Beyond the Pitfalls: Effective Patellar Bone Grafting Guide
Key Takeaway
Learn more about Beyond the Pitfalls: Effective Patellar Bone Grafting Guide and how to manage it. Patellar bone grafting addresses severe patellar bone deficiency, occurring in about 10% of revision total knee arthroplasty, when another implant cannot be fixed. It aims to restore bone stock, improve patellar tracking and quadriceps leverage, and offers cosmetic appeal. Correct component positioning is crucial, as malposition with patellar bone grafting can lead to gradual lateral subluxation.
Beyond the Pitfalls: Effective Patellar Bone Grafting Guide
Introduction & Epidemiology
Patellar bone deficiency represents a complex challenge in revision total knee arthroplasty (TKA), often leading to compromised implant fixation, extensor mechanism dysfunction, and persistent anterior knee pain. While a spectrum of patellar issues can arise, severe bone loss that precludes adequate fixation of a new patellar implant is a significant concern. This scenario accounts for approximately 10% of revision TKA cases, demanding a meticulous surgical strategy to restore patellar integrity and function.
The primary objective of patellar bone grafting is to augment compromised patellar bone stock, thereby facilitating secure patellar component fixation, optimizing patellar tracking, improving quadriceps leverage, and achieving a cosmetically acceptable outcome. The choice of grafting technique and material is dictated by the extent and morphology of the bone defect, patient factors, and the overall revision plan. A thorough understanding of the biomechanical implications of patellar bone loss and the reconstructive options is paramount for successful outcomes.
Surgical Anatomy & Biomechanics
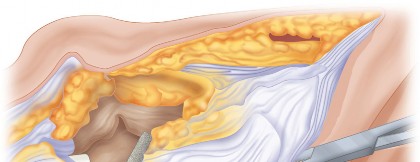
The patella, the largest sesamoid bone, is integral to the extensor mechanism of the knee. Its primary functions include increasing the quadriceps lever arm, enhancing quadriceps efficiency, and protecting the knee joint. Anatomically, the patella comprises a robust cortical shell with a cancellous interior, receiving its blood supply predominantly from the superior and inferior genicular arteries, forming a rich peripatellar anastomosis. Disruption of this blood supply, particularly during extensive surgical exposure or previous procedures, can contribute to bone devitalization and subsequent deficiency.
Biomechanically, effective patellar tracking within the trochlear groove is contingent upon several factors: the morphology and orientation of the femoral trochlea, the tibial tubercle position, overall limb alignment, and critically, the rotational alignment of the femoral and tibial components in a TKA.
Pitfalls in Component Alignment:
*
Correct rotational positioning of the femoral and tibial components is a prerequisite for a successful outcome.
Malrotation of either component can significantly alter patellar kinematics, leading to patellar tilt, subluxation, or impingement.
*
Patellar bone grafting in the setting of component malposition will result in gradual lateral subluxation of the patellar shell construct.
This is a critical pitfall. Grafting may restore bone stock, but it cannot correct fundamental malalignment. Addressing component malrotation and patellofemoral tracking prior to or in conjunction with patellar reconstruction is non-negotiable. Lateral subluxation not only leads to pain and dysfunction but also places abnormal stresses on the graft-implant construct, potentially leading to early failure.
Patellar bone deficiency inherently reduces the contact area with the femoral trochlea and can compromise the quadriceps lever arm. This diminishes the mechanical advantage of the quadriceps, leading to extensor lag, quadriceps weakness, and difficulty with activities requiring knee extension. Grafting aims to restore patellar volume and shape, thereby improving contact mechanics and quadriceps efficiency. Furthermore, an intact patella provides a stable platform for quadriceps and patellar tendon insertions, which are crucial for maintaining the integrity and function of the extensor mechanism.
Indications & Contraindications
Patellar bone grafting is a specialized technique primarily reserved for revision TKA in the presence of significant patellar bone loss.
Indications for Patellar Bone Grafting:
-
Severe Patellar Bone Deficiency:
This is the primary indication, where insufficient host bone precludes stable fixation of a conventional patellar component. This typically correlates with Work-Leiden (W-L) classification types III and IV, or Sisto-Meller (S-M) classification types III and IV.
- Type III (W-L/S-M): Patellar component loosening with significant bone loss confined to the patella.
- Type IV (W-L/S-M): Patellar component loosening with extensive bone loss and compromised extensor mechanism.
- Cancellous patellar bone grafting provides potential for restoration of bone stock, facilitates patellar tracking, improves quadriceps leverage, and is cosmetically appealing.
- Periprosthetic Patellar Fracture: Non-union or malunion of patellar fractures in the presence of an existing TKA component, especially if associated with bone loss that would compromise subsequent component fixation.
- Aseptic Loosening with Osteolysis: Significant bone resorption around a loose patellar component, necessitating bone stock restoration prior to reimplantation.
- Recurrent Patellar Instability with Bone Loss: While component malposition is the primary etiology, persistent instability in the setting of structural bone deficiency may benefit from grafting to restore patellar height or thickness.
- Salvage of Extensor Mechanism Compromise: In select cases, to reconstruct a severely compromised patella that is part of a larger extensor mechanism reconstruction.
Contraindications:
- Active Periprosthetic Joint Infection: Grafting in the presence of active infection is contraindicated due to high failure rates and risk of chronic infection. The infection must be eradicated prior to any reconstructive procedure.
- Insufficient Soft Tissue Coverage: Inadequate skin and subcutaneous tissue coverage over the anterior aspect of the knee may compromise wound healing and graft viability.
- Irreparable Extensor Mechanism Disruption: If the quadriceps or patellar tendon is extensively damaged or irrecoverably scarred, the underlying mechanical stability required for graft integration may be absent.
- Severe Uncorrectable Malalignment: If underlying femoral or tibial component malrotation or overall limb alignment issues cannot be corrected, grafting alone will not resolve patellofemoral dysfunction and may fail.
- Limited Patient Compliance/Poor Medical Status: Patients with severe comorbidities or those unable to comply with rigorous rehabilitation protocols may not be suitable candidates.
- Extensive Patellar Necrosis: If the entire patella is avascular and necrotic, grafting may be futile, and alternative salvage procedures should be considered.
Summary of Patellar Problem Management Options
| Category | Indication for Grafting | Other Operative Options for Patellar Problems (No Grafting) | Non-Operative Management (for Minor Issues/Adjunctive) |
|---|---|---|---|
| Bone Loss | Severe patellar bone deficiency precluding component fixation (W-L III/IV, S-M III/IV), osteolysis, recurrent loosening with bone deficit. | Structural bone grafting of the patella (onlay/inlay), Cancellous Patellar Bone Grafting . | |
| Patellar Component Failure (No Severe Bone Loss) | N/A | Patellar component exchange (if bone stock is adequate). | |
| Tracking/Alignment Issues | Patellar height/thickness restoration needed for improved tracking in specific bone loss scenarios. | Revision of malrotated femoral/tibial components, lateral retinacular release, medial patellofemoral ligament reconstruction (rarely primary). | Physical therapy, quadriceps strengthening, bracing (rarely effective for fixed malalignment). |
| Fracture | Non-union or malunion with significant bone loss. | Open reduction internal fixation (ORIF) for acute fractures with sufficient bone stock. | Immobilization, conservative management for stable, non-displaced fractures. |
| Extensor Mechanism Compromise | Reconstruction in conjunction with soft tissue repair. | Quadriceps plasty, V-Y lengthening, allograft reconstruction of tendons. | Physical therapy, bracing. |
| Salvage Options | To avoid patellectomy. | Patellar resection arthroplasty (rarely indicated for severe bone loss), Gull-wing osteotomy (for patellar fracture/defect), Porous metal baseplate , Crossed Kirschner wires for cemented fixation of the patellar component . Patellectomy should be avoided. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial for successful patellar bone grafting. This involves a comprehensive patient assessment, detailed imaging review, and surgical templating.
1. Examination/Imaging:
*
Clinical Examination:
*
Skin:
Assessment of location, quality, and vascularity of previous incisions. Note any atrophy, scarring, or signs of impending dehiscence. Integrity of the extensor mechanism should be evaluated for palpable defects, tendon integrity, and quadriceps function.
*
Range of Motion (ROM):
Document active and passive ROM, looking for contractures or extensor lag.
*
Patellar Tracking:
Dynamic assessment of patellar motion through flexion and extension, noting any subluxation or tilt.
*
Neurovascular Status:
Pre-operative assessment is essential.
*
Imaging:
*
Standard Radiographs:
AP, lateral, and Merchant views of the knee are essential. Assess patellar height, tilt, subluxation, and overall bone loss. Look for osteolysis around existing components.
*
Long-Leg Alignment Views:
To assess overall limb alignment and identify any coronal plane deformities.
*
Computed Tomography (CT) Scan:
The gold standard for evaluating patellar bone stock and morphology, quantifying bone loss, and precisely assessing femoral and tibial component rotation. This is critical for identifying and planning correction of underlying malalignment that could jeopardize graft success.
*
Magnetic Resonance Imaging (MRI):
Useful for evaluating soft tissue integrity (quadriceps/patellar tendons) if clinical suspicion for rupture exists.

2. Graft Selection & Templating:
*
Graft Type:
*
Autograft:
Offers osteoinductive and osteoconductive properties, no risk of disease transmission. Potential donor sites include the ipsilateral femoral head, proximal tibia (condyle), or distal femur. Disadvantages include limited availability and donor site morbidity.
*
Allograft:
Readily available, avoids donor site morbidity. Typically, femoral head or distal femoral condyle allografts are used. Disadvantages include risk of disease transmission (though low with modern processing) and slower incorporation compared to autograft. Allograft morselized cancellous bone is often used to fill cavities.
*
Combined Autograft/Allograft:
Frequently employed, using structural allograft for large defects and autograft (e.g., from reamed medullary canals or osteophytes) for cancellous packing.
*
Templating:
Utilize pre-operative imaging (especially CT) to template the required graft size and shape. Consider the ideal patellar thickness and height for optimal tracking.
3. Patient Positioning:
*
Supine Position:
Standard for TKA.
*
Tourniquet:
A pneumatic tourniquet on the proximal thigh is typically used to minimize blood loss and enhance visualization.
*
Donor Site Access:
If autograft harvest (e.g., ipsilateral femoral head) is planned, ensure appropriate draping and positioning to allow for aseptic access to the hip joint.

Detailed Surgical Approach / Technique
The surgical technique for patellar bone grafting is highly individualized based on the extent of bone loss and the specific goals of the revision. The following outlines a generalized approach, focusing on key principles.
1. Incision and Exposure:
* Utilize the existing midline skin incision if feasible. If a new incision is required, aim for a straight midline approach.
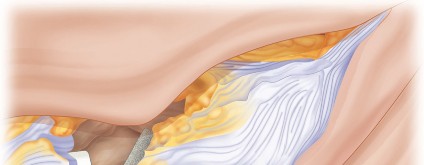
* Carefully dissect through scarred subcutaneous tissue. A medial parapatellar arthrotomy is commonly used, extending proximally along the quadriceps tendon and distally to the tibial tubercle. Meticulous soft tissue handling is crucial to preserve remaining vascularity and avoid devitalizing the patella.
* Address any adhesions and achieve adequate exposure of the patellofemoral joint. Evert the patella if possible, or perform a quadriceps snip or V-Y quadriceps arthroplasty if necessary for exposure.

2. Component Assessment and Removal:
* Thoroughly assess the existing femoral, tibial, and patellar components for loosening, malposition, wear, and corrosion.
*
Crucially, assess femoral and tibial component rotation.
If malrotation is identified as a primary driver of patellar dysfunction, this must be addressed. Correcting component malposition is often a prerequisite for successful patellar grafting outcomes.
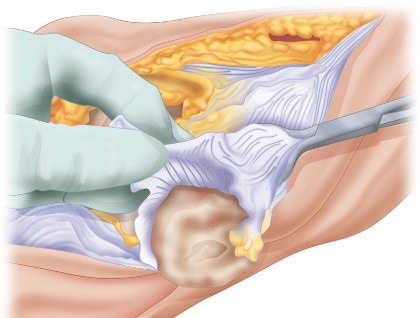
* Carefully remove the failed patellar component and any associated cement or osteolytic debris.

3. Patellar Preparation:
* Debride all fibrous tissue, necrotic bone, and sclerotic margins from the patellar defect. The goal is to create a well-vascularized, bleeding bone bed to promote graft integration.
* Measure the dimensions of the patellar defect (depth, width, height) to guide graft sizing.
* Maintain as much of the intact cortical shell as possible, especially the superior and inferior poles for quadriceps and patellar tendon insertions.
4. Graft Harvest and Shaping (if applicable):
*
Autograft:
If using ipsilateral femoral head autograft, harvest is performed at this stage. The femoral head can be fashioned into a desired shape using oscillating saws and rongeurs.
*
Allograft:
Thaw and prepare the allograft (e.g., femoral head, distal femur) according to tissue bank protocols. Shape the allograft precisely to match the patellar defect, ensuring a stable press-fit or a suitable surface for fixation.

5. Graft Fixation:
*
Cancellous Patellar Bone Grafting:
For smaller defects or to fill voids behind a structural graft or implant. The cancellous bone is packed firmly into the defect to maximize contact with host bone. This provides an osteoconductive scaffold.
*
Structural Bone Grafting:
*
Inlay Grafting:
A defect-specific graft is fashioned and placed into a prepared cavity in the patella.
*
Onlay Grafting:
The graft is contoured to augment the posterior surface of the patella.
*
Fixation Methods:
*
Screws:
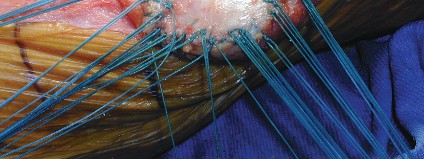
Small fragment screws (e.g., 2.7 mm or 3.5 mm cortical screws) or cannulated screws are often used for rigid fixation of structural grafts. These are typically placed from the anterior cortical surface into the graft, avoiding penetration of the articulating surface.
*
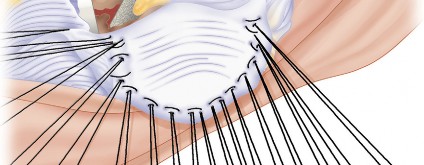
Kirschner Wires:
As mentioned in the seed,
crossed Kirschner wires for cemented fixation of the patellar component
can be employed. These provide initial stability for the graft and act as anchors for cement interdigitation. The wires are cut flush or bent to prevent irritation.
*
Cerclage Wires:
Circumferential cerclage wires can be used, particularly in cases where the cortical shell is fractured or compromised, to provide additional stability to the entire patellar construct.


*
Porous Metal Baseplate:
In some systems, a porous metal baseplate can be used directly as a structural augmentation to bridge defects or provide a platform for component fixation.

6. Patellar Component Implantation:
* Once the graft is securely fixed and deemed stable, the patella is prepared for the new patellar component.
* If using a standard cemented component, drill peg holes into the graft and host bone, ensuring proper depth.
* Cleanse the surface thoroughly.
* Cement the new patellar component, ensuring complete cement mantle and stable fixation to both the graft and remaining host bone.


7. Addressing Patellar Tracking and Extensor Mechanism Integrity:
* With the new patellar component in place, meticulously assess patellar tracking throughout the range of motion.
* If lateral maltracking persists, a lateral retinacular release may be indicated. However, this should be performed judiciously to avoid devascularization or over-release, which could lead to medial instability.
* Ensure the overall tension of the extensor mechanism is appropriate.
* The seed mentions
Gull-wing osteotomy
as a treatment option. This technique, typically used for managing patellar fractures with significant bone loss or defects, involves creating two osteotomy cuts to elevate the patellar fragments, often combined with a structural graft or porous metal augments, to restore patellar morphology.



8. Alternative Considerations:
*
Patellar Resection Arthroplasty:
This involves removing the patella and allowing a fibrous articulation. While listed as an option, it is generally considered a salvage procedure for patients with severely compromised patellae where reconstruction is not feasible, often leading to poor functional outcomes, extensor lag, and anterior knee pain.
*
Patellectomy:
As strongly indicated in the seed content,
patellectomy should be avoided.
It leads to a significant loss of quadriceps mechanical advantage, marked extensor lag, and severe functional impairment. It is a procedure of last resort.

9. Wound Closure:
* Thorough irrigation of the surgical site.
* Careful layered closure of the arthrotomy and subcutaneous tissues, ensuring no tension on the skin. A drain may be used.
* Assess stability of the entire construct and patellar tracking one final time before wound closure.
Complications & Management
Patellar bone grafting is a technically demanding procedure associated with a range of potential complications, some unique to the graft itself and others inherent to revision TKA.
| Complication | Incidence (Approximate) | Salvage Strategies
Post-Operative Rehabilitation Protocols
Successful outcomes following patellar bone grafting hinge not only on meticulous surgical execution but also on a structured and progressive post-operative rehabilitation protocol. The goal is to protect the healing graft, ensure secure fixation of the patellar component, restore range of motion, and optimize quadriceps function, all while respecting the biological timeline for graft incorporation.
Phase 1: Initial Protection and Early Motion (Weeks 0-6)
The primary goals are to protect the graft-implant construct and initiate controlled range of motion.
*
Immobilization:
The knee is typically placed in an immobilizer or hinged knee brace locked in extension for the initial 2-4 weeks. This provides protection against disruptive forces, particularly during weight-bearing.
*
Weight-Bearing:
Touch-down weight-bearing (TDWB) or non-weight-bearing (NWB) with crutches is usually prescribed for the first 4-6 weeks to minimize stress across the healing patella.
*
Range of Motion (ROM):
*
Passive ROM:
Gentle passive flexion, often initiated in a controlled manner (e.g., using a continuous passive motion, CPM, machine or assisted by a therapist), up to 30-45 degrees by Week 2, progressing to 60-90 degrees by Week 6, depending on surgical stability. Extension should be stressed toward full extension.
*
Active-Assisted ROM:
Once passive motion is tolerated, active-assisted exercises can begin.
*
Muscle Activation:
*
Quadriceps Sets:
Gentle isometric quadriceps contractions in extension to promote muscle activation without stressing the patellofemoral joint.
*
Ankle Pumps:
To prevent deep vein thrombosis.
*
Gluteal Sets:
To maintain hip strength.
*
Wound Care:
Meticulous wound care is essential.
Phase 2: Progressive Motion and Strengthening (Weeks 6-12)
This phase focuses on increasing ROM, restoring quadriceps strength, and initiating protected weight-bearing.
*
Weight-Bearing:
Progress from TDWB to partial weight-bearing (PWB), and then to full weight-bearing (FWB) as tolerated and as radiographic evidence of graft healing progresses. A gradual increase in knee flexion during weight-bearing activities is introduced.
*
Range of Motion (ROM):
* Progressive increase in active and passive flexion towards full range. Target 120-130 degrees by the end of this phase.
* Continue to work on achieving full extension.
*
Strengthening:
*
Isometrics:
Continued quadriceps sets, hamstring sets.
*
Light Concentric/Eccentric:
Gradually introduce gentle short arc quads (SAQ), straight leg raises (SLR) with minimal resistance, hamstring curls, and calf raises. Avoid resisted terminal knee extension (0-30 degrees) to minimize patellofemoral joint stress initially.
*
Core Strengthening:
Crucial for overall stability.
*
Proprioception:
Begin balance exercises (e.g., single leg stance with support).
*
Scar Mobilization:
Gentle massage to prevent adhesions.
Phase 3: Advanced Strengthening and Functional Return (Weeks 12-24)
The focus shifts to advanced strengthening, improving endurance, and preparing for return to functional activities.
*
Full Weight-Bearing:
Expected to be at FWB without assistive devices.
*
Range of Motion (ROM):
Should be approaching near-normal or functional limits.
*
Strengthening:
* Progressive resistance exercises for quadriceps, hamstrings, and glutes. This includes leg presses, squats (mini-squats initially, progressing in depth), step-ups, and lunges.
* Emphasize eccentric control of the quadriceps.
* Begin closed-chain exercises to promote co-contraction and stability.
*
Cardiovascular Fitness:
Introduce low-impact activities such as stationary cycling, elliptical training, or swimming.
*
Sport-Specific Training (if applicable):
For patients desiring return to more demanding activities, introduce agility and higher-level proprioceptive drills under strict supervision.
*
Criteria for Progression:
Based on pain levels, absence of swelling, adequate strength symmetry, and objective ROM achievements.
Phase 4: Return to Activity (Months 6+ and beyond)
*
Maintenance:
Continue with a home exercise program focused on strength, flexibility, and endurance.
*
Gradual Return to Activity:
Patients can progressively return to desired activities, guided by their surgeon and therapist, ensuring that activities are introduced gradually to prevent overload. High-impact or pivoting sports may be restricted or modified based on individual outcomes and long-term stability of the construct.
Key Considerations:
*
Pain Management:
Effective pain control is vital to facilitate participation in rehabilitation.
*
Edema Control:
Compression and elevation are important to manage swelling.
*
Patient Education:
Patients must understand the importance of adherence to protocols and the biological timeline for graft healing, which can be 6-12 months or longer for full incorporation.
*
Radiographic Monitoring:
Serial radiographs are essential to monitor graft integration and component stability.
Summary of Key Literature / Guidelines
The body of literature concerning patellar bone grafting in revision TKA is primarily composed of case series, retrospective reviews, and smaller prospective studies, reflecting the relatively uncommon but challenging nature of the procedure. There are no large-scale randomized controlled trials, and thus, current guidelines often draw from expert consensus and cumulative clinical experience.
Key themes in the literature emphasize:
- Importance of Addressing Underlying Biomechanics: Numerous studies reiterate that patellar tracking issues and mechanical malalignment (particularly femoral and tibial component malrotation) must be corrected to ensure the longevity of any patellar reconstruction, including grafting. Failure to do so is a primary cause of recurrent patellar subluxation and graft failure, as highlighted by the seed content.
- Efficacy of Autograft vs. Allograft: While autograft theoretically offers superior osteoinductive properties and faster incorporation, allograft (especially femoral head) has demonstrated comparable clinical outcomes for structural defects, often preferred for its availability and avoidance of donor site morbidity. The use of cancellous allograft for void filling is also well-supported.
- Fixation Methods: Rigid fixation of structural grafts using screws, Kirschner wires, and/or cerclage wires is critical for initial stability and preventing micromotion that could impede graft incorporation. Cemented fixation of the patellar component onto the reconstructed patella requires careful technique to ensure robust interdigitation with both host bone and graft.
- Clinical Outcomes: Outcomes are generally favorable in selected patients, with reports of improved patellofemoral tracking, reduced anterior knee pain, and restoration of quadriceps function. However, complication rates, particularly patellar fracture and aseptic loosening, remain higher than in primary TKA or routine patellar component revision.
- Classification Systems: The Work-Leiden (W-L) and Sisto-Meller (S-M) classification systems for patellar bone defects are widely used to guide treatment decisions and prognosticate outcomes. These systems help standardize the assessment of patellar bone loss, which is fundamental to determining the need for grafting.
- Role of Alternative Techniques: While patellectomy should be avoided due to poor functional outcomes, techniques like Gull-wing osteotomy are recognized for specific patellar fracture patterns with bone loss, allowing for better restoration of patellar height and morphology. Porous metal baseplates offer an alternative in complex defects, aiming for biological fixation.
- Rehabilitation: A structured, progressive rehabilitation program is paramount, balancing early motion with protection of the healing construct. Excessive early loading or aggressive ROM can compromise graft healing and fixation.
Overall, the literature supports patellar bone grafting as a viable and often necessary option for severe patellar bone deficiency in revision TKA, provided that underlying biomechanical issues are adequately addressed and meticulous surgical technique is employed. Continued research, particularly on long-term outcomes and advanced grafting materials, will further refine treatment algorithms.
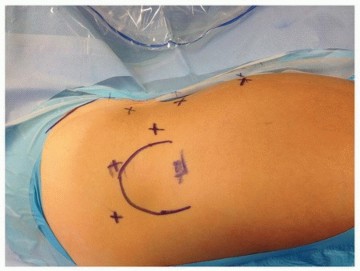
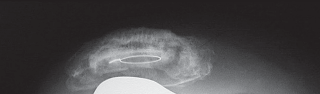
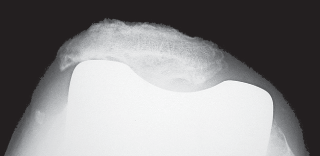
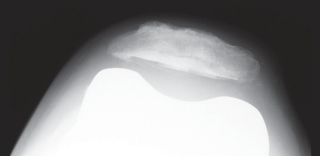
Clinical & Radiographic Imaging


You Might Also Like