Total Knee Arthroplasty for Varus Knee Deformity: Surgical Anatomy & Management

Key Takeaway
Total Knee Arthroplasty (TKA) for varus knees requires meticulous planning. Surgeons must understand specific bony and ligamentous changes, like MCL contracture and lateral laxity. Expert strategies involve precise bone resections and comprehensive soft tissue balancing to correct deformity, restore mechanical alignment, and ensure long-term patient satisfaction.
Total Knee Replacement in the Varus Knee: Expert Surgical Strategies
Introduction & Epidemiology
Total knee arthroplasty (TKA) is a highly successful procedure for alleviating pain and restoring function in patients with end-stage knee arthritis. The varus knee, characterized by medial compartment collapse and coronal plane malalignment, represents the most common presentation of osteoarthritis necessitating TKA. Epidemiological data indicate that varus deformity accounts for approximately 80-90% of osteoarthritic knees undergoing primary TKA. This deformity results from progressive cartilage loss and subchondral bone erosion primarily in the medial tibiofemoral compartment, often compounded by laxity or contracture of surrounding soft tissues. Achieving a well-balanced, stable knee with appropriate mechanical alignment is paramount for long-term implant survival and patient satisfaction in these cases. Failure to adequately address the complex biomechanical alterations and soft tissue imbalances inherent to the varus knee can lead to persistent pain, instability, reduced range of motion, and accelerated wear. This chapter outlines expert surgical strategies for managing varus knee deformities during TKA, emphasizing meticulous preoperative planning, precise bone resections, and comprehensive soft tissue balancing.
Surgical Anatomy & Biomechanics
A thorough understanding of the knee's anatomy and biomechanics is fundamental for successful TKA in the varus knee.
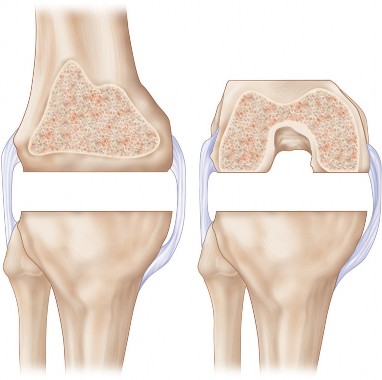
Bony Anatomy
The varus knee typically presents with distinct bony alterations:
*
Medial Tibial Plateau:
Significant cartilage loss and subchondral bone wear, leading to medial metaphyseal bone loss and depression of the articular surface. This often necessitates bone augmentation or deeper cuts.
*
Medial Femoral Condyle:
Cartilage erosion and potential osteophyte formation.
*
Femoral Bowing:
Proximal femoral bowing or distal femoral condylar hypoplasia can influence the femoral valgus cut angle, requiring careful assessment on long-leg radiographs.
*
Patella:
May exhibit tilt or subluxation laterally due to the overall varus alignment.
Ligamentous Anatomy and Soft Tissue Changes
The soft tissue envelope in a varus knee undergoes predictable changes:
*
Medial Compartment:
The medial collateral ligament (MCL) complex is typically contracted and tight. This complex includes the superficial MCL (sMCL), deep MCL (dMCL), and posterior oblique ligament (POL). The pes anserinus tendons (sartorius, gracilis, semitendinosus) and the capsule-meniscal complex also contribute to medial tightness. The semimembranosus attachments can also be contracted.
*
Lateral Compartment:
The lateral collateral ligament (LCL) and posterolateral corner structures (popliteus tendon, arcuate complex) are often attenuated or stretched due due to chronic tension, leading to laxity in extension and potentially in flexion.
*
Posterior Cruciate Ligament (PCL):
Its status (intact, attenuated, contracted) influences component choice (cruciate-retaining vs. posterior-stabilized) and surgical technique. In some severe varus cases, the PCL may be contracted.
Biomechanics of Varus Deformity
The normal mechanical axis of the lower limb passes through the center of the femoral head, the center of the knee, and the center of the ankle. In a varus knee, the mechanical axis deviates medially to the center of the knee, concentrating compressive forces on the medial compartment. This leads to:
*
Increased Medial Compartment Loading:
Exacerbating cartilage wear and subchondral sclerosis.
*
Soft Tissue Imbalance:
The chronic compressive forces medially lead to shortening and contracture of medial structures, while the lateral compartment becomes distended and relatively lax. This imbalance is often more pronounced in extension than in flexion.
*
Fixed vs. Correctable Deformity:
The chronicity and severity of the varus determine whether the deformity is fixed (irreducible with valgus stress) or correctable (reducible with valgus stress). Fixed deformities necessitate greater soft tissue release.
*
Rotational Malalignment:
While primarily a coronal plane deformity, varus knees can also present with subtle or significant tibial internal rotation or femoral external rotation, impacting patellofemoral tracking and overall knee kinematics.
Indications & Contraindications
Indications
The primary indications for TKA in the varus knee align with general TKA principles, with specific considerations for the varus morphology.
-
End-stage arthritis associated with pain and dysfunction that has failed nonoperative treatment. This remains the cornerstone indication.
- Pain: Severe, persistent knee pain, often localized to the medial compartment, that significantly impacts activities of daily living, sleep, and quality of life.
- Dysfunction: Progressive loss of range of motion, ambulation difficulties, inability to perform routine activities, and symptomatic limb malalignment.
- Failure of Nonoperative Management: This includes physical therapy, anti-inflammatory medications, corticosteroid injections, viscosupplementation, and activity modification, over an appropriate duration (typically 3-6 months).
-
Radiographic Evidence:
Advanced degenerative changes, including joint space narrowing, subchondral sclerosis, osteophyte formation, and significant medial compartment bone loss, as seen on standing radiographs.
-
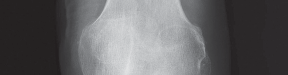
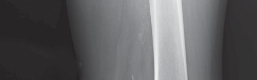
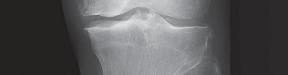
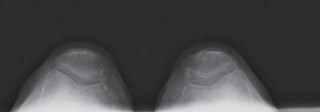
- Fig. 1A: Anteroposterior (AP) radiograph demonstrating severe medial compartment osteoarthritis with joint space narrowing and subchondral sclerosis.
-
- Fig. 1B: Lateral radiograph revealing osteophyte formation and patellofemoral degenerative changes.
-

- Fig. 1C: Merchant's view showing patellofemoral articulation.
-

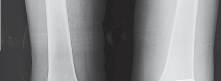
- Fig. 2A: Standing long-leg alignment radiograph demonstrating significant varus malalignment with the mechanical axis passing medial to the knee center.
-

- Fig. 2B: Postoperative standing long-leg alignment radiograph demonstrating restoration of neutral mechanical alignment.
-
-
Significant Coronal Plane Deformity: Typically defined as >5-10 degrees of varus on standing long-leg films, especially if associated with symptomatology.
-

- Fig. 3A: Preoperative weight-bearing AP view demonstrating severe medial compartment collapse and varus angulation.
-
- Fig. 3B: Valgus stress radiograph. This view is crucial to determine if the varus deformity is fixed or correctable. A correctable deformity typically requires less aggressive medial soft tissue release intraoperatively.
-
- Fig. 3C: Another long-leg alignment illustrating a more subtle but significant varus deformity.
-

- Fig. 3D: Magnified view of the medial compartment showing severe bone loss and osteophytes.
-
-
Inflammatory Arthritis: Conditions such as rheumatoid arthritis leading to varus deformity, often with associated bone loss and ligamentous laxity.
-
Post-traumatic Arthritis: Resulting from intra-articular fractures or ligamentous injuries, leading to malalignment and degenerative changes.
Contraindications
-
Absolute Contraindications:
- Active infection in the knee or elsewhere in the body (e.g., active cutaneous infection, urinary tract infection, dental abscess).
- Reflex sympathetic dystrophy.
- Extensor mechanism dysfunction preventing ambulation (e.g., quadriceps paralysis).
- Significant vascular compromise of the limb.
- Uncontrolled medical comorbidities that pose excessive anesthetic or surgical risk.
-
Relative Contraindications:
- Morbid obesity.
- Peripheral neuropathy or neuromuscular disorders.
- Severe, rapidly progressing osteopenia.
- Young patient age (<55 years old) if other options are viable, though this is evolving.
- Arterial insufficiency requiring revascularization.
- Prior knee arthrodesis, which significantly complicates soft tissue balancing.
Table: Operative vs. Non-Operative Indications
| Feature | Non-Operative Treatment Indicated | Operative Treatment (TKA) Indicated |
|---|---|---|
| Pain Level | Mild to moderate, intermittent, responsive to conservative care. | Severe, debilitating, persistent despite non-operative therapy. |
| Functional Limitation | Minimal impact on daily activities; able to modify activities. | Significant impairment in ADLs, gait, and quality of life. |
| Radiographic Findings | Mild to moderate osteoarthritis, minimal joint space narrowing. | End-stage arthritis (Kellgren-Lawrence Grade III-IV), severe joint space narrowing, subchondral sclerosis, osteophytes, significant bone loss, varus malalignment. |
| Response to Treatment | Symptomatic relief with NSAIDs, PT, injections, weight management. | Failure of extensive non-operative regimen (usually 3-6 months). |
| Knee Stability | Stable with intact ligaments. | Medial compartment instability or fixed varus deformity. |
| Patient Expectations | Realistic goals for symptom management and activity modification. | Realistic expectations for pain relief, functional improvement, and recovery. |
| Medical Comorbidities | Uncontrolled or severe comorbidities increasing surgical risk. | Well-controlled comorbidities; acceptable surgical risk. |
| Infection | No active infection. | No active infection. |
Pre-Operative Planning & Patient Positioning
Meticulous preoperative planning is the cornerstone of successful TKA, particularly in the varus knee, where precise deformity correction and soft tissue balancing are critical.
Clinical Assessment
- History: Detailed history of pain, dysfunction, prior knee injuries, surgeries, and medical comorbidities.
-
Physical Examination:
- Gait Analysis: Observe the patient's gait for a varus thrust or instability.
- Alignment: Clinically assess standing alignment.
- Range of Motion: Measure flexion and extension. Note any fixed flexion contracture.
- Stability: Crucially, assess knee stability with varus and valgus stress in both extension and 30 degrees of flexion. As noted in the seed content, examination of the knee with valgus stress is useful to determine if the varus deformity is fixed or correctable. A correctable deformity may not need a significant medial release intraoperatively. This differentiates between a purely bony deformity and one with significant medial soft tissue contracture.
- Neurovascular Exam: Perform a thorough examination to rule out any pre-existing deficits.
- Extensor Mechanism: Assess patellar tracking and quadriceps strength.
Radiographic Assessment
-
Plain Radiographs:
- Standing Anteroposterior (AP), Lateral, and Merchant's views: These provide initial assessment of joint space narrowing, osteophyte burden, and patellofemoral pathology (as shown in Fig. 1A, 1B, 1C).
- Standing Full-Length Hip-to-Ankle (Long-Leg Alignment) Radiographs: These are indispensable for accurate assessment of the mechanical axis and quantification of the varus deformity (Fig. 2A, 2B, 3C). They allow for templating of component sizes, determining the required femoral valgus cut angle, and anticipating potential bone loss.
- Stress Radiographs: Valgus stress radiographs in extension and 30 degrees of flexion help differentiate between fixed and reducible varus deformity (Fig. 3B). This directly influences the extent of medial soft tissue release required.
-
Special Imaging (as indicated):
-
Computed Tomography (CT) Scan:
Useful for assessing complex deformities, severe bone loss, or significant rotational malalignment of the femur or tibia, especially in cases of post-traumatic arthritis or prior osteotomies. This aids in precise rotational component positioning.
-

- Fig. 4A: Axial CT image demonstrating femoral rotation (e.g., posterior condylar axis).
-
- Fig. 4B: Coronal CT image showing significant medial tibial bone loss.
-
-
Magnetic Resonance Imaging (MRI):
Rarely indicated for primary TKA, but may be considered if concomitant soft tissue pathology (e.g., meniscal tear, osteonecrosis) or occult pathology is suspected, particularly in younger patients.
-
- Fig. 5A: Sagittal MRI view illustrating cartilage degeneration and subchondral bone changes.
-

- Fig. 5B: Coronal MRI view depicting extensive medial compartment osteoarthritis and potential meniscal extrusion.
-
- Fig. 5C: Axial MRI view providing additional information on patellofemoral tracking and rotational alignment.
-
-
Computed Tomography (CT) Scan:
Useful for assessing complex deformities, severe bone loss, or significant rotational malalignment of the femur or tibia, especially in cases of post-traumatic arthritis or prior osteotomies. This aids in precise rotational component positioning.
Templating and Implant Selection
- Component Sizing: Template femoral and tibial components using calibrated long-leg radiographs to estimate sizes, anticipating bone resections and potential augments.
-
Implant Type:
- Cruciate Retaining (CR): If the PCL is functional and the deformity is mild to moderate.
- Posterior Stabilized (PS): Most commonly used in varus knees, as it simplifies soft tissue balancing by excising the PCL, which can be contracted, and provides inherent posterior stability.
- Constrained Condylar Knee (CCK) / Hinge: Reserved for severe deformities with significant ligamentous instability, severe bone loss, or revision cases where primary balancing cannot achieve stability.
- Augments/Stems: Plan for bone augments or stems for cases with severe medial tibial bone loss or metaphyseal defects, to ensure adequate implant support and prevent subsidence.
-
Rotational Alignment:
Pre-plan femoral and tibial rotational alignment based on anatomical landmarks (e.g., Whiteside's line, posterior condylar axis, tibial tubercle).
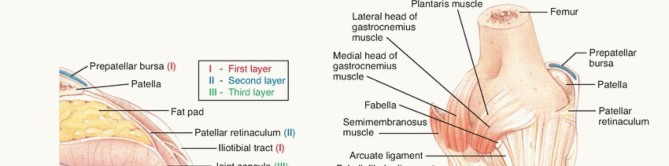
-
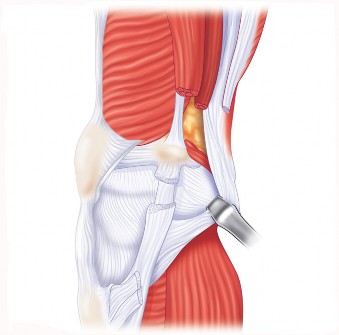
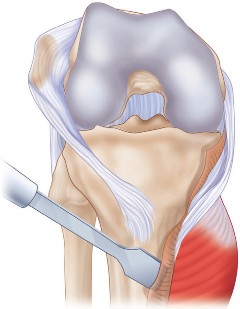
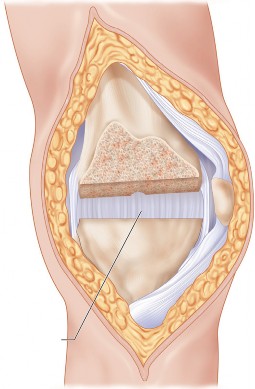
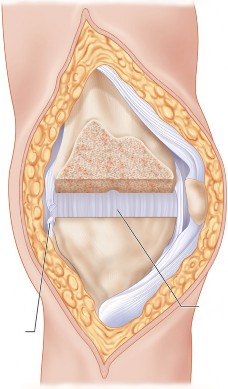
- Fig. 6A: Anatomical illustration of knee ligaments, highlighting the MCL and LCL.
-
- Fig. 6B: Diagram illustrating femoral condylar anatomy and common axes used for rotational alignment.
-
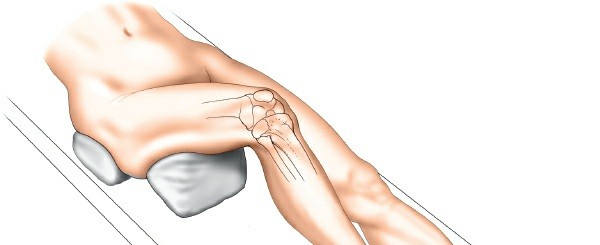
Patient Positioning
- Supine Position: The patient is positioned supine on the operating table.
- Tourniquet: A pneumatic tourniquet is applied to the proximal thigh, typically inflated after exsanguination.
- Leg Holder: A knee-flexion support or leg holder may be used to provide stable positioning for bone cuts and soft tissue balancing. The contralateral limb is typically abducted and flexed to allow full access to the operative knee.
- Sterile Prep and Drape: Standard sterile preparation and draping are performed.
Detailed Surgical Approach / Technique
The surgical technique for TKA in a varus knee emphasizes precise bone resections, meticulous soft tissue balancing, and careful component positioning to restore a neutral mechanical axis and provide a stable, functional knee.
1. Incision and Exposure
-
Midline Skin Incision:
A straight midline skin incision is made, extending from approximately 3-4 cm proximal to the patella to just medial to the tibial tubercle.
-
- Fig. 7A: Surgical image showing a typical midline skin incision for TKA.
-
-
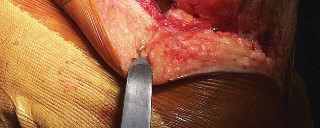
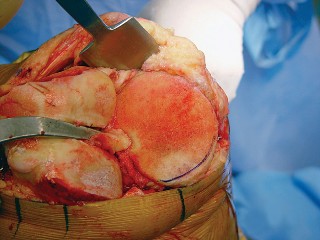
Medial Parapatellar Arthrotomy:
The approach of choice for most primary TKAs. An incision is made through the medial retinaculum, vastus medialis obliquus, and joint capsule. The patella is then everted laterally.
-

- Fig. 7B: Surgical image demonstrating exposure of the knee joint after medial parapatellar arthrotomy and patellar eversion.
-
2. Bone Resection
The goal is to achieve balanced rectangular flexion and extension gaps perpendicular to the mechanical axis.
-
Distal Femoral Resection:
- An intramedullary (IM) or extramedullary (EM) guide can be used. IM guides are common but require careful determination of the valgus cut angle. In a varus knee, the distal femur is often laterally compensated, so the anatomical valgus angle may be less than the typical 5-7 degrees. Preoperative long-leg radiographs are critical to determine the patient-specific valgus angle.
- The distal femoral cut establishes the extension gap. The standard resection is 9 mm from the most prominent femoral condyle (usually the lateral in a varus knee) to accommodate common femoral components.
-
- Fig. 8A: Surgical image showing the intramedullary alignment rod being inserted into the femoral canal.
-
- Fig. 8B: Surgical image demonstrating the distal femoral cutting block secured in place, ready for resection.
-
Proximal Tibial Resection:
- An extramedullary guide is preferred for tibial cuts to align the component perpendicular to the mechanical axis of the tibia.
- The cut typically aims for 0-3 degrees of varus/valgus relative to the mechanical axis and 3-5 degrees of posterior slope.
- In varus knees, significant medial tibial bone loss is common. The initial cut should be referenced from the least affected portion of the tibial plateau, often the lateral side, to ensure adequate bone removal from the collapsed medial side. Over-resection of the lateral tibia to match the medial defect must be avoided, as this can lead to joint line elevation.
- If significant medial bone loss is present, the initial cut may be set to resect only enough bone to remove sclerotic bone and provide a stable seating for the component. Subsequent balancing and potential augments/stems will address the defect.
-

- Fig. 9A: Surgical image depicting the extramedullary tibial cutting guide aligned to the mechanical axis of the tibia.
-

- Fig. 9B: Surgical image demonstrating the proximal tibial resection being performed with an oscillating saw.
3. Gap Balancing and Soft Tissue Release (Critical for Varus Knee)
Achieving balanced, symmetrical flexion and extension gaps is paramount. In varus knees, this primarily involves releasing contracted medial structures. The sequential medial release technique is commonly employed.
*
Assessment of Gaps:
After the initial bone cuts, trial spacers or tensioning devices are used to assess the flexion and extension gaps.
*
Extension Gap:
Assessed at full extension. In a varus knee, the medial extension gap will be tight, and the lateral gap may be lax.
*
Flexion Gap:
Assessed at 90 degrees of flexion. The medial flexion gap may also be tight, often due to contracted deep MCL and posterior oblique ligament.
*

*
Fig. 10A:
Surgical image demonstrating gap assessment in extension using a spacer block. Note the tight medial compartment.
*

*
Fig. 10B:
Surgical image illustrating gap assessment in flexion, revealing potential medial tightness.
-
Sequential Medial Soft Tissue Release: This is a step-wise approach to release the contracted medial structures to achieve a rectangular, balanced extension gap.
- Medial Osteophytes: Remove all medial osteophytes from the distal femur and proximal tibia first.
-
Superficial MCL (sMCL):
Release the posteromedial capsule and the deep layers of the sMCL from the proximal tibia, often starting from posterior and moving anteriorly. This can be performed with a subperiosteal elevation using a Cobb elevator or periosteal elevator. Pie-crusting (puncturing the sMCL without complete transection) can also be used for more subtle releases.
-

- Fig. 11A: Surgical image showing a Cobb elevator being used to release contracted soft tissues from the medial tibial plateau.
-
- Deep MCL (dMCL) and Posteromedial Capsule: If further release is needed, the deep MCL and posterior oblique ligament are released from the tibia. This is typically done in conjunction with the sMCL release or as a distinct, deeper step.
- Semimembranosus Attachments: In severe varus deformities, the insertion of the semimembranosus tendon onto the posterior medial tibia can be contracted and require release.
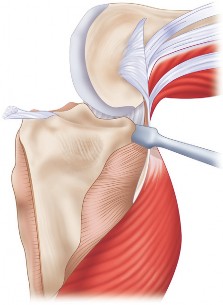
-
PCL Release (if using PS implant):
If a posterior-stabilized implant is chosen, the PCL is resected. This further opens the flexion gap and simplifies balancing.
-
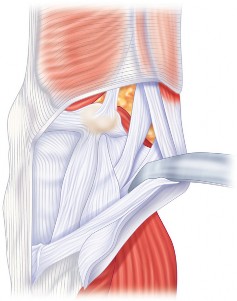
- Fig. 22A: Surgical image depicting the posterior aspect of the knee, potentially showing PCL excision or posterior capsule release.
-
- Fig. 22B: Another view of the posterior knee, highlighting structures relevant to posterior balancing.
-
-

- Fig. 11B: Surgical image demonstrating the use of a tensioning device to assess the medial compartment release and ensure adequate gap equalization.
-
Flexion Gap Balancing: After achieving a balanced extension gap, the flexion gap is assessed.
- If the flexion gap remains tight, femoral component rotation is crucial. The femoral component should be externally rotated 3 degrees relative to the posterior condylar axis or perpendicular to Whiteside's line (epicondylar axis) to balance the flexion gap. Excessive external rotation can lead to mediolateral imbalance and instability.
- If the flexion gap is still tight after optimal rotation, further posterior capsular release or, rarely, small additional bone resection from the posterior femoral condyles may be necessary.
4. Patellar Preparation and Tracking
- Patellar Resection: The patella is prepared by resecting approximately 7-9 mm from its posterior surface, aiming to restore pre-arthritic patellar thickness.
-
Patellar Tracking:
After trial components are placed, patellar tracking is assessed through a full range of motion. The "no thumb test" can be employed.
- Lateral Release: If there is persistent lateral patellar tilt or subluxation, a lateral retinacular release may be performed. This involves releasing the lateral retinaculum from the patella to the vastus lateralis, carefully avoiding the superior lateral geniculate artery.
-
- Fig. 12A: Surgical image showing assessment of patellar tracking through knee flexion and extension.
5. Trial Reduction and Final Assessment
-
Trial Components:
Femoral, tibial, and patellar trial components are inserted.
-
- Fig. 13A: Surgical image depicting the femoral and tibial trial components in situ.
-

- Fig. 13B: Surgical image demonstrating range of motion assessment with trial components, ensuring full extension and adequate flexion.
-
- Stability and Range of Motion: Assess for full extension and flexion. Check stability in varus/valgus stress throughout the range of motion. The knee should be stable with minimal laxity, particularly in extension and 30 degrees of flexion.
-
Rotational Alignment:
Verify correct femoral and tibial rotational alignment.
-

- Fig. 17A: Surgical image showing instruments used to check femoral component rotation.
-
- Fig. 17B: Another view of rotational alignment verification on the femoral side.
-
-
Addressing Bone Defects:
If significant medial tibial bone loss remains after initial cuts, metal augments or bone graft may be used to fill the defect and provide a stable base for the tibial component.
-

- Fig. 18A: Surgical image illustrating the use of a metal augment for a significant medial tibial bone defect.
-
- Fig. 18B: Another view showing the augment securely attached to the tibial baseplate.
-
- Fig. 16A: Surgical image demonstrating customized instrumentation or navigation system for complex deformities.
-

- Fig. 16B: Close-up of specialized cutting blocks designed to address specific bone defects.
-
For very severe instability or bone loss, a more constrained implant (CCK or hinge) may be necessary.
-

- Fig. 21A: Surgical image of a constrained condylar knee (CCK) femoral trial.
-

- Fig. 21B: A CCK tibial baseplate with a post, indicating a more constrained articulation.
-
-
6. Final Component Implantation and Closure
-
Cementation:
Remove trials. The bone surfaces are cleaned and dried. Bone cement (methyl methacrylate) is mixed and applied to the bone surfaces and the internal aspects of the components.
-
- Fig. 14A: Surgical image showing the application of bone cement to the prepared femoral condyles.
-
-
Component Implantation:
The femoral, tibial, and patellar components are implanted and held in position until the cement cures.
-

- Fig. 14B: Surgical image of the final femoral component being seated.
-
- Wound Closure: The knee is thoroughly irrigated. The joint capsule and retinaculum are repaired. The subcutaneous tissues are closed, followed by skin closure.
7. Post-Implantation Radiographs (Initial Assessment)
-

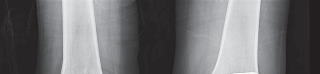
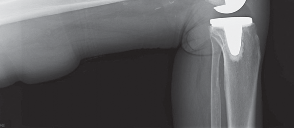
- Fig. 15A: Post-operative AP radiograph showing well-aligned components and restoration of the joint space.
-

- Fig. 15B: Post-operative lateral radiograph demonstrating appropriate component positioning and posterior slope.
-
- Fig. 15C: Post-operative standing long-leg alignment radiograph confirming restoration of a neutral mechanical axis.
Complications & Management
While TKA is generally safe and effective, complications can occur, particularly in the technically demanding varus knee. Understanding these complications and their management is crucial for all orthopedic surgeons.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (%) | Salvage Strategies |
|---|---|---|
| Infection | 0.5-2 |
Acute (<4 weeks):
Irrigation and debridement with polyethylene exchange, parenteral antibiotics.
Chronic (>4 weeks) or failed I&D: Two-stage revision (implant removal, antibiotic spacer, parenteral antibiotics, reimplantation) or one-stage revision in selected cases. Arthrodesis or amputation for intractable cases. 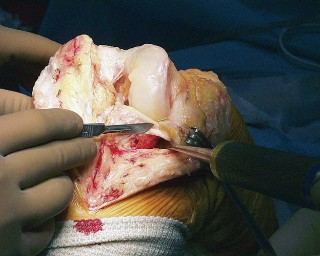 Fig. 20A:
Clinical image of a wound complication, potentially infection or delayed healing.
Fig. 20A:
Clinical image of a wound complication, potentially infection or delayed healing.
|
| Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) | DVT: 5-20 (symptomatic), PE: 0.5-2 (symptomatic) |
DVT:
Anticoagulation (oral or parenteral).
PE: Systemic anticoagulation. IVC filter for recurrent PE or contraindication to anticoagulation. |
| Periprosthetic Fracture | 0.5-2 |
Intraoperative:
Immediate fixation (screws, wires, plates) or conversion to a constrained implant/long-stemmed components.
Postoperative: Non-operative management (bracing) for stable, non-displaced fractures. Open reduction and internal fixation (ORIF) with plates/screws for unstable fractures. Revision arthroplasty with constrained or hinged implants and stems for complex fractures or implant loosening. 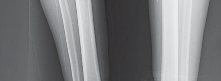 Fig. 19A:
Post-operative radiograph demonstrating a periprosthetic fracture of the distal femur.
Fig. 19A:
Post-operative radiograph demonstrating a periprosthetic fracture of the distal femur.
|
| Instability (Flexion/Extension Gap Mismatch) | 2-5 |
Recurrent Varus (medial instability):
If mild, bracing and physical therapy. If severe, revision TKA with increased polyethylene thickness, medial ligament plication, or conversion to a more constrained implant (CCK).
Recurrent Valgus (lateral instability from over-release): Revision TKA with thicker polyethylene, often requiring a constrained or hinged implant. |
| Stiffness / Arthrofibrosis | 2-10 |
Early (<3 months):
Aggressive physical therapy, manipulation under anesthesia (MUA).
Late (>3 months): Arthroscopic or open arthrolysis. Revision TKA for severe, intractable stiffness. |
| Aseptic Loosening | 1-3 |
Revision TKA with component exchange, often involving augments, stems, and bone grafting. Addressing mechanical malalignment or implant-related factors.
 Fig. 19B:
Radiograph showing evidence of tibial component loosening with lucency at the cement-bone interface.
Fig. 19B:
Radiograph showing evidence of tibial component loosening with lucency at the cement-bone interface.
|
| Patellofemoral Complications | 2-5 |
Patellar Maltracking/Tilt:
Physical therapy, lateral release.
Patellar Fracture: Non-operative for non-displaced. ORIF or patellectomy (partial/total) for displaced/comminuted fractures. Patellar Clunk Syndrome: Arthroscopic debridement. |
| Nerve Injury | <1 | Most common: peroneal nerve (lateral popliteal nerve). Management is typically conservative (observation, bracing). Surgical neurolysis for persistent deficit if indicated. |
| Vascular Injury | <0.1 | Immediate surgical exploration and vascular repair. May require graft interposition. |
| Persistent Pain | 5-15 |
Rule out infection, aseptic loosening, instability, malalignment, patellofemoral issues, complex regional pain syndrome. Address underlying cause; multidisciplinary pain management. Revision TKA if a correctable mechanical issue is identified.
 Fig. 20B:
Surgical image potentially showing a revision procedure for a painful TKA.
Fig. 20B:
Surgical image potentially showing a revision procedure for a painful TKA.
|
Specific Complications in the Varus Knee
- Persistent Varus or Medial Compartment Instability: This is a key concern. If inadequate medial release is performed, the knee may remain in varus or be unstable medially. Conversely, over-release of the MCL can lead to valgus instability. Careful intraoperative soft tissue balancing is critical. If persistent varus is noted postoperatively, treatment options range from observation and bracing to revision TKA with further medial release and/or more constrained implants.
- Peroneal Nerve Palsy: The peroneal nerve is susceptible to traction injury during severe varus deformity correction, especially with a fixed flexion contracture. This is due to the abrupt lengthening of the lateral structures. Preoperative neurological assessment, intraoperative vigilance, and avoiding excessive correction are important. Postoperatively, observation is typically indicated, as most deficits resolve spontaneously. An ankle-foot orthosis may be needed.
- Joint Line Elevation/Depression: Improper tibial resection in cases of severe medial tibial bone loss can lead to joint line elevation (if too little bone is resected laterally) or depression (if too much bone is resected medially). This can compromise knee kinematics and patellofemoral function. Preoperative templating and using augments for bone defects are crucial.
Post-Operative Rehabilitation Protocols
A structured and progressive post-operative rehabilitation protocol is essential for optimizing outcomes following TKA in the varus knee, focusing on pain management, range of motion, strength recovery, and functional independence.
Phase I: Immediate Post-Operative (Days 0-7)
- Goals: Pain control, minimize swelling, achieve early knee flexion and full extension, independent transfers, protected weight-bearing.
- Weight-Bearing: As tolerated with an assistive device (walker, crutches), typically full weight-bearing.
-
Range of Motion (ROM):
- Continuous Passive Motion (CPM) machine: May be used, though its routine benefit is debated.
- Active-assisted and passive ROM exercises: Focus on achieving 0 degrees extension and 90 degrees flexion by discharge.
- Patellar mobilizations: To prevent adhesions.
-
Strengthening:
- Quad sets, gluteal sets, ankle pumps.
- Straight leg raises (SLR) in supine, with assistance if quadriceps lag.
- Gentle hamstring curls.
- Mobility: Bed mobility, sit-to-stand transfers, short distance ambulation with assistive device.
-
Cryotherapy and Compression:
Essential for managing pain and swelling.
-

- Fig. 23A: Patient demonstrating early post-operative knee flexion exercises.
-
Phase II: Early Recovery (Weeks 2-6)
- Goals: Improve ROM (aim for 0-110+ degrees), increase strength, progress ambulation, reduce reliance on assistive devices.
- ROM: Continue with active and passive flexion and extension exercises. Incorporate wall slides, heel slides, prone hangs.
-
Strengthening:
- Progressive resistive exercises: Quadriceps strengthening (mini-squats, leg presses, step-ups), hamstring curls, calf raises.
- Balance and proprioception exercises: Single leg stance with support.
- Mobility: Wean off assistive devices as tolerated. Increase ambulation distance. Stair climbing practice.
- Scar Mobilization: Begin once the incision is well-healed to prevent adhesions.
Phase III: Functional Progression (Weeks 7-12)
- Goals: Normalize gait, achieve functional ROM (0-120+ degrees), maximize strength, return to light recreational activities.
- ROM: Continue to work on flexion, aiming for functional range.
-
Strengthening:
- Advanced closed-chain exercises: Lunges, deeper squats, stationary cycling.
- Open-chain exercises for specific muscle groups.
- Balance and Agility: Progress to dynamic balance exercises.
-
Activity Integration:
Low-impact activities (swimming, cycling) can be introduced.
-
- Fig. 23B: Patient engaging in physical therapy exercises to improve strength and range of motion.
-
Phase IV: Advanced Activity / Return to Sport (Months 3+)
- Goals: Continue strength and endurance training, return to desired activities (low-impact sports).
- Progression: Gradual increase in intensity and duration of exercises. Sport-specific training for approved activities.
- Patient Education: Emphasize lifelong adherence to exercise, avoidance of high-impact activities (running, jumping), and maintenance of a healthy weight.
Key Considerations for Varus Knee Rehabilitation
- Pain Management: Patients may experience more initial pain due to extensive soft tissue release. Aggressive multimodal pain management is crucial.
- Early Extension: Achieving full extension early is critical to prevent a fixed flexion contracture, which can compromise long-term function and lead to pain.
- Quadriceps Strength: Varus knees often have significant quadriceps weakness preoperatively. Aggressive quadriceps strengthening is essential for regaining functional mobility.
- Patient Compliance: Emphasize the importance of patient adherence to the rehabilitation program for optimal outcomes.
Summary of Key Literature / Guidelines
The literature on total knee arthroplasty in the varus knee consistently highlights the importance of restoring neutral mechanical alignment and achieving balanced flexion and extension gaps. Key themes and consensus points include:
- Mechanical Alignment Philosophy: The long-standing gold standard remains restoration of the neutral mechanical axis (0 ± 3 degrees varus/valgus) in the coronal plane. Studies by Insall, Ranawat, and others have demonstrated improved long-term implant survival with this approach. While kinematic alignment has gained recent interest, its applicability and long-term outcomes in severe varus deformities, particularly those with significant bone loss and ligamentous contractures, are still under investigation and may carry higher risks of instability if not meticulously executed.
- Sequential Soft Tissue Release: The efficacy of sequential medial soft tissue release for correcting varus deformity and balancing the knee in extension is well-established. Numerous cadaveric and clinical studies detail the order of release, starting with medial osteophytes, followed by the superficial MCL (often posterior fibers first), deep MCL, and potentially semimembranosus attachments. The importance of stress radiographs in determining the fixity of the deformity and guiding the extent of release is emphasized.
- Femoral Component Rotation: Achieving proper femoral component rotation is critical for balancing the flexion gap and ensuring optimal patellofemoral tracking. References like Whiteside's line (perpendicular to the deepest part of the trochlear groove) and the transepicondylar axis are primary anatomical landmarks, often with a 3-degree external rotation relative to the posterior condylar axis.
- Management of Bone Defects: The management of medial tibial bone loss is a recurring challenge. Literature supports the use of metal augments for contained defects greater than 5 mm, or stem extensions for larger defects to provide stability and prevent subsidence. Autograft or allograft bone chips can also be used, though often require more robust mechanical support from the implant.
- Implant Selection: While most varus knees can be managed with cruciate-retaining or posterior-stabilized designs, the literature indicates an increasing use of PS designs in moderate to severe varus deformities due to their ability to simplify soft tissue balancing by excising the PCL. Constrained condylar knee (CCK) implants are reserved for cases with severe ligamentous insufficiency or significant bone loss where primary balancing cannot achieve stability, or in revision settings.
- Outcomes: Modern TKA for varus knee deformities consistently reports excellent long-term outcomes, with 10-year survivorship rates exceeding 90-95% in many series. However, patient satisfaction, while generally high, can be impacted by residual pain, stiffness, or subtle instability, underscoring the importance of meticulous surgical technique and comprehensive rehabilitation. Specific attention to balancing in the varus knee has been shown to improve functional scores and reduce revision rates for instability.
- Computer-Assisted Navigation and Robotics: Emerging literature suggests that computer-assisted navigation and robotic-assisted TKA may offer advantages in achieving more precise bone cuts and objective soft tissue balancing in complex varus deformities, potentially reducing outliers in mechanical alignment. However, their impact on long-term clinical outcomes and cost-effectiveness compared to conventional techniques is still being evaluated.
In conclusion, successful TKA in the varus knee necessitates a comprehensive understanding of the pathology, meticulous preoperative planning, and a systematic approach to bone resection and soft tissue balancing. Adherence to these expert surgical strategies is crucial for optimizing outcomes and minimizing complications.
Clinical & Radiographic Imaging




You Might Also Like