Latissimus Dorsi Transfer: Surgical Technique & Protocol
Key Takeaway
The latissimus dorsi transfer is a powerful salvage procedure for massive, irreparable posterosuperior rotator cuff tears. By transferring the latissimus dorsi tendon to the superolateral humeral head, surgeons can restore the glenohumeral force couple, improving external rotation and forward elevation. This guide details the precise surgical technique, critical neurovascular anatomy, biomechanical principles, and structured postoperative rehabilitation required to achieve optimal clinical outcomes in carefully selected patients.
INTRODUCTION TO LATISSIMUS DORSI TRANSFER
The management of massive, irreparable posterosuperior rotator cuff tears—specifically those involving the supraspinatus and infraspinatus tendons—presents a formidable challenge in orthopedic surgery. When primary repair is biologically or biomechanically impossible due to severe tendon retraction, advanced fatty infiltration (Goutallier stage 3 or 4), or poor tissue quality, joint-preserving salvage procedures must be considered for patients without advanced glenohumeral osteoarthritis.
The latissimus dorsi transfer, pioneered and popularized by Christian Gerber in the late 1980s, remains a cornerstone technique for restoring shoulder function in this specific demographic. By transferring the latissimus dorsi (LD) tendon from its native insertion on the lesser tuberosity and bicipital groove to the superolateral aspect of the greater tuberosity, the muscle is converted from an internal rotator and adductor into an external rotator and active depressor of the humeral head. This biomechanical conversion restores the critical transverse force couple of the shoulder, stabilizing the humeral head within the glenoid during active elevation.
This comprehensive guide details the indications, biomechanical principles, precise surgical technique, and rigorous postoperative rehabilitation protocols required to execute a successful latissimus dorsi transfer.
BIOMECHANICS AND ANATOMY
The Transverse Force Couple
Normal shoulder kinematics rely on a balanced transverse force couple. The subscapularis anteriorly balances the infraspinatus and teres minor posteriorly. In massive posterosuperior tears, this balance is lost, leading to superior migration of the humeral head, subacromial impingement, and a loss of active external rotation and forward elevation (often presenting as a positive external rotation lag sign or Hornblower's sign).
The transferred latissimus dorsi acts synergistically with the remaining intact rotator cuff. Its new vector provides a strong inferiorly directed force that counteracts the superior pull of the deltoid, centering the humeral head and allowing the deltoid to efficiently elevate the arm.
Surgical Anatomy of the Latissimus Dorsi
The latissimus dorsi is a broad, flat muscle originating from the spinous processes of T7-L5, the thoracolumbar fascia, the iliac crest, and the inferior three or four ribs. It converges into a flat tendon that spirals around the teres major to insert into the floor of the intertubercular (bicipital) groove of the humerus.
- Innervation: Thoracodorsal nerve (C6, C7, C8), a branch of the posterior cord of the brachial plexus.
- Blood Supply: Thoracodorsal artery, a continuation of the subscapular artery.
- Neurovascular Pedicle: The pedicle enters the muscle on its deep surface, approximately 3 to 4 cm medial to its lateral border and 8 to 10 cm distal to its humeral insertion. This proximal location allows for extensive distal mobilization of the muscle belly without compromising its viability.
Clinical Pearl: The latissimus dorsi tendon is distinctly separate from the teres major tendon, although they run in close proximity. The LD tendon is typically more tendinous at its insertion, whereas the teres major has muscular fibers extending almost to its bony attachment. Recognizing this distinction is critical during harvest.
INDICATIONS AND PATIENT SELECTION
Careful patient selection is the most critical determinant of success in latissimus dorsi transfer. The procedure is technically demanding and requires a highly compliant patient for the prolonged postoperative rehabilitation phase.
Primary Indications
- Massive, irreparable posterosuperior rotator cuff tears (supraspinatus and infraspinatus).
- Intractable pain and significant loss of active external rotation and elevation.
- Younger, physiologically active patients (typically under 65 years of age) who demand high functional use of the extremity.
- Failure of conservative management (physical therapy, corticosteroid injections).
Critical Prerequisites
- Intact Subscapularis: An intact and functioning subscapularis is an absolute prerequisite. Without it, the anterior aspect of the transverse force couple is absent, and the LD transfer will fail to center the humeral head, leading to continued anterosuperior escape.
- Intact Deltoid: The deltoid must be fully functional to provide the primary motor force for elevation once the humeral head is stabilized.
- Minimal Glenohumeral Arthritis: Patients with advanced arthropathy (Hamada Grade 4 or 5) are better served by a Reverse Total Shoulder Arthroplasty (RTSA).
Contraindications
- Severe glenohumeral osteoarthritis or cuff tear arthropathy.
- Irreparable subscapularis tears.
- Deltoid dysfunction or axillary nerve palsy.
- True pseudoparalysis (inability to actively elevate the arm beyond 90 degrees in the presence of a completely stiff shoulder), though some authors argue that LD transfer can reverse pseudoparalysis if the subscapularis is intact.
- Inability to comply with strict postoperative rehabilitation.
PREOPERATIVE PLANNING
Advanced imaging is mandatory. Magnetic Resonance Imaging (MRI) is utilized to assess the degree of tendon retraction and, most importantly, the extent of fatty infiltration in the rotator cuff musculature. Goutallier stage 3 (more fat than muscle) or 4 (completely fat) in the supraspinatus and infraspinatus confirms irreparability. The subscapularis and teres minor must be evaluated for structural integrity and muscle quality.
Computed Tomography (CT) may be utilized to assess glenoid morphology and humeral bone stock, particularly if there is a concern for cystic changes at the greater tuberosity where the transfer will be anchored.
SURGICAL TECHNIQUE
The procedure can be performed via a single-incision posterior approach or a dual-incision (superior and posterior) approach. The classic single-incision posterior approach is detailed below, as it provides excellent access for both harvest and fixation.
1. Patient Positioning and Anesthesia
- Anesthesia: General anesthesia combined with an interscalene regional block is recommended for optimal pain control and muscle relaxation.
- Positioning: The patient is placed in the lateral decubitus position on a beanbag. The operative arm is draped free to allow for full manipulation during the procedure. A sterile hydraulic arm positioner (e.g., Spider arm) can be highly beneficial.
- Preparation: The entire forequarter, including the axilla and the posterior hemithorax down to the iliac crest, must be prepped and draped.
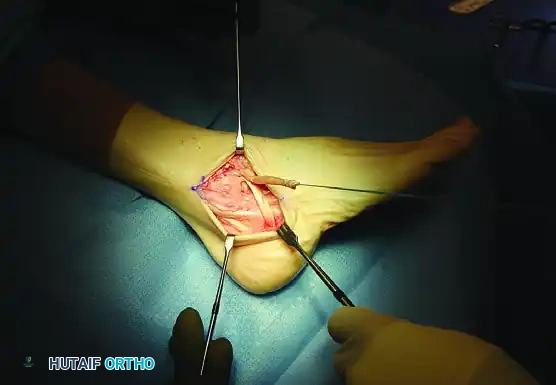
2. Incision and Exposure
Once the irreparability of the supraspinatus and infraspinatus tendons is confirmed (often via a preliminary arthroscopic evaluation), proceed to the latissimus dorsi transfer.
Make a 12- to 15-cm longitudinal posterior skin incision. The incision should follow the lateral border of the latissimus dorsi muscle, starting from the posterior axillary fold and extending distally toward the inferior angle of the scapula.
Dissect through the subcutaneous tissue to expose the deep fascia. Identify the lateral border of the latissimus dorsi.
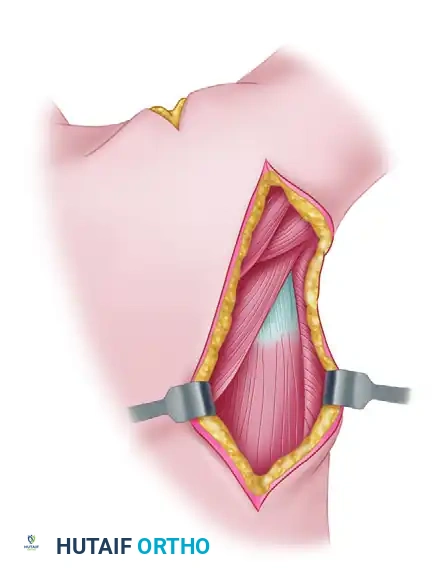
3. Tendon Harvest and Release
Develop the plane between the latissimus dorsi and the underlying teres major. This plane is relatively avascular but requires careful blunt dissection. Trace the latissimus dorsi proximally toward its insertion on the humerus.
Identify the muscle, and meticulously release it from the humeral shaft. The insertion is a broad, flat tendon located in the floor of the bicipital groove.
🚨 SURGICAL WARNING: NEUROVASCULAR STRUCTURES
Extreme caution must be exercised during the detachment of the tendon from the humerus.
* Axillary Nerve: Lies immediately adjacent to the proximal (superior) end of the tendon.
* Radial Nerve: Curves around the humerus immediately distal (anterior) to the tendon insertion.
Keep dissection strictly on the bone during detachment to avoid catastrophic nerve injury.
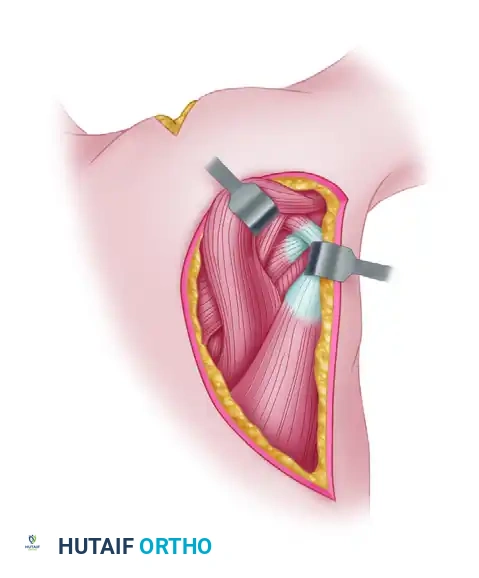
4. Mobilization of the Muscle
Once detached, the tendon is grasped with a heavy clamp or traction suture. To achieve adequate excursion for the transfer to reach the greater tuberosity, the muscle belly must be extensively mobilized.
Identify the neurovascular bundle (thoracodorsal nerve and artery) on the deep, anterior surface of the muscle. Carefully mobilize the latissimus dorsi distally, releasing all fascial attachments to the inferior angle of the scapula and the chest wall. The pedicle must be visualized and protected throughout this mobilization. Adequate release is achieved when the tendon can easily reach the posterosuperior acromion with the arm at the side.
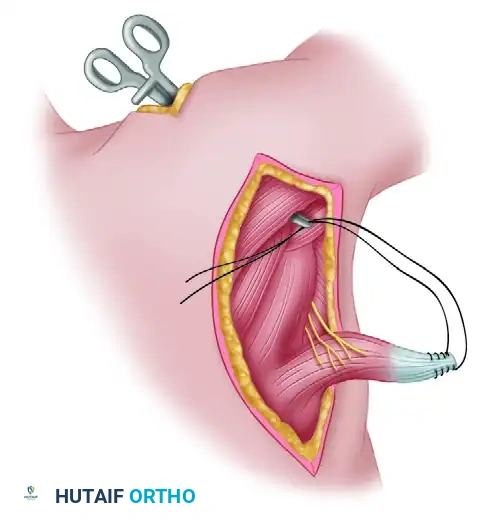
5. Tendon Preparation and Transfer
Prepare the distal end of the harvested tendon. Pass two No. 3 braided polyester sutures (or modern high-strength ultra-high-molecular-weight polyethylene sutures) through the tendon at its medial and lateral borders using a locking Krackow technique. This provides a robust grasp on the tendon for subsequent tensioning and fixation.
Next, develop the transfer interval. Use a long clamp or passing instrument to pull the prepared tendon through the plane between the infraspinatus-teres minor complex (posteriorly) and the deltoid muscle (anteriorly and superiorly).
Ensure the tendon is not twisted during passage. The transfer must route superficial to the teres major and deep to the posterior deltoid.
6. Fixation to the Humeral Head
Expose the superolateral aspect of the humeral head (the native footprint of the supraspinatus and infraspinatus). Prepare a bony trough in the greater tuberosity using a burr or osteotome to expose bleeding cancellous bone, which is critical for tendon-to-bone healing.
Anchor the transferred tendon to the bony trough. The classic technique involves pulling the heavy nonabsorbable sutures out through the bone via transosseous tunnels and tying the knots over the lateral cortex of the greater or lesser tuberosity.
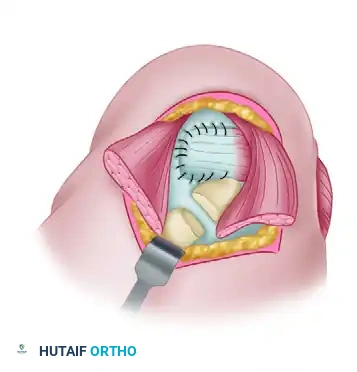
Modern Alternative: Many surgeons now utilize double-row suture anchor constructs (transosseous-equivalent) for fixation, which provides excellent biomechanical strength and maximizes the footprint contact area.
Tensioning: The tendon must be fixed under appropriate tension. The arm should be positioned in 45 degrees of abduction and 30 to 45 degrees of external rotation during knot tying.
7. Cuff Integration and Closure
If possible, suture the remaining anterior and posterior rotator cuff tissue (subscapularis and teres minor remnants) to the medial and lateral borders of the transferred latissimus dorsi tendon. This creates a continuous fibrous canopy, enhancing the biomechanical force couple and improving the watertight seal of the joint.
If the remaining cuff cannot be mobilized for repair, meticulously débride the degenerative edges. If the deltoid was detached from the acromion during a superior approach (if utilized), reattach it securely with transosseous sutures.
Irrigate the wound copiously. Place a closed-suction drain in the axillary space to prevent hematoma formation. Close the deltopectoral fascia (if opened) and the deep fascial layers over the posterior incision. Close the subcutaneous tissue and skin in a standard layered fashion.
POSTOPERATIVE CARE AND REHABILITATION
The success of a latissimus dorsi transfer is heavily dependent on strict adherence to a phased postoperative rehabilitation protocol. The transferred muscle must heal to the bone, and the patient's central nervous system must be retrained to fire the latissimus dorsi during shoulder elevation and external rotation—a process known as cortical plasticity.
Phase I: Protection and Healing (Weeks 0 to 6)
- Immobilization: The arm is immediately placed in a specialized shoulder orthosis (splint) in 45 degrees of abduction and 30 to 45 degrees of external rotation. This position minimizes tension on the repair site.
- Duration: The splint is worn full-time (24 hours a day) for 6 weeks.
- Exercises: Passive range-of-motion (ROM) exercises out of the splint are started on the first postoperative day under the strict guidance of a physical therapist. Movements are restricted to forward elevation and external rotation within safe limits to prevent stiffness while protecting the repair. Internal rotation and adduction are strictly prohibited.
Phase II: Active Motion and Neuromuscular Re-education (Weeks 6 to 12)
- Splint Weaning: After 6 weeks, the abduction splint is gradually discontinued.
- Active ROM: Active-assisted and active abduction and external rotation exercises are begun.
- Biofeedback: Neuromuscular electrical stimulation (NMES) and biofeedback techniques are highly recommended during this phase. Patients must consciously learn to contract the latissimus dorsi to initiate external rotation and elevation.
Phase III: Strengthening and Functional Return (Months 3 to 9)
- Strengthening: Progressive resistive strengthening exercises are initiated at 3 months postoperatively. Focus is placed on the deltoid, the transferred latissimus dorsi, and the periscapular stabilizers.
- Duration: Strengthening and functional retraining are continued for 6 to 9 months. Maximum medical improvement may not be reached until 12 to 18 months postoperatively, as cortical retraining is a slow process.
COMPLICATIONS AND OUTCOMES
Potential Complications
- Nerve Injury: The most devastating complication is injury to the radial or axillary nerve during tendon harvest, or injury to the thoracodorsal pedicle during mobilization. Meticulous surgical technique is paramount.
- Tendon Rupture: Failure of the tendon-to-bone healing or traumatic rupture of the transfer can occur, usually due to non-compliance with the postoperative splinting protocol.
- Hematoma: The extensive dead space created by harvesting the LD muscle belly predisposes the patient to hematoma and seroma formation. Closed suction drainage is essential.
- Infection: Deep surgical site infections require prompt irrigation and debridement.
Clinical Outcomes
When performed for the correct indications, latissimus dorsi transfer yields highly satisfactory results. Long-term studies demonstrate significant improvements in pain relief, active forward elevation, and active external rotation. Patients typically experience a reversal of the external rotation lag sign and a restoration of the ability to perform activities of daily living at waist and head height. While it does not restore a completely "normal" shoulder, it provides a durable, joint-preserving solution that significantly enhances the quality of life for patients with massive, irreparable posterosuperior rotator cuff tears.
You Might Also Like