; medial side intact. (Highest risk for peroneal nerve injury).
- KD-IV: Pan-ligamentous injury. All four major ligaments (ACL, PCL, MCL, LCL/PLC) are torn.
- KD-V: Any multiligamentous knee injury associated with a periarticular fracture (e.g., tibial plateau or distal femur fracture).
Surgical Warning: The Schenck classification is highly useful but limited in the acute setting by the difficulty of obtaining an accurate physical examination due to pain, guarding, and swelling. Examination under anesthesia (EUA) and MRI are critical for definitive classification.
CLINICAL AND RADIOGRAPHIC EVALUATION
Initial Assessment and Physical Examination
The initial evaluation of a patient with a suspected knee dislocation must follow Advanced Trauma Life Support (ATLS) protocols, as these are frequently high-energy polytrauma patients.
Once life-threatening injuries are addressed, the extremity must be examined thoroughly. Visual inspection may reveal gross deformity, swelling, or ecchymosis. A transverse anteromedial skin furrow (the "dimple sign") is pathognomonic for an irreducible posterolateral dislocation, indicating that the medial femoral condyle has buttonholed through the medial capsule.
Physical examination for ligamentous laxity (Lachman, posterior drawer, varus/valgus stress at 0° and 30°, dial test) should be attempted but is often limited. The extensor mechanism must be evaluated, and the limb must be serially examined for signs of compartment syndrome, which can develop insidiously as joint capsule disruption allows bleeding into the calf compartments.
Radiographic Evaluation
Initial radiographic evaluation focuses on determining the direction of the dislocation and identifying concomitant bony injuries, such as avulsion fractures (e.g., Segond fracture, fibular head avulsion) or periarticular fractures.
Anteroposterior (AP), lateral, and oblique views must be obtained immediately before and after reduction.
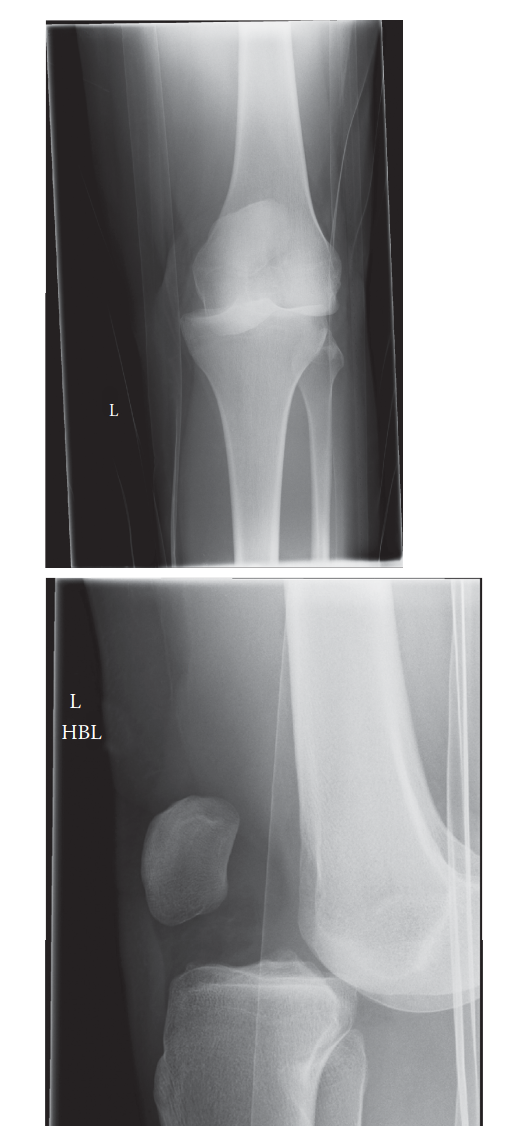
Figure 1: Anteroposterior (AP) radiograph demonstrating a gross lateral knee dislocation with complete loss of tibiofemoral articulation.

Figure 2: Lateral radiograph of the same patient confirming the severe displacement and disruption of the joint axis.
Following successful closed reduction and stabilization (often via a knee immobilizer or external fixator), advanced imaging is required.
* Magnetic Resonance Imaging (MRI): The gold standard for evaluating soft tissue injuries. MRI accurately identifies midsubstance tears versus avulsions of the cruciates and collaterals, meniscal pathology, and the status of the popliteus tendon and PLC.
* Computed Tomography (CT): Indicated if there is a suspected periarticular fracture (KD-V) to aid in preoperative planning for osseous fixation.
VASCULAR AND NERVE INJURIES
Vascular Injuries: The Ultimate Priority
The absolute first priority in the assessment and treatment of traumatic knee dislocations is the vascular status of the extremity. The popliteal artery is uniquely vulnerable due to its anatomic tethering proximally at the adductor hiatus and distally at the soleus arch. During a dislocation, the artery is subjected to massive traction and sheer forces, leading to intimal disruption, dissection, and subsequent thrombosis.
The incidence of popliteal artery injury ranges from 7% to 25% in modern series. It is critical to understand that the presence of palpable pedal pulses does not exclude a limb-threatening vascular injury. An intimal flap may allow sufficient antegrade flow initially, only to thrombose hours later.
The Ankle-Brachial Index (ABI):
The ABI is the cornerstone of initial vascular assessment. It is calculated by dividing the systolic pressure in the injured ankle (dorsalis pedis or posterior tibial) by the systolic pressure in the uninjured arm.
* ABI > 0.90: High negative predictive value (100% in some prospective studies). Warrants serial clinical observation.
* ABI < 0.90: Indicates a high probability of arterial injury. Mandates immediate advanced vascular imaging (CT Angiography or conventional arteriography) or immediate surgical exploration if hard signs of ischemia are present.
Hard Signs of Arterial Ischemia:
* Absent pulses
* Expanding hematoma
* Pulsatile hemorrhage
* Palpable thrill or audible bruit
* Signs of distal ischemia (pallor, poikilothermia, paralysis, pain, pulselessness, paresthesia)
If hard signs are present, the patient must be taken emergently to the operating room for revascularization by a vascular surgeon. Ischemic time exceeding 6 to 8 hours is associated with amputation rates approaching 85%.

Figure 3: Femoral arteriogram in a patient with a knee dislocation demonstrating complete occlusion of the popliteal artery at the level of the joint line.
Neurologic Injuries
Nerve damage occurs in 10% to 40% of knee dislocations. The common peroneal nerve is most frequently injured, particularly in KD-IIIL (posterolateral corner) injuries, where the incidence can reach 45%. The mechanism is typically a traction neurapraxia or axonotmesis as the nerve is stretched around the fibular neck during severe varus and internal rotation forces.
Nearly half of these nerve injuries result in permanent neurological deficits (foot drop). Initial management is expectant, with ankle-foot orthosis (AFO) bracing. If no recovery is noted clinically or on electromyography (EMG) by 3 to 6 months, nerve exploration, neurolysis, or tendon transfer (e.g., posterior tibial tendon to the dorsum of the foot) may be indicated.
SURGICAL MANAGEMENT
The management of multiligamentous knee injuries has evolved from nonoperative cast immobilization to aggressive, anatomic surgical reconstruction. Evidence strongly supports operative intervention to restore joint kinematics, prevent early-onset osteoarthritis, and maximize functional recovery.
Indications and Timing
- Emergent Surgery: Indicated for vascular repair, open dislocations, irreducible dislocations (e.g., buttonholed medial condyle), or evolving compartment syndrome. In these cases, the orthopedic surgeon typically applies a spanning external fixator to stabilize the joint while the vascular surgeon repairs the popliteal artery.
- Acute/Subacute Reconstruction (2 to 3 weeks): The preferred window for definitive ligamentous reconstruction. Operating before 2 weeks carries a high risk of arthrofibrosis and fluid extravasation leading to compartment syndrome. Operating after 3-4 weeks makes identifying and repairing retracted capsular structures and collateral ligaments exceedingly difficult.
Patient Positioning and Setup
- Anesthesia: General anesthesia combined with a regional block (e.g., adductor canal block) for postoperative pain control.
- Positioning: The patient is placed supine on a radiolucent operating table. A lateral post or leg holder is utilized to allow full range of motion and valgus stress.
- Tourniquet: A proximal thigh tourniquet is applied but should be used judiciously, especially if there has been a prior vascular repair. In cases of repaired popliteal arteries, tourniquet use is generally contraindicated.
- Examination Under Anesthesia (EUA): A meticulous EUA is performed to confirm the exact instability pattern, documenting Lachman, pivot shift, dial test, and varus/valgus gapping.
Surgical Approaches and Step-by-Step Reconstruction
The surgical strategy typically involves a single-stage reconstruction of all injured ligaments, utilizing allograft tissue (Achilles, tibialis anterior, or hamstring) to minimize donor-site morbidity in an already traumatized limb.
1. Diagnostic Arthroscopy and Cruciate Preparation
- Standard anterolateral and anteromedial portals are established.
- The joint is debrided of hematoma and ligamentous stumps.
- Meniscal tears are repaired if possible, or debrided if irreparable.
- The femoral and tibial footprints of the ACL and PCL are identified and cleared.
2. PCL Reconstruction (The Foundation)
The PCL is the primary stabilizer of the knee and must be reconstructed first to establish the central axis.
* Tibial Tunnel: An accessory posteromedial portal is often established to protect the neurovascular bundle. A PCL guide is placed through the anteromedial portal and hooked over the posterior tibial facet. A guide pin is drilled from the anteromedial tibia to the posterior footprint, followed by reaming.
* Femoral Tunnel: Drilled inside-out through the anterolateral portal into the anatomic footprint of the anterolateral bundle of the PCL on the medial femoral condyle.
* Graft Passage: The Achilles allograft is passed from distal to proximal.
3. ACL Reconstruction
- Tibial Tunnel: Drilled using a standard ACL tibial guide set at 55 degrees, exiting at the anatomic footprint.
- Femoral Tunnel: Drilled independently through an accessory medial portal to ensure anatomic placement on the lateral femoral condyle.
- Graft Passage: The graft is passed but not yet tensioned.
4. Collateral and Corner Reconstruction
Open approaches are utilized for the medial and lateral sides.
Medial Side (MCL/PMC):
* A medial longitudinal incision is made.
* If the injury is acute (< 3 weeks) and the tissue is robust, primary repair with suture anchors may be attempted.
* If tissue is poor, an anatomic reconstruction of the superficial MCL and posterior oblique ligament (POL) is performed using allograft, securing the graft to the medial epicondyle, proximal tibia, and posteromedial tibia.
Lateral Side (LCL/PLC):
* A lateral hockey-stick incision is made.
* The common peroneal nerve is identified and neurolysed to protect it during the procedure.
* Anatomic reconstruction of the LCL, popliteus tendon, and popliteofibular ligament is performed (e.g., LaPrade technique).
* Fibular and tibial tunnels are drilled, and the femoral tunnels are placed at the anatomic footprints of the LCL and popliteus.
5. Graft Tensioning and Fixation Sequence
The sequence of tensioning is critical to restore normal knee kinematics:
1. PCL: Tensioned first at 90° of flexion with an anterior drawer force applied to restore the anatomic tibial step-off. Fixed with an interference screw.
2. ACL: Tensioned at full extension or 10° of flexion.
3. Collaterals: The LCL/PLC is tensioned at 30° of flexion with a valgus and internal rotation force. The MCL/POL is tensioned at 30° of flexion with a varus and internal rotation force.
Pitfall: Over-constraining the knee during collateral ligament tensioning is a common error. Ensure the knee can achieve full extension and at least 90° of flexion on the table before final fixation.
POSTOPERATIVE PROTOCOL
The postoperative rehabilitation following a multiligamentous knee reconstruction is a delicate balance between protecting the healing grafts and preventing arthrofibrosis.
- Phase I (0-4 weeks): The knee is locked in full extension in a hinged knee brace. Weight-bearing is strictly non-weight-bearing (NWB) or toe-touch weight-bearing (TTWB). Passive range of motion (PROM) is initiated early (0° to 90°) to prevent stiffness, but active hamstring contraction is avoided to protect the PCL graft.
- Phase II (4-8 weeks): Progression to partial weight-bearing. The brace is unlocked for ambulation if quad control is sufficient. ROM is advanced to full flexion.
- Phase III (8-16 weeks): Progression to full weight-bearing. Closed-chain kinetic exercises are initiated. Proprioceptive training begins.
- Phase IV (4-6 months+): Straight-line jogging, agility drills, and sport-specific training. Return to play is rarely achieved before 9 to 12 months and requires passing stringent functional criteria.
CONCLUSION
Knee dislocations are complex, limb-threatening injuries that require a systematic, multidisciplinary approach. Immediate identification and management of vascular injuries using the ABI and advanced imaging are paramount. Once the limb is salvaged, anatomic classification using the Schenck system guides the surgical strategy. Through meticulous, phased multiligamentous reconstruction and rigorous postoperative rehabilitation, orthopedic surgeons can restore stability and function to these devastatingly injured joints.
You Might Also Like