Floating Knee Injuries: Comprehensive Review of Etiology, Anatomy, and Management
Key Takeaway
A floating knee injury involves severe ipsilateral fractures of the femur and tibia, typically from high-energy trauma. Classified by Fraser, these complex injuries demand meticulous assessment due to inherent instability, extensive soft tissue damage, and high rates of neurovascular compromise. Management is primarily operative, often via damage control orthopedics, to restore alignment and prevent complications.
Introduction & Epidemiology
The "floating knee" injury, first described by McNeur in 1953 and later classified by Fraser in 1970, represents a severe ipsilateral fracture of the femur and tibia. This high-energy trauma pattern often results from significant axial loading or direct impact, commonly seen in motor vehicle collisions, falls from height, and pedestrian versus vehicle accidents. The inherent instability and extensive soft tissue damage associated with these injuries classify them among the most challenging musculoskeletal traumas, demanding meticulous assessment and management.
Epidemiologically, floating knee injuries are relatively rare, accounting for approximately 0.5-2% of all long bone fractures. However, they are associated with a high incidence of polytrauma, with reported rates ranging from 20% to over 50%. Associated injuries can be life-threatening and include head trauma, chest and abdominal injuries, and significant vascular or neurological compromise to the affected limb. Vascular injury to the popliteal artery occurs in 8-15% of cases, while peroneal or tibial nerve palsies are reported in 10-30%. Compartment syndrome, a limb-threatening condition, also has a notable incidence.
Fraser's classification remains the most widely accepted system:
*
Type I:
Both femoral and tibial fractures are extra-articular. This subtype generally has a better prognosis but is less common.
*
Type II:
At least one of the fractures (femoral or tibial) extends into the knee joint (intra-articular). This is the more common and prognostically challenging subtype due to the potential for post-traumatic arthritis and long-term functional deficits.
Schatzker's classification for proximal tibia fractures and the AO/OTA classification system for both femoral and tibial fractures are also critical for comprehensive injury characterization, guiding surgical planning, and predicting outcomes. Early recognition, prompt resuscitation following Advanced Trauma Life Support (ATLS) protocols, meticulous limb assessment, and timely surgical stabilization are paramount to optimize functional outcomes and minimize complications.
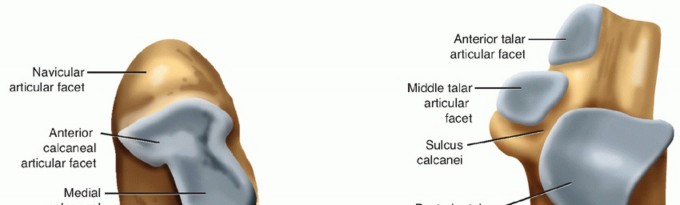
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy of the knee and surrounding femur and tibia is essential for managing floating knee injuries. The knee joint, a complex synovial hinge joint, is formed by the distal femur, proximal tibia, and patella. Its stability is conferred by both bony congruity and a robust ligamentous and muscular envelope.
Femur: The distal femur includes the medial and lateral condyles, the intercondylar notch, and the supracondylar region. The condyles articulate with the tibial plateau. The metaphyseal-diaphyseal junction is a common fracture site.
Tibia: The proximal tibia comprises the medial and lateral tibial plateaus, the intercondylar eminence, and the tibial tuberosity. The tibial plateau is critical for load bearing and knee stability. The tibial shaft extends distally.
Ligamentous Structures:
*
Cruciate Ligaments (ACL & PCL):
Provide primary anteroposterior stability. Often injured in high-energy floating knee cases, particularly if the knee experienced a dislocation component.
*
Collateral Ligaments (MCL & LCL):
Provide valgus and varus stability, respectively. The MCL is a broad, flat ligament, while the LCL is a distinct cord-like structure, part of the posterolateral corner.
*
Patellofemoral Ligaments:
Medial and lateral patellofemoral ligaments contribute to patellar tracking.
Muscles and Neurovascular Structures:
*
Quadriceps Femoris:
Principal extensor of the knee, comprising rectus femoris, vastus medialis, vastus lateralis, and vastus intermedius.
*
Hamstrings:
Semimembranosus, semitendinosus, and biceps femoris. Provide knee flexion and hip extension.
*
Neurovascular Bundle:
The popliteal artery and vein, along with the tibial and common peroneal nerves, pass through the popliteal fossa. These structures are highly vulnerable to injury, particularly in displaced supracondylar femoral or proximal tibial fractures, or knee dislocations. The superficial femoral artery becomes the popliteal artery at the adductor hiatus. The common peroneal nerve courses around the fibular neck.
Biomechanics:
The floating knee disrupts the entire kinetic chain of the lower limb. The femur and tibia, normally acting as stable levers transmitting forces across the knee joint, become unstable segments. This leads to:
*
Loss of load-bearing capacity:
Inability to bear weight.
*
Rotational instability:
Uncontrolled rotation of the limb segments.
*
Muscle dysfunction:
Impaired ability of quadriceps and hamstrings to function effectively.
*
Increased risk of further soft tissue and neurovascular injury:
Due to uncontrolled motion and sharp fracture fragments.
The anatomical considerations guide the surgical approach, internervous planes, and choice of fixation implants. Maintaining the mechanical axis and restoring articular congruity are paramount to long-term function and prevention of post-traumatic arthrosis.
Indications & Contraindications
Management of floating knee injuries is overwhelmingly operative, given the inherent instability, high-energy mechanism, and risk of severe complications. Damage control orthopedics (DCO) principles are frequently applied, especially in polytraumatized patients, where initial external fixation may precede definitive internal fixation.
Operative Indications
The vast majority of floating knee injuries require surgical stabilization. Indications include:
*
All open fractures:
Requiring aggressive debridement, irrigation, and stabilization.
*
Displaced or unstable closed fractures:
To restore alignment and length and prevent further soft tissue damage.
*
Vascular injury:
Requires emergent repair, often followed by skeletal stabilization (either temporary external fixation or definitive internal fixation).
*
Neurological compromise:
While nerve recovery is unpredictable, stabilization prevents further mechanical irritation or stretch.
*
Compartment syndrome:
Requires emergent fasciotomy, with subsequent fracture stabilization.
*
Inability to achieve or maintain closed reduction:
Indicating persistent instability.
*
Polytrauma patients:
Early definitive fixation (within 24-48 hours) can reduce the systemic inflammatory response and improve outcomes in hemodynamically stable patients ("early appropriate care").
*
Fraser Type II injuries:
Intra-articular involvement mandates anatomical reduction and stable internal fixation of the articular fragments.
Non-Operative Indications
Non-operative management for floating knee injuries is exceedingly rare and typically reserved for specific, highly selected cases where surgical risks outweigh potential benefits.
*
Severely comminuted, unsalvageable limb:
In rare instances where amputation is the primary consideration.
*
Extremely high-risk medical comorbidities:
Patients with prohibitive anesthetic or surgical risks where even external fixation is deemed too hazardous.
*
Non-displaced, stable, extra-articular fractures (Fraser Type I):
Only in specific, highly compliant patients, often with an inability to tolerate surgery. This requires strict immobilization and close monitoring, with inherent risks of malunion, nonunion, and stiffness.
Table 1: Operative vs. Non-Operative Indications for Floating Knee
| Feature/Condition | Operative Management | Non-Operative Management |
|---|---|---|
| Fracture Type | All Fraser Type II (intra-articular) | Rarely Fraser Type I (extra-articular, non-displaced) |
| Displaced, unstable fractures (all types) | ||
| Soft Tissue Injury | Open fractures, impending skin compromise, compartment syndrome | Closed, stable soft tissues |
| Vascular/Neurological | All suspected or confirmed vascular injuries | No vascular injury; stable neurological status |
| Progressive neurological deficit | ||
| Patient Status | Hemodynamically stable or stabilized polytrauma | Moribund patient, prohibitive surgical/anesthetic risk |
| Early appropriate care in polytrauma | Unsustainable medical comorbidities | |
| Reducibility/Stability | Unable to achieve or maintain closed reduction | Achievable and maintainable stable closed reduction (rare) |
| Associated Injuries | Knee ligamentous instability (requiring stabilization) | Isolated, non-displaced fibula fracture (if present) |
| Goal | Anatomical reduction, stable fixation, early mobilization | Palliation, comfort, avoiding complications of surgery |
Pre-Operative Planning & Patient Positioning
Comprehensive pre-operative planning is critical for successful management of floating knee injuries, accounting for the often-polytraumatized patient and the complexity of the orthopedic injuries.
Pre-Operative Assessment & Planning
- ATLS Protocol: Prioritize life-threatening injuries. Hemodynamic stability is paramount. Blood products, massive transfusion protocols, and resuscitation adjuncts should be readily available.
-
Detailed Clinical Examination:
- Neurovascular Assessment: Meticulous evaluation of distal pulses (palpation, Doppler), capillary refill, motor and sensory function of the peroneal and tibial nerves. Any suspicion of vascular injury (absent/diminished pulses, expanding hematoma, pulsatile bleeding, pallor, paresthesias, poikilothermia) necessitates emergent vascular surgery consultation and often an angiogram (CT angiography is preferred if stable; conventional angiography if unstable or for therapeutic intervention). Ankle-Brachial Index (ABI) should be performed if pulses are palpable but diminished (ABI < 0.9 is concerning).
- Soft Tissue Envelope: Assess for open wounds, abrasions, contusions, and potential for compartment syndrome. Document swelling and skin viability.
- Knee Stability: While difficult in acute fracture settings, gross instability suggests ligamentous injury.
-
Imaging:
- Plain Radiographs: AP and lateral views of the entire femur, knee, and tibia/fibula, including the hip and ankle joints. Crucially, image quality must be sufficient to define fracture patterns.
- Computed Tomography (CT) Scan: Essential for all intra-articular fractures (Fraser Type II). Provides detailed information on fracture comminution, articular step-off, and fragment displacement. 3D reconstructions are invaluable for pre-operative visualization and surgical templating.
- CT Angiography (CTA): If vascular injury is suspected, a CTA is the gold standard in stable patients.
- MRI: Rarely indicated acutely but may be useful later to assess ligamentous or meniscal injuries.
- Damage Control Orthopedics (DCO): For hemodynamically unstable or severely polytraumatized patients, temporary external fixation (ex-fix) of both the femur and tibia is often the initial orthopedic intervention. This stabilizes the limb, reduces pain, controls bleeding, and allows for resuscitation and management of other life-threatening injuries. Definitive fixation is then performed when the patient is physiologically optimized, typically within 3-10 days.
- Timing of Definitive Fixation: Early appropriate care (definitive fixation within 24-48 hours) is preferred for stable patients to minimize complications like ARDS, fat embolism, and infection, and to facilitate early rehabilitation.
-
Surgical Plan:
- Order of Fixation: Typically, the femur is stabilized first to restore length and alignment, followed by the tibia. This sequence helps restore tension to soft tissues and aids in reduction of the tibial fracture. However, in cases of severe open tibial injury or vascular compromise distal to the tibia, the tibia may be addressed first.
- Implant Choice: Intramedullary nails (IMN) are generally preferred for diaphyseal and some metaphyseal fractures. Locking plates are chosen for articular or highly comminuted metaphyseal fractures where anatomical reduction of the joint surface is paramount. Hybrid fixation (nailing one bone, plating the other) is common.
- Approaches: Determine optimal surgical approaches for both femur and tibia.
Patient Positioning
- Supine Position on a Radiolucent Operating Table: This is the most common position, allowing for easy access to both the femur and tibia, and unimpeded fluoroscopic imaging.
- Traction Table (optional): A traction table can be useful for reducing femoral shaft fractures or achieving length in severe shortening, but can limit access to the knee and distal femur/proximal tibia. Careful consideration is needed, and often manual traction or temporary external fixators are used for reduction.
- Pneumatic Tourniquet: Can be used on the thigh for knee-level work, particularly for definitive plating of intra-articular fractures, to optimize visualization and minimize blood loss. However, prolonged tourniquet time should be avoided, especially if vascular injury is present or suspected.
- Prep and Drape: Extensive prep from the ipsilateral iliac crest to the foot to allow for multiple approaches and potential future incisions. Ensure access to the hip for antegrade femoral nailing and adequate visualization of the entire limb for fluoroscopy.
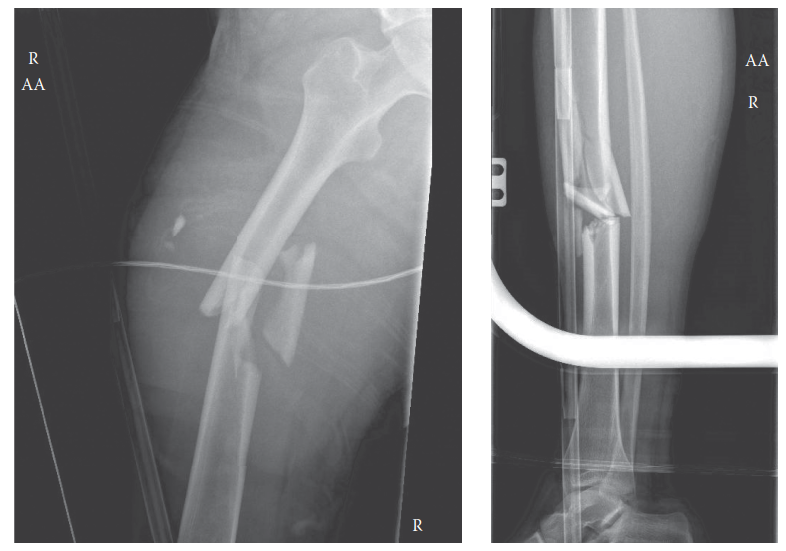
Typical floating knee injury demonstrating displaced distal femoral and proximal tibial fractures.
Detailed Surgical Approach / Technique
The definitive surgical management of a floating knee injury aims to restore anatomical alignment, reconstruct articular surfaces, achieve stable fixation, and facilitate early functional rehabilitation. The approach often combines principles of damage control and early appropriate care.
General Principles
- Sequence: Generally, stabilize the femoral fracture first, then the tibial fracture. This restores overall limb length and mechanical axis, providing a stable platform for subsequent tibial fixation, and often aids in the reduction of the tibial fracture by restoring soft tissue tension. Exceptions include severe open tibial injuries requiring immediate debridement and stabilization, or concomitant vascular injury that must be repaired prior to definitive bone fixation.
- Articular Reconstruction: For intra-articular fractures (Fraser Type II), anatomical reduction of the joint surface is paramount to minimize post-traumatic arthritis. Provisional K-wire fixation should precede definitive screw and plate fixation.
- Soft Tissue Preservation: Minimize additional soft tissue stripping. Utilize minimally invasive techniques where appropriate.
- Stable Fixation: The chosen implants must provide sufficient stability to allow for early, controlled range of motion and progression to weight-bearing.
Femoral Fracture Fixation
Choice of Implant:
*
Intramedullary Nailing (IMN):
The gold standard for diaphyseal and many metaphyseal femoral fractures.
*
Antegrade Nailing:
Entry point typically at the greater trochanter or piriformis fossa. Preferred for midshaft and proximal femur fractures.
*
Retrograde Nailing:
Entry point through the intercondylar notch of the distal femur. Often preferred for distal femoral shaft fractures, supracondylar fractures, or in polytrauma patients where a concomitant ipsilateral hip or acetabular fracture precludes antegrade nailing. Allows for easier approach to the tibia without repositioning.
*
Locking Plate Fixation:
Primarily used for highly comminuted supracondylar/intra-articular distal femoral fractures (e.g., AO/OTA 33-C). Plates (e.g., LISS, LCP) provide angular stability and fixed-angle constructs.
Technique (Example: Retrograde IMN for Distal Femur):
1.
Approach:
Medial or lateral parapatellar approach to the knee, extending proximally as needed. Incise the retinaculum.
2.
Entry Portal:
Identify the intercondylar notch. Create an entry portal just anterior to the PCL origin, slightly medial or lateral to the midline of the intercondylar notch, ensuring alignment with the femoral canal on AP and lateral fluoroscopic views.
3.
Reaming:
Ream the femoral canal to the appropriate size.
4.
Reduction:
Apply longitudinal traction, manual reduction, or temporary external fixation to restore length and alignment. Use reduction clamps or large pointed reduction forceps.
5.
Nail Insertion:
Carefully insert the retrograde femoral nail.
6.
Locking Screws:
Apply distal locking screws first to control rotation and fixation of distal fragments. Then, apply proximal locking screws. Verify appropriate screw length and position with fluoroscopy.
7.
Wound Closure:
Standard layered closure.
Tibial Fracture Fixation
Choice of Implant:
*
Intramedullary Nailing (IMN):
The gold standard for diaphyseal and some metaphyseal tibial fractures.
*
Entry Portal:
Typically a medial or lateral parapatellar approach to create a portal just medial to the patellar tendon insertion, aiming for alignment with the medullary canal. Suprapatellar nailing can also be used, particularly in patients with patella alta or for facilitating easier knee rehabilitation.
*
Locking Plate Fixation:
Preferred for highly comminuted proximal tibial metaphyseal and intra-articular fractures (tibial plateau fractures, e.g., Schatzker V, VI; AO/OTA 41-C).
*
Approaches:
Anteromedial, anterolateral, or posteromedial approaches depending on the fracture pattern and comminution.
*
Dual Plating:
May be required for complex bicondylar plateau fractures.
Technique (Example: Locking Plate for Tibial Plateau Fracture):
1.
Approach:
Anterolateral or anteromedial approach, depending on the plateau involvement. Extensive soft tissue dissection may be required, but care taken to preserve muscle attachments and periosteum.
2.
Articular Reduction:
* Expose the joint directly.
* Use a distraction device (e.g., femoral distractor) or external fixator to gain exposure and aid in reduction.
* Elevate depressed articular fragments using osteotomes or tampers via a cortical window (e.g., through a metaphyseal defect).
* Fill metaphyseal voids with bone graft (autograft, allograft, or synthetic bone substitute) to support the reduced articular surface.
* Provisionally stabilize articular fragments with K-wires, verifying anatomical reduction with fluoroscopy and direct visualization.
3.
Plate Application:
* Contour the locking plate to fit the proximal tibia.
* Apply the plate, ensuring it is positioned to buttress the reduced fragments and provide stable fixation.
* Insert locking screws into the tibial condyles, directed to capture articular fragments and provide subchondral support.
* Insert diaphyseal screws, a mix of locking and non-locking, to secure the plate to the tibial shaft.
4.
Soft Tissue Closure:
Meticulous layered closure, ensuring no undue tension. Consider drains if significant hematoma is anticipated.
Associated Injuries & General Surgical Considerations
- Vascular Repair: If a vascular injury is present, this takes precedence. Vascular repair (e.g., saphenous vein graft) should be performed first, typically followed by temporary external fixation, and then definitive fixation once the vascular repair is secured and patency confirmed.
- Nerve Injuries: Document pre-operative neurological status. Exploration of nerve injuries is not typically performed acutely unless there's a penetrating injury.
- Open Fractures: Require immediate and thorough debridement, pulsed lavage, and appropriate antibiotic prophylaxis. Often, these are initially treated with external fixation, with delayed definitive fixation after several wound checks and further debridements.
- Knee Ligamentous Injuries: While floating knee injuries are often associated with collateral and/or cruciate ligament injuries, primary repair/reconstruction is generally not performed acutely due to the overall severity of the injury, extensive swelling, and risk of infection. These are often addressed in a secondary, staged procedure if symptomatic after fracture healing and rehabilitation.
- Compartment Syndrome: Requires emergent fasciotomy. The fasciotomy wounds are typically left open and managed with serial debridements and delayed primary or secondary closure/skin grafting.
Complications & Management
Floating knee injuries are associated with a high rate of complications due to the severity of the initial trauma, extensive soft tissue disruption, and the complexity of surgical management. Proactive anticipation and meticulous surgical technique are crucial for minimizing their incidence.
Table 2: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (approx.) | Salvage Strategy |
|---|---|---|
| Vascular Injury | 8-15% | Immediate vascular surgery consultation; repair (e.g., vein graft), fasciotomy. External fixation for temporary skeletal stability. |
| Nerve Injury | 10-30% | Observation, neurolysis if entrapped, nerve grafting for gap defects (delayed). Physical therapy. |
| Compartment Syndrome | 5-10% | Emergent fasciotomy (often four-compartment for lower leg). Delayed wound closure/skin graft. |
| Infection (Superficial/Deep) | 5-15% (higher in open fractures) | Aggressive debridement, irrigation, IV antibiotics (culture-guided). Serial debridement. Implant retention if stable; removal if unstable/septic nonunion. |
| Nonunion/Malunion | 10-20% (higher for tibia) | Revision surgery: plate/nail exchange, bone grafting (autograft/allograft), osteotomy for malunion. |
| Post-Traumatic Arthritis | 30-50% (especially Fraser Type II) | Conservative management (NSAIDs, PT, injections). Activity modification. Joint-preserving procedures (osteotomy) or total knee arthroplasty (TKA) in severe cases. |
| Stiffness/Loss of Motion | 20-40% | Aggressive physical therapy, continuous passive motion (CPM). Manipulation under anesthesia. Arthroscopic arthrolysis. |
| Hardware Failure | 5-10% | Revision fixation, often with stronger constructs or exchange nailing. Bone grafting if nonunion present. |
| DVT/Pulmonary Embolism | 5-15% (clinical) | Pharmacological prophylaxis. Early mobilization. Compression devices. Treatment with anticoagulation. |
| Wound Complications | 10-20% | Meticulous wound care, debridement, skin grafting/flap coverage if needed. |
| Heterotopic Ossification | Rare but possible | Prophylaxis (NSAIDs/radiation) in high-risk patients. Excision if symptomatic (delayed). |
Detailed Management Strategies
Early Complications (Acute Phase):
*
Vascular Injury:
Immediate recognition is critical. Angiography (CT or conventional) confirms diagnosis. If identified, immediate skeletal stabilization (often external fixation) to reduce limb movement and facilitate vascular repair by a vascular surgeon. Following repair, close monitoring for compartment syndrome is essential.
*
Nerve Injury:
Most nerve palsies associated with closed fractures are neurapraxias and resolve spontaneously. Serial neurological exams are crucial. If a nerve is transected (e.g., in an open injury), primary repair or grafting may be considered acutely, but often delayed to allow for soft tissue healing.
*
Compartment Syndrome:
High index of suspicion, especially with high-energy trauma, vascular injury, or prolonged ischemia-reperfusion. Classic signs: pain out of proportion, pallor, paresthesia, pulselessness, paralysis. Definitive diagnosis by intracompartmental pressure measurement. Emergent fasciotomy is limb-saving.
*
Infection:
Prophylactic antibiotics are standard. For open fractures, broad-spectrum antibiotics are continued based on Gustilo-Anderson classification. Aggressive debridement of necrotic tissue and thorough wound irrigation are paramount. Deep infections often require surgical debridement, antibiotics, and sometimes implant removal and exchange or external fixation.
Late Complications (Post-Healing Phase):
*
Nonunion/Malunion:
Common, especially in the tibia, due to severe soft tissue damage, comminution, and distraction. Diagnosed by persistent pain, tenderness, motion at the fracture site, and radiographic evidence of failure to heal. Managed by revision surgery: often exchange nailing, plating with bone grafting (autograft or allograft), or osteotomy for malunion to restore alignment.
*
Post-Traumatic Arthritis:
A significant long-term sequela, particularly with intra-articular involvement (Fraser Type II). Results from articular cartilage damage, incongruity, and altered biomechanics. Management ranges from conservative measures (NSAIDs, activity modification, intra-articular injections) to joint-preserving osteotomies for malalignment, and ultimately total knee arthroplasty (TKA) for severe, symptomatic arthritis. TKA in this setting can be technically challenging due to previous hardware, altered anatomy, and soft tissue scarring.
*
Stiffness and Loss of Motion:
High incidence due to prolonged immobilization, soft tissue contractures, and heterotopic ossification. Aggressive physical therapy, including continuous passive motion (CPM) machines, is crucial. Manipulation under anesthesia or arthroscopic/open arthrolysis may be necessary.
*
Hardware Failure:
Breakage or loosening of plates/screws or nails. Usually indicative of an underlying nonunion or excessive mechanical stress. Requires revision surgery to address the nonunion and replace failed hardware.
*
DVT/PE:
Prophylaxis with low-molecular-weight heparin (LMWH) or unfractionated heparin (UFH) is recommended unless contraindicated. Early mobilization is also key.
Close follow-up, patient education, and a multidisciplinary approach involving physical therapists, pain management specialists, and potentially vascular surgeons, are vital for managing these complex complications.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical determinant of functional outcome in floating knee injuries. Protocols must be individualized based on the stability of fixation, the extent of soft tissue injury, and patient compliance. The goals are to restore knee range of motion, muscle strength, and functional mobility while protecting the healing fractures and reconstructed articular surfaces.
General Principles
- Early, Controlled Mobilization: Crucial to prevent stiffness and promote cartilage healing (for intra-articular fractures).
- Gradual Weight-Bearing Progression: Dictated by fracture healing and implant stability.
- Pain Management: Adequate pain control facilitates participation in therapy.
- Patient Education: Understanding the protocol and potential complications is vital for adherence.
Phases of Rehabilitation
Phase 1: Acute Post-Operative (Weeks 0-6)
- Goals: Reduce swelling and pain, protect fixation, initiate gentle range of motion (ROM), maintain muscle tone in uninjured areas.
- Weight Bearing (WB): Typically non-weight bearing (NWB) on the affected limb. Some protocols may allow toe-touch weight bearing (TTWB) if fixation is exceptionally stable, especially for femoral fractures.
-
Range of Motion (ROM):
- Continuous Passive Motion (CPM) machine: Often initiated immediately post-op, aiming for 0-30 degrees initially, progressing gradually to 0-90 degrees as tolerated.
- Passive ROM (PROM): Gentle, pain-free PROM exercises (flexion/extension) by a therapist.
- Active-Assistive ROM (AAROM): Patient assists with movement within pain limits.
-
Exercises:
- Isometric exercises: Quadriceps sets, gluteal sets, hamstring sets to prevent atrophy.
- Ankle pumps: To prevent deep vein thrombosis (DVT).
- Upper body and core strengthening: To maintain overall fitness and aid in transfers.
- Patellar mobilizations: To prevent patellar adhesion and improve tracking.
- Bracing: A hinged knee brace may be used, often locked in extension for protection during transfers and sleep, allowing for controlled ROM during therapy sessions.
Phase 2: Early Healing & Progressive Mobilization (Weeks 6-12)
- Goals: Increase ROM and strength, initiate partial weight bearing, improve gait mechanics.
- Weight Bearing (WB): Progress from TTWB to partial weight bearing (PWB) with crutches or a walker, typically starting around 6-8 weeks post-op, as radiographic signs of healing appear. Gradual progression to full weight bearing (FWB) often occurs by 10-12 weeks, contingent on radiographic confirmation of fracture union.
- Range of Motion (ROM): Progress towards full, pain-free ROM (0-120 degrees flexion).
-
Exercises:
- Isotonic strengthening: Leg raises (straight leg raise, hip abduction/adduction), knee flexion (heel slides), gentle knee extension against gravity.
- Closed kinetic chain exercises (initiation): Partial squats, wall slides (minimal weight), depending on fixation stability.
- Balance and proprioception: Single leg stance (non-involved leg), weight shifting.
- Gait training: With assistive devices, focusing on proper mechanics.
- Bracing: May transition to an unlocked hinged knee brace or discontinue as stability improves and ROM goals are met.
Phase 3: Advanced Strengthening & Functional Recovery (Weeks 12-24)
- Goals: Restore full ROM and strength, achieve independent ambulation, prepare for higher-level activities.
- Weight Bearing (WB): Full weight bearing (FWB) , with cessation of assistive devices as strength and balance allow.
- Range of Motion (ROM): Aim for full, symmetrical ROM.
-
Exercises:
- Progressive resistance exercises: Leg press, hamstring curls, calf raises, step-ups.
- Advanced closed kinetic chain exercises: Deeper squats, lunges, balance board activities.
- Cardiovascular fitness: Stationary cycling, swimming, elliptical trainer.
- Sport-specific drills (if applicable): Initiate low-impact activities, gradually progressing.
- Functional Training: Focus on agility, coordination, and return to daily activities.
Phase 4: Return to Activity / Long-Term (Month 6 onwards)
- Goals: Maximize functional outcomes, address residual deficits, educate on long-term joint health.
- Exercises: Continued strength and endurance training, maintenance of flexibility.
- Activity Modification: Patients with significant articular damage (Fraser Type II) may need to limit high-impact activities to mitigate the risk of premature post-traumatic osteoarthritis.
- Monitoring: Regular follow-up for assessment of joint degeneration and ongoing pain.
- Addressing Secondary Issues: Management of chronic pain, potential need for future ligament reconstruction, or total knee arthroplasty.
It is crucial to emphasize that this is a general guideline. Radiographic evidence of fracture healing is the primary driver for advancing weight-bearing status. Close communication between the orthopedic surgeon and physical therapist is essential throughout the rehabilitation process.
Summary of Key Literature / Guidelines
The management of floating knee injuries has evolved, benefiting from advancements in imaging, surgical techniques, and a better understanding of polytrauma management. Key principles derived from literature and clinical guidelines emphasize a multidisciplinary, systematic approach.
-
Damage Control Orthopedics (DCO): The concept of DCO has been pivotal in managing these often severely injured patients. Early studies by Pape et al. (2000s) and others highlighted the benefits of initial temporary external fixation for unstable polytrauma patients, allowing for physiological resuscitation before definitive internal fixation. This "staged" approach is shown to reduce the systemic inflammatory response and improve outcomes in hemodynamically unstable patients, reducing rates of ARDS, MOF (Multiple Organ Failure), and mortality. However, early appropriate care (definitive fixation within 24-48 hours) for physiologically stable patients has also been shown to improve outcomes by reducing complication rates associated with prolonged external fixation (e.g., pin site infections, loss of reduction).
-
Fracture Fixation Principles:
- Femur: Intramedullary nailing (IMN) is the preferred method for femoral shaft and most metaphyseal fractures due to its load-sharing characteristics, high union rates, and minimally invasive nature. Retrograde IMN is particularly advantageous in floating knee cases as it allows for femoral stabilization without requiring patient repositioning and can be combined with a supracondylar approach for the tibia or used when antegrade nailing is precluded. For complex distal femoral intra-articular fractures (AO/OTA 33-C), anatomical reduction and stable locking plate fixation remain the gold standard.
- Tibia: IMN is also preferred for tibial shaft and some metaphyseal fractures. For proximal tibial plateau fractures (Schatzker V, VI; AO/OTA 41-C), anatomical reduction of the articular surface and buttress plating with locking constructs are essential. Dual plating (medial and lateral) may be necessary for bicondylar fractures. The choice between nailing and plating often depends on the exact fracture morphology (diaphyseal vs. intra-articular) and the extent of soft tissue injury.
- Order of Fixation: Most literature supports stabilizing the femur first to restore limb length and alignment, which aids in subsequent tibial fracture reduction.
-
Associated Injuries Management:
- Vascular Injury: Guidelines universally stress the urgency of identifying and managing popliteal artery injuries. CT angiography is the diagnostic modality of choice in stable patients. Timely repair (within 6-8 hours of ischemia) is critical to prevent amputation. Studies by Friedman et al. and others consistently show that delaying vascular repair significantly increases amputation rates.
- Compartment Syndrome: The necessity for a high index of suspicion and prompt fasciotomy for suspected compartment syndrome is a cornerstone of management, endorsed by trauma and orthopedic societies.
- Ligamentous Injury: Acute repair of knee ligaments is generally not recommended in the setting of complex floating knee fractures due to the extensive swelling, instability, and risk of infection. These are often managed secondarily if persistent instability becomes functionally limiting after fracture healing.
-
Outcomes and Prognosis:
- Functional Outcomes: Despite optimal surgical management, floating knee injuries are associated with significant long-term morbidity. Studies by Fraser (1970), Rethnam et al. (2007), and others consistently report high rates of post-traumatic arthritis (30-50%), knee stiffness (20-40%), malunion/nonunion (10-20%), and chronic pain. Functional scores (e.g., Knee Society Score, SF-36) are often lower compared to isolated long bone fractures.
- Factors Affecting Prognosis: Intra-articular involvement (Fraser Type II), severity of initial soft tissue injury (open fractures, high Gustilo-Anderson classification), associated vascular/nerve injuries, and development of complications (infection, compartment syndrome) are all negative prognostic indicators.
- Rehabilitation: Aggressive and early rehabilitation is consistently highlighted in literature as crucial for optimizing range of motion and functional recovery, even though full recovery is often challenging.
-
Multidisciplinary Approach: The comprehensive management of floating knee injuries, especially in polytrauma, necessitates a multidisciplinary team involving trauma surgeons, orthopedic surgeons, vascular surgeons, anesthesiologists, and physical therapists. This collaborative approach, guided by established ATLS protocols and orthopedic trauma guidelines, remains the gold standard for improving patient outcomes.
In summary, the current literature underscores the severe nature of floating knee injuries. Optimal management involves adherence to DCO principles, meticulous anatomical reduction and stable fixation, vigilant monitoring and aggressive management of associated injuries and complications, and a structured, prolonged rehabilitation program. While functional limitations are common, consistent application of these principles offers the best opportunity for maximizing patient recovery.
You Might Also Like