Tibial Plateau Fractures: Your Guide to Causes, Treatment & Recovery
Key Takeaway
Looking for accurate information on Tibial Plateau Fractures: Your Guide to Causes, Treatment & Recovery? Tibial plateau fractures are breaks in the flat top portion of the tibia bone, forming part of the knee joint. These are typically high-energy injuries from falls or accidents, often damaging both bone and overlying cartilage. Treatment for tibial plateau fractures can involve bracing, splinting, or surgery, depending on severity, and requires a period of non-weight bearing to heal.
Tibial Plateau Fractures: Your Guide to Causes, Treatment & Recovery
Introduction & Epidemiology
Tibial plateau fractures represent a challenging subset of intra-articular injuries of the knee, demanding meticulous surgical planning and execution to restore articular congruity, axial alignment, and knee stability. The knee joint, a complex articulation between the distal femur and the proximal tibia, is crucial for both mobility and weight-bearing. Fractures involving the tibial plateau disrupt the load-bearing surface, leading to significant functional impairment if not appropriately managed.
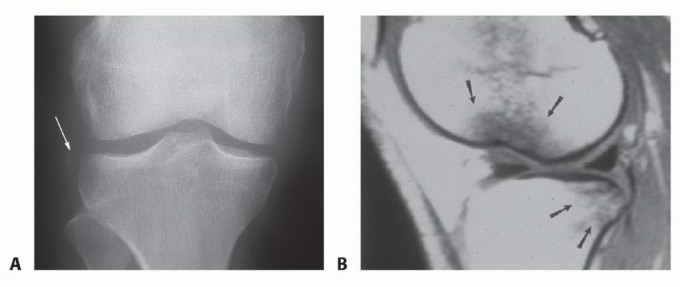
The mechanism of injury is typically characterized by an axial load combined with a varus or valgus moment applied to the knee. This often occurs in high-energy trauma, such as motor vehicle accidents (MVAs) or falls from height, particularly in younger, active individuals. In these contexts, associated soft tissue injuries, including meniscal tears (up to 50%), ligamentous disruptions (e.g., ACL, MCL, LCL, PCL in 10-40%), and neurovascular compromise (popliteal artery injury in 3-10%, peroneal nerve palsy in 2-15%), are common and must be thoroughly evaluated. Conversely, in the elderly population, lower-energy mechanisms, such as simple falls, can result in tibial plateau fractures due to osteoporotic bone. This bimodal distribution of incidence highlights the diverse patient demographic and fracture patterns encountered.

Figure 2: Knee X-rays illustrating a tibial plateau fracture.
Understanding the unique biomechanical forces and associated injuries is paramount for accurate diagnosis, classification, and treatment planning. The ultimate goal is to achieve a stable, well-aligned knee with preserved articular cartilage integrity, thereby minimizing the risk of post-traumatic osteoarthritis (PTOA) and optimizing long-term functional outcomes.
Surgical Anatomy & Biomechanics
The proximal tibia is a critical anatomical region that forms the inferior aspect of the knee joint. Its complex architecture, comprising cortical bone, cancellous bone, and articular cartilage, dictates fracture patterns and influences surgical strategies.
Bony Anatomy
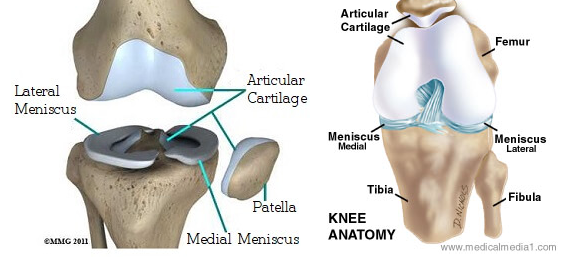
The tibial plateau is the expanded, flat superior surface of the tibia, divided into medial and lateral condyles by the intercondylar eminence (tibial spines).
*
Medial Tibial Condyle:
Typically larger, stronger, and more concave than the lateral condyle. It bears approximately 60% of the axial load. The posteromedial aspect is particularly robust.
*
Lateral Tibial Condyle:
Smaller, weaker, and convex, making it more susceptible to depression fractures. Its anterior and posterior slopes are significant for knee kinematics.
*
Intercondylar Eminence:
Consists of medial and lateral tibial spines, which provide attachments for the anterior and posterior cruciate ligaments. Fractures involving the eminence can lead to knee instability.
*
Tibial Tuberosity:
Located anteriorly, serves as the insertion site for the patellar tendon. Its integrity is important for extensor mechanism function.
*
Metaphyseal Flare:
The region immediately distal to the articular surface, composed of highly vascular cancellous bone. It provides crucial support for the articular fragments and is often comminuted in high-energy injuries.

Figure 1: Diagrammatic representation of the tibial plateau anatomy.
Articular & Soft Tissue Structures
- Articular Cartilage: The smooth, hyaline cartilage covering the tibial condyles facilitates frictionless movement. Injury to this surface is a primary determinant of long-term prognosis.
- Menisci: The medial and lateral menisci are C-shaped (medial) and O-shaped (lateral) fibrocartilaginous structures that sit between the femur and tibia. They act as shock absorbers, load distributors, and contribute to knee stability. Meniscal tears are highly associated with tibial plateau fractures, particularly lateral meniscus tears (up to 50-70% in lateral condyle fractures) and medial meniscus tears (less common, but significant when present).
- Cruciate Ligaments: The anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) originate from the intercondylar eminence and are vital for anteroposterior stability. Avulsion fractures of their insertions can occur.
- Collateral Ligaments: The medial collateral ligament (MCL) resists valgus stress, and the lateral collateral ligament (LCL) resists varus stress. These provide mediolateral stability. Injuries to these ligaments are common in fracture dislocations.
- Extensor Mechanism: Comprises the quadriceps muscle, quadriceps tendon, patella, patellar tendon, and tibial tuberosity. Essential for knee extension.
Neurovascular Structures
The popliteal fossa houses critical neurovascular structures at risk during tibial plateau fractures and their surgical management:
*
Popliteal Artery and Vein:
Positioned posteriorly, immediately against the posterior aspect of the proximal tibia. They are susceptible to stretch, compression, or laceration in displaced fractures, particularly posteromedial or bicondylar patterns.
*
Peroneal Nerve:
Located superficially on the lateral aspect of the fibular neck, it is vulnerable to direct trauma, traction, or iatrogenic injury during lateral approaches. It supplies sensation to the dorsum of the foot and motor function to the ankle dorsiflexors and evertors.
Biomechanics of Fracture
Tibial plateau fractures result from complex loading patterns:
*
Axial Load with Valgus Stress:
Most common mechanism, typically resulting in lateral condyle fractures (Schatzker I, II, III). The lateral femoral condyle acts as a wedge, driving into the lateral tibial plateau.
*
Axial Load with Varus Stress:
Less common, leading to medial condyle fractures (Schatzker IV). The medial femoral condyle drives into the medial tibial plateau. These are often high-energy and associated with significant soft tissue injury.
*
High-Energy Axial Load:
Can lead to bicondylar fractures (Schatzker V, VI) with significant comminution, metaphyseal-diaphyseal dissociation, and extensive soft tissue damage.
*
Posterior Shearing Force:
Can cause posterior condylar fractures, often associated with knee dislocation or dashboard injuries.
Understanding these biomechanical principles, combined with a detailed appreciation of surgical anatomy, is fundamental for accurate classification, comprehensive pre-operative planning, and successful execution of reduction and fixation strategies.
Indications & Contraindications
The decision between operative and non-operative management for tibial plateau fractures hinges on a careful assessment of fracture characteristics, patient factors, and associated injuries.
Non-Operative Indications
Non-operative management is typically reserved for stable fractures with minimal displacement and no significant articular involvement.
*
Minimally Displaced/Depressed Fractures:
* Articular step-off < 2-3 mm
* Condylar widening < 5 mm
* Stable knee on stress radiographs (indicating intact ligaments)
*
Non-Articular Fractures:
E.g., avulsion of intercondylar eminence without significant articular surface involvement.
*
Non-Ambulatory Patients:
Patients with limited functional demands or significant comorbidities precluding safe surgical intervention.
*
Contraindications to Surgery:
Severe medical comorbidities, active infection, or precarious soft tissue envelope.
Management typically involves bracing (hinged knee brace), non-weight bearing for 6-12 weeks, followed by progressive rehabilitation. Close monitoring for secondary displacement or loss of reduction is critical.
Operative Indications
Surgical intervention is generally indicated for fractures that compromise joint stability, articular congruity, or mechanical alignment, or in the presence of specific associated injuries.
*
Articular Step-Off:
> 2-3 mm articular incongruity. This threshold is critical for preventing PTOA.
*
Condylar Widening/Displacement:
> 5 mm metaphyseal widening or displacement, indicating significant instability and disruption of mechanical axis.
*
Medial Condyle Fractures (Schatzker IV):
Often high-energy, inherently unstable due to the valgus forces typically applied to the knee, and at higher risk of neurovascular injury.
*
Bicondylar Fractures (Schatzker V, VI):
All bicondylar fractures require surgical stabilization due to inherent instability and loss of metaphyseal support.
*
Open Fractures:
Require urgent surgical debridement and stabilization to prevent infection.
*
Compartment Syndrome:
Requires immediate fasciotomy.
*
Vascular Injury:
Requires emergent vascular repair and fracture stabilization.
*
Associated Ligamentous Instability:
Especially if chronic instability is anticipated after fracture healing.
*
Irreducible Fractures:
Fractures where soft tissue interposition (e.g., meniscus) prevents closed reduction.
*
Patellar Instability/Tibial Tubercle Avulsion:
Disrupting the extensor mechanism.
Contraindications
-
Absolute Contraindications:
- Active local or systemic infection (relative contraindication for elective fixation, but may be managed by external fixation in emergencies).
- Severely compromised soft tissue envelope (e.g., extensive degloving injury, severe fracture blisters) precluding safe open reduction and internal fixation (ORIF). In such cases, temporizing external fixation may be employed, followed by delayed ORIF once the soft tissue condition improves.
-
Relative Contraindications:
- Significant medical comorbidities that make surgery excessively high risk (e.g., severe cardiac or pulmonary disease).
- Non-ambulatory patients with low functional demands.
- Severe osteopenia/osteoporosis where stable fixation is unlikely to be achieved with standard hardware. However, specific techniques like cement augmentation or specialized locking plates can mitigate this.
Summary of Operative vs. Non-Operative Indications
| Feature / Category | Non-Operative Management | Operative Management |
|---|---|---|
| Articular Step-Off | < 2-3 mm | > 2-3 mm |
| Condylar Widening | < 5 mm | > 5 mm |
| Stability on Stress | Stable | Unstable |
| Fracture Type (Schatzker) | Schatzker I-III (minimally displaced) | Schatzker I-IV (displaced), Schatzker V-VI (all) |
| Soft Tissue Envelope | Intact, no blisters or severe swelling | Open fracture, compartment syndrome, vascular injury, severe instability |
| Patient Factors | Low functional demand, significant comorbidities | High functional demand, good health, amenable to surgery |
| Associated Injuries | None or minor, non-surgical | Vascular injury, compartment syndrome, significant ligamentous disruption |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is paramount for successful outcomes in tibial plateau fractures. It involves detailed imaging analysis, classification, surgical timing considerations, and meticulous preparation of the surgical environment.
Imaging
- Plain Radiographs: Anteroposterior (AP), lateral, and oblique views (45° internal and external) of the knee are essential initial imaging. Full-length lower extremity alignment films can be helpful for complex deformities.
-
Computed Tomography (CT) Scan:
The gold standard for assessing articular depression, comminution, and the exact morphology of the fracture fragments.
- Thin-cut axial images, coronal, and sagittal reconstructions are crucial.
- 3D reconstructions provide invaluable insights into fragment orientation and aid in planning reduction maneuvers and hardware placement.
- Magnetic Resonance Imaging (MRI): Indicated if significant soft tissue injuries (meniscal tears, ligamentous ruptures) are suspected, especially in cases where clinical examination is limited due to pain or swelling. It helps in planning concomitant soft tissue repair.
- Angiography/CTA: If vascular injury is suspected based on clinical signs (diminished pulses, expanding hematoma, cool extremity) or specific fracture patterns (e.g., bicondylar, posteromedial displacement).
Fracture Classification and Surgical Strategy
-
Schatzker Classification:
Divides tibial plateau fractures into six types based on morphology and location:
- Type I: Split fracture of the lateral plateau.
- Type II: Split depression fracture of the lateral plateau.
- Type III: Pure depression fracture of the lateral plateau (less common).
- Type IV: Medial plateau fracture (split or depression).
- Type V: Bicondylar fracture with metaphyseal-diaphyseal dissociation.
- Type VI: Bicondylar fracture with metaphyseal-diaphyseal dissociation and transverse subcondylar fracture.
- AO/OTA Classification: A more comprehensive and detailed classification system that describes fracture location, severity, and articular involvement.
- These classifications guide the choice of surgical approach, implant selection, and reduction strategy.
Soft Tissue Assessment and Timing of Surgery
- The condition of the soft tissue envelope is a critical determinant of surgical timing.
- Acute Surgery (within 6-8 hours): Indicated for open fractures, compartment syndrome, or irreducible neurovascular compromise.
- Delayed Surgery (3-10 days): Most commonly, surgery is delayed until the "wrinkle sign" returns, indicating resolution of swelling and diminished risk of wound complications. Elevation, ice, and gentle range of motion (ROM) can aid in soft tissue recovery. Fracture blisters must be monitored; surgery through intact blisters is generally acceptable, but disrupted blisters increase infection risk.
-
Staged Protocol:
For severe soft tissue injury or highly comminuted fractures, a staged approach may be used:
- External fixation for temporary stabilization, pain control, and soft tissue recovery.
- Delayed ORIF once soft tissues permit.
Pre-Operative Patient Optimization
- Medical clearance, assessment of comorbidities.
- Prophylactic antibiotics administered pre-incision.
- Deep vein thrombosis (DVT) prophylaxis initiated.
- Pain management strategy.
Patient Positioning and Setup
- Position: Supine on a radiolucent operating table.
- Pads and Supports: A bump or bolster placed under the ipsilateral hip for internal rotation of the leg, if needed for exposure. A leg holder can be used to maintain knee flexion and stability.
- Tourniquet: A pneumatic thigh tourniquet is routinely applied for a bloodless field, though it may be released after initial exposure or reduction in cases of significant soft tissue compromise.
- C-arm Access: Ensure unrestricted intraoperative fluoroscopy access (AP, lateral, oblique views) to verify reduction and hardware placement.
- Preparation: The entire lower extremity from mid-thigh to toes is prepared and draped to allow for full ROM and potential access for bone grafting.
Detailed Surgical Approach / Technique
The goal of surgical management for tibial plateau fractures is anatomical reduction of the articular surface, restoration of mechanical alignment, and stable fixation to permit early mobilization. The specific approach and technique depend on the fracture pattern, soft tissue condition, and surgeon preference.
General Principles of Fixation
- Articular Reduction: Achieve anatomical reduction of the articular fragments, confirmed by direct visualization and fluoroscopy.
- Metaphyseal Support: Elevate depressed articular segments and fill the underlying metaphyseal void with bone graft (autograft, allograft, or synthetic bone substitute) to prevent collapse.
- Restoration of Mechanical Axis: Re-establish the correct varus/valgus and procurvatum/recurvatum alignment.
- Stable Fixation: Employ robust internal fixation (plates, screws) to maintain reduction and allow for early rehabilitation.
- Soft Tissue Preservation: Minimize soft tissue stripping to reduce the risk of wound complications and infection.
Surgical Approaches
1. Anterolateral Approach (for Lateral Condyle Fractures: Schatzker I, II, III, some IV)
- Incision: Typically a straight or slightly curved longitudinal incision centered over the lateral tibial plateau, extending from the femoral epicondyle distally to the fibular head level. Alternatively, a more oblique incision parallel to the anterior border of the fibula may be used.
- Internervous Plane: The approach proceeds between the vastus lateralis (femoral nerve) and biceps femoris (sciatic nerve, common peroneal branch) proximally, and between the tibialis anterior (deep peroneal nerve) and the peroneal muscles (superficial peroneal nerve) distally. The common peroneal nerve must be identified and protected, especially as it wraps around the fibular neck.
-
Dissection:
- Incise the skin and subcutaneous tissue.
- Carefully identify and protect the common peroneal nerve.
- Incise the deep fascia along the planned approach.
- Elevate the tibialis anterior and extensor digitorum longus from the lateral aspect of the tibia.
- Identify the iliotibial (IT) band. A longitudinal incision through the IT band, either anterior or posterior to the IT band depending on access, allows exposure of the joint capsule.
- Perform a submeniscal arthrotomy (typically elevating the lateral meniscus superiorly with traction sutures) to visualize the articular surface and depressed fragments.
-
Reduction & Fixation:
- Direct Visualization: Use small periosteal elevators or ball-tipped tampers to elevate depressed articular fragments.
- K-wire Placement: Place K-wires through small drill holes in the intact lateral cortex, under the depressed fragment, to leverage and elevate it.
- Bone Grafting: Once the articular surface is reduced, fill the metaphyseal void created by the elevation with bone graft (cancellous autograft from the ipsilateral iliac crest, allograft, or synthetic bone substitute). This provides structural support and prevents re-collapse.
- Temporary Fixation: Use K-wires or small pointed reduction clamps to hold the fragments.
- Definitive Fixation: Apply a pre-contoured periarticular locking plate (e.g., L-plate, T-plate, anatomical lateral tibial plateau plate) to buttress the lateral condyle. Place lag screws through the plate or separately to compress the articular split fragments. Ensure screws do not violate the joint space.
- Assess Stability: Check stability with a stress test and fluoroscopy.
2. Posteromedial Approach (for Medial Condyle Fractures: Schatzker IV, some V, VI involving the posteromedial corner)
- Incision: A longitudinal incision centered over the posteromedial aspect of the proximal tibia, posterior to the saphenous nerve and vein.
- Internervous Plane: No true internervous plane. Dissection is directly through the subcutaneous tissue and fascia.
-
Dissection:
- Incise skin and subcutaneous tissue.
- Carefully identify and retract the saphenous nerve and vein anteriorly.
- Identify the pes anserinus tendons (sartorius, gracilis, semitendinosus). These can be either split or retracted anteriorly.
- The semimembranosus muscle and its complex tendinous attachments are identified. The posteromedial corner of the tibia is exposed by retracting the semimembranosus posteriorly or releasing its superficial attachments.
- The posterior capsule and posterior horn of the medial meniscus can be visualized.
-
Reduction & Fixation:
- Direct Visualization: Elevate and reduce depressed fragments.
- Bone Grafting: Fill metaphyseal defects.
- Fixation: Apply a medial or posteromedial buttress plate (e.g., small fragment locking plate) designed to support the medial condyle. Ensure careful screw placement to avoid neurovascular structures located posteriorly.
3. Bicondylar Approaches (for Schatzker V, VI)
These fractures often require dual approaches or extended single approaches to address both condyles.
*
Dual Incisions:
Commonly a combination of an anterolateral and a separate posteromedial incision.
*
Staged Reduction:
Typically, one condyle is reduced and provisionally fixed first (often the more comminuted or key fragment, e.g., lateral), followed by the other. The reduction of the articular surface and reconstruction of the metaphyseal bone are prioritized.
*
Sequence:
The lateral condyle is often addressed first due to its common involvement in depression fractures. The medial condyle, particularly the posteromedial fragment, provides crucial weight-bearing support and must be robustly stabilized.
*
Anterior Midline Incision with Submeniscal Arthrotomy:
Can be used, but risks compromising the vascularity of the anterior soft tissues, especially when extensive subperiosteal dissection is performed. This approach is less favored for bicondylar fractures due to the potential for wound complications.
4. Direct Posterior Approach (for Posterior Condyle Fractures)
- Incision: Posterior midline or S-shaped incision over the popliteal fossa.
- Dissection: Requires careful dissection through the popliteal fossa, retracting neurovascular bundles. Allows direct visualization of posterior fragments.
- Fixation: Small fragment plates and screws.
Intraoperative Considerations
- Arthroscopy: Can be used concomitantly with ORIF to assess articular reduction, identify meniscal or ligamentous injuries, and perform repair. However, it can extravasate fluid into the soft tissues, potentially increasing swelling and compartment syndrome risk.
- C-Arm Fluoroscopy: Used continuously to verify reduction, screw length, and intra-articular position of hardware.
- Leg Length and Alignment: Crucial to restore. Check with full-length films if necessary.
- Associated Injuries: Meniscal tears (especially lateral) should be repaired if possible, as they contribute to load distribution and stability. Ligamentous injuries are assessed and managed based on severity (repair, reconstruction, or non-operative management).
-
Closure:
Meticulous layered closure, ensuring adequate hemostasis and drainage (if necessary) to prevent hematoma formation.

Figure 3: Intraoperative view showing a tibial plateau fracture before fixation.

Figure 4: Intraoperative image demonstrating reduction and provisional fixation with K-wires.

Figure 5: Post-fixation image illustrating plate and screw constructs used for stabilization.
Complications & Management
Tibial plateau fractures, particularly high-energy patterns, are associated with a significant rate of complications, both early and late. Proactive identification and appropriate management are crucial for mitigating adverse outcomes.
Early Complications
-
Compartment Syndrome:
- Incidence: 5-15%, higher in high-energy, bicondylar fractures.
- Description: Increased pressure within the closed fascial compartments of the leg, leading to muscle ischemia and nerve damage.
- Management: Immediate diagnosis (clinical suspicion, compartment pressure monitoring) followed by urgent four-compartment fasciotomy.
-
Neurovascular Injury:
- Incidence: Popliteal artery injury (3-10%), peroneal nerve palsy (2-15%). Higher in medial or bicondylar fractures with significant displacement.
- Description: Popliteal artery injury can lead to limb ischemia. Peroneal nerve injury can result in foot drop.
- Management: Urgent surgical exploration for vascular injury with repair/grafting. Fracture stabilization is crucial. Peroneal nerve injury is often a stretch injury; observation is common, but exploration may be considered for complete lesions or if recovery does not occur.
-
Infection:
- Incidence: Superficial 5-10%, deep 1-5%. Higher in open fractures, extensive soft tissue dissection, or prolonged surgical time.
- Description: Bacterial colonization of the wound or bone.
- Management: Prophylactic antibiotics, meticulous surgical technique, delayed definitive fixation in cases of soft tissue compromise. Superficial infections treated with wound care and oral antibiotics. Deep infections require surgical debridement, intravenous antibiotics, and potentially hardware removal.
-
Wound Complications:
- Incidence: 10-20%. Includes necrosis, dehiscence, blistering.
- Description: Impaired wound healing, particularly over the anterolateral aspect due to thin soft tissue coverage.
- Management: Judicious surgical timing (waiting for "wrinkle sign"), minimal soft tissue stripping, careful handling of skin edges, appropriate flap design. Minor dehiscence may be treated with local wound care; significant dehiscence or necrosis may require surgical debridement, negative pressure wound therapy, or flap coverage.
-
DVT/Pulmonary Embolism (PE):
- Incidence: DVT 10-40% (clinical), PE 1-3%.
- Description: Thromboembolic events due to immobilization and trauma.
- Management: Prophylactic anticoagulation (low molecular weight heparin or oral anticoagulants) is standard. Early mobilization is encouraged.
-
Loss of Reduction/Fixation Failure:
- Incidence: Varies with fracture type and fixation quality.
- Description: Re-displacement of fragments, hardware pull-out, or breakage.
- Management: Revision surgery with more robust fixation, potentially involving different implant constructs or bone grafting.
Late Complications
-
Post-Traumatic Osteoarthritis (PTOA):
- Incidence: Up to 50-70% long-term, even with anatomical reduction.
- Description: Progressive degeneration of articular cartilage due to initial chondral damage, persistent incongruity, malalignment, or instability.
- Management: Symptomatic management (physiotherapy, NSAIDs, injections). For severe, debilitating PTOA, corrective osteotomy (if malalignment is present) or total knee arthroplasty (TKA) may be necessary, often challenging due to prior trauma and hardware.
-
Nonunion/Malunion:
- Incidence: Nonunion < 5%. Malunion > 10%.
- Description: Nonunion refers to failure of bone healing. Malunion is healing in an unacceptable anatomical position (e.g., varus/valgus deformity, procurvatum/recurvatum).
- Management: Nonunion requires revision surgery with debridement, bone grafting, and stable fixation. Malunion may require corrective osteotomy if symptomatic or functionally limiting.
-
Knee Stiffness/Arthrofibrosis:
- Incidence: Up to 20-30%.
- Description: Restricted range of motion due to scar tissue formation within the joint.
- Management: Aggressive physiotherapy, continuous passive motion (CPM), manipulation under anesthesia, or arthroscopic/open arthrolysis.
-
Chronic Pain:
- Incidence: Significant percentage, often multifactorial.
- Description: Persistent pain due to hardware irritation, nerve injury, residual instability, or PTOA.
- Management: Analgesics, physical therapy, nerve blocks, hardware removal (if symptomatic), psychological support.
-
Meniscal/Ligamentous Instability:
- Incidence: Residual instability if concomitant injuries were not diagnosed or adequately managed.
- Description: Persistent knee instability despite fracture healing.
- Management: Ligamentous reconstruction if severe and symptomatic.
Table of Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence | Salvage Strategy |
|---|---|---|
| Compartment Syndrome | 5-15% | Urgent 4-compartment fasciotomy. |
| Popliteal Artery Injury | 3-10% | Urgent vascular repair (grafting), fracture stabilization. |
| Peroneal Nerve Palsy | 2-15% | Observation, bracing. Possible nerve exploration for complete transection or non-recovery. |
| Deep Infection | 1-5% | Urgent surgical debridement, IV antibiotics, irrigation, possible hardware removal/exchange. |
| Wound Necrosis/Dehiscence | 10-20% | Debridement, negative pressure wound therapy, primary closure, or flap coverage. |
| DVT/Pulmonary Embolism | DVT 10-40% | Anticoagulation (therapeutic). |
| Loss of Reduction/Fixation Failure | Varies (5-15%) | Revision surgery with more robust fixation, bone grafting. |
| Post-Traumatic Osteoarthritis | 50-70% | Conservative management (PT, NSAIDs). Corrective osteotomy, total knee arthroplasty for severe, symptomatic disease. |
| Nonunion | < 5% | Revision surgery with debridement, bone grafting, and stable fixation. |
| Malunion | > 10% | Corrective osteotomy if symptomatic or functionally limiting. |
| Knee Stiffness/Arthrofibrosis | 20-30% | Aggressive physical therapy, manipulation under anesthesia, arthrolysis. |
| Chronic Pain | High | Multimodal pain management, hardware removal (if symptomatic), addressing underlying etiology (e.g., PTOA, nerve injury). |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as surgical fixation in achieving optimal outcomes for tibial plateau fractures. Protocols are typically individualized based on fracture stability, fixation achieved, soft tissue integrity, and surgeon preference. The general principles involve protecting the repair, controlling pain and swelling, restoring range of motion, regaining strength, and gradually progressing weight-bearing.
Phase 1: Protective Phase (Weeks 0-6)
- Goals: Protect fixation, control pain and swelling, initiate gentle range of motion, maintain muscle tone.
- Weight Bearing: Strict non-weight bearing (NWB) on the operative leg. Crutches or a walker are used.
- Immobilization: Often a hinged knee brace locked in extension or a specific range (e.g., 0-30 degrees flexion initially) for ambulation and sleep.
-
Range of Motion (ROM):
- Passive Range of Motion (PROM): Initiated early, often within the first few days post-op. Can be performed with a Continuous Passive Motion (CPM) machine or by a therapist.
- Active-Assistive Range of Motion (AAROM): Progressed as tolerated, avoiding active hamstring and quadriceps contraction against resistance if fracture stability is a concern.
- Flexion Limits: May be restricted (e.g., 0-90 degrees) depending on fracture pattern and fixation stability, especially for posterior condyle or medial condyle fractures.
- Cryotherapy & Compression: Essential for edema control and pain management.
-
Exercises:
- Quadriceps setting, gluteal sets.
- Ankle pumps to prevent DVT.
- Gentle knee flexion/extension exercises within prescribed limits.
- Upper body and core strengthening.
Phase 2: Early Mobilization and Progressive Weight Bearing (Weeks 6-12)
- Goals: Gradual increase in weight bearing, improve full range of motion, initiate strengthening.
-
Weight Bearing:
- Week 6-8: Typically progress to toe-touch weight bearing (TTWB) or 25% partial weight bearing (PWB) with crutches, as per radiographic evidence of early healing and surgeon's assessment.
- Week 8-12: Progress to 50-75% PWB.
- Range of Motion: Increase active and passive ROM towards full flexion and extension. Continue gentle stretching.
-
Exercises:
- Initiate gentle closed kinetic chain exercises (e.g., mini-squats, wall slides) with appropriate weight-bearing limits.
- Progress open kinetic chain exercises (e.g., seated knee extension, hamstring curls) with low resistance.
- Proprioception and balance exercises (e.g., single leg stance on stable surface).
- Stationary cycling with light resistance.
Phase 3: Advanced Strengthening and Functional Return (Weeks 12-24+)
- Goals: Restore full strength, endurance, agility, and return to pre-injury activities.
- Weight Bearing: Progress to full weight bearing (FWB) without assistive devices.
- Range of Motion: Achieve full, pain-free ROM.
-
Exercises:
- Advance strengthening with higher resistance and increased repetitions. Incorporate lunges, step-ups, leg press.
- Progress proprioceptive training (e.g., balance board, unstable surfaces).
- Sport-specific drills for athletes.
- Gradual return to impact activities (e.g., jogging) if appropriate for the patient's goals and bone healing.
- Return to Sport: Typically 6-12 months, depending on sport, patient's recovery, and radiographic evidence of complete healing. A functional test battery may be performed.
Important Considerations
- Communication: Close communication between the surgeon, physical therapist, and patient is essential.
- Individualization: Protocols must be tailored to the individual patient, fracture type, quality of fixation, and presence of associated injuries (e.g., meniscal repair, ligamentous reconstruction may necessitate more protected ROM or weight-bearing).
- Pain Management: Ongoing pain management is crucial to allow participation in therapy.
- Complication Monitoring: Monitor for signs of infection, DVT, or hardware complications.
Summary of Key Literature / Guidelines
The management of tibial plateau fractures has evolved significantly with advancements in imaging, surgical techniques, and implant technology. Current literature provides a foundation for evidence-based decision-making.
Classification Systems
- Schatzker Classification (1974): Remains widely used for its simplicity and clinical utility, correlating fracture patterns with injury mechanisms and often guiding surgical approaches. While criticized for its limited inter-observer reliability and inability to fully capture the complexity of bicondylar fractures, it continues to be a standard reference.
- AO/OTA Classification: Offers a more detailed and reproducible system, categorizing fractures by location (proximal tibia, 4), articular involvement (A=extra-articular, B=partial articular, C=complete articular), and increasing severity. It is favored for research and comprehensive communication among specialists.
- Newer imaging-based classifications (e.g., Luo's three-column concept): Emphasize the posteromedial and posterolateral fragments identified by CT, aiding in surgical planning for complex patterns.
Diagnostic Imaging
- CT Scanning: Widely accepted as indispensable for pre-operative planning. Studies consistently show that CT with 3D reconstruction significantly improves the accuracy of fracture characterization, articular depression, and fragment identification compared to plain radiographs alone, leading to better surgical planning and potentially improved outcomes.
- MRI: Recommended for suspected meniscal or ligamentous injuries, which have a high reported incidence (meniscal tears 40-70%, cruciate ligament tears 10-40%). Pre-operative MRI can inform concurrent soft tissue repair strategies.
Surgical Timing and Soft Tissue Management
- The concept of the "safe window" for surgery, allowing for resolution of soft tissue swelling, is strongly supported in the literature. Studies demonstrate a higher incidence of wound complications (necrosis, infection) when surgery is performed in the acute phase (<3 days) in the presence of severe swelling or fracture blisters, unless compelling indications (e.g., compartment syndrome, open fracture, vascular injury) necessitate urgent intervention.
- Staged Protocol: For severe soft tissue injury, a staged approach involving temporary external fixation followed by delayed ORIF (after 7-14 days) has demonstrated reduced rates of wound complications, particularly in high-energy, bicondylar fractures.
Fixation Principles
- Anatomical Reduction: Maintaining articular congruity (ideally <2 mm step-off) and restoring mechanical axis are primary goals to minimize the risk of PTOA.
- Bone Grafting: The use of bone graft (autograft, allograft, or synthetic substitutes) to support elevated articular segments and fill metaphyseal voids is a common practice to prevent secondary collapse, especially in depressed fractures (Schatzker II, III, V, VI). The choice of graft material is often debated, with autograft historically considered the gold standard, but allograft and synthetics showing comparable outcomes in many series.
- Locking Plate Technology: Periarticular locking plates have become the standard of care, offering enhanced angular stability in osteoporotic bone and comminuted fractures, reducing the risk of screw pull-out. They allow for fixation closer to the joint line and facilitate early motion.
- Dual Plating: For bicondylar fractures (Schatzker V, VI), dual plating (anterolateral and posteromedial) provides superior stability compared to single plating, particularly for robust posteromedial column fixation.
Complications and Outcomes
- Post-Traumatic Osteoarthritis (PTOA): Despite anatomical reduction, PTOA remains the most common long-term complication, occurring in 50-70% of cases. Risk factors include residual articular step-off, persistent malalignment, severe initial chondral damage, and associated meniscal/ligamentous injuries.
- Infection and Wound Complications: Remain significant concerns, especially in open fractures or cases with extensive soft tissue injury. Meticulous surgical technique, appropriate timing, and prophylactic antibiotics are key.
- Functional Outcomes: Most patients achieve good to excellent functional outcomes following surgical management. However, a significant proportion may experience some degree of persistent pain, stiffness, or limitation in high-impact activities. Long-term follow-up studies emphasize the importance of early aggressive rehabilitation to maximize ROM and strength.
Rehabilitation
- Early initiation of range of motion is crucial to prevent stiffness, but must be balanced with fracture stability and protected weight-bearing. Gradual progression of weight-bearing, often initiated at 6-12 weeks post-op, is guided by radiographic signs of healing and fracture stability. Individualized protocols are paramount, reflecting the complexity and variability of these injuries.
In summary, the current literature underscores the necessity of comprehensive pre-operative planning utilizing advanced imaging, meticulous surgical technique focused on anatomical reduction and stable fixation, thoughtful management of the soft tissue envelope, and a structured, individualized post-operative rehabilitation program to optimize functional outcomes and minimize complications in patients with tibial plateau fractures.
You Might Also Like