Find Top Knee Arthroscopy Surgeons in San Jose for Expert Care

Key Takeaway
We review everything you need to understand about Find Top Knee Arthroscopy Surgeons in San Jose for Expert Care. Finding top knee arthroscopy surgeons in San Jose, CA involves thorough research, checking online reviews on sites like Healthgrades or Zocdoc, and seeking referrals. Evaluate their experience, credentials, communication style, and patient satisfaction to ensure quality care. Prioritize surgeons in San Jose with proven expertise for effective treatment.
Introduction & Epidemiology
Knee arthroscopy represents a cornerstone procedure in contemporary orthopedic surgery, characterized by its minimally invasive nature for both diagnostic and therapeutic interventions within the tibiofemoral and patellofemoral joints. The genesis of arthroscopy is credited to Professor Kenji Takagi in the early 20th century, who utilized a cystoscope to inspect the knee joint, with further pioneering work by Dr. Masaki Watanabe advancing instrumentation and technique in the mid-20th century. This evolution from open arthrotomy to endoscopic visualization has revolutionized the management of intra-articular knee pathology, offering substantial advantages including smaller incisions, reduced post-operative pain, accelerated rehabilitation, and enhanced intra-articular assessment and precision.
Epidemiologically, knee arthroscopy remains one of the most frequently performed orthopedic surgical procedures globally. Its widespread application spans a broad demographic, from young athletes sustaining acute traumatic injuries to older individuals presenting with degenerative conditions. Common indications contributing to its high incidence include meniscal tears (both traumatic and degenerative), anterior cruciate ligament (ACL) ruptures, chondral defects, loose body removal, and treatment of synovial disorders. The increasing participation in sports and recreational activities across all age groups, coupled with an aging population seeking to maintain active lifestyles, continues to drive the demand for arthroscopic knee procedures. Advances in imaging modalities, particularly magnetic resonance imaging (MRI), have also refined diagnostic accuracy, leading to more targeted surgical interventions. A robust understanding of the indications, contraindications, anatomical nuances, technical strategies, and potential sequelae is imperative for any practitioner involved in the care of knee joint pathologies.
Surgical Anatomy & Biomechanics
A profound understanding of knee anatomy and biomechanics is fundamental for successful arthroscopic intervention. The knee joint, the largest synovial joint in the human body, is a complex articulation comprising the tibiofemoral and patellofemoral joints.
Bony Architecture and Articular Surfaces
The distal femur presents with medial and lateral condyles, separated by the intercondylar notch. The proximal tibia features medial and lateral tibial plateaus, which are relatively flat but possess slight concavities, separated by the intercondylar eminence. The patella, a sesamoid bone, articulates with the trochlear groove on the anterior aspect of the distal femur. All articulating surfaces are covered by hyaline cartilage, a specialized connective tissue critical for smooth, low-friction movement and efficient load distribution. Cartilage thickness varies across the joint, being thickest on the patella and femoral condyles. Damage to this cartilage, particularly full-thickness defects, can significantly impair joint function and predispose to osteoarthritis.
Menisci
The menisci are crescent-shaped fibrocartilaginous structures interposed between the femoral condyles and tibial plateaus.
*
Medial Meniscus:
C-shaped, broader posteriorly, with firm attachments to the deep medial collateral ligament (MCL) and joint capsule. This relative immobility renders it more susceptible to injury.
*
Lateral Meniscus:
More circular or O-shaped, with less firm peripheral attachments (apart from the popliteus hiatus), allowing for greater mobility.
*
Functions:
Menisci play crucial roles in load transmission (reducing tibiofemoral contact stresses by 50% or more), shock absorption, joint stability (especially the medial meniscus limiting anterior tibial translation), and proprioception.
*
Vascularity:
The blood supply to the menisci originates from the medial and lateral geniculate arteries, forming a perimeniscal capillary plexus. This supply penetrates approximately 10-30% of the meniscal width from the periphery, defining the "red-red" (vascularized), "red-white" (partially vascularized), and "white-white" (avascular) zones. This vascularity directly influences healing potential, with repairs being more successful in the red-red zones.
Ligamentous Stabilizers
The knee's stability is largely dependent on a complex interplay of intra-articular and extra-articular ligaments.
*
Cruciate Ligaments (Intra-articular):
*
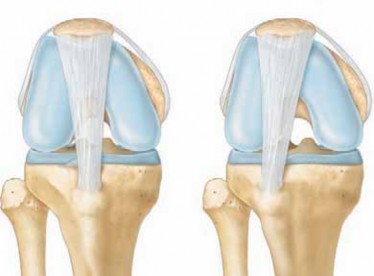
Anterior Cruciate Ligament (ACL):
Originates from the posterior-medial aspect of the lateral femoral condyle and inserts into the anteromedial intercondylar area of the tibia. It is the primary restraint to anterior tibial translation and a secondary restraint to internal rotation. It consists of two main bundles: the anteromedial (AM) bundle (tighter in flexion) and the posterolateral (PL) bundle (tighter in extension), which function synergistically throughout the range of motion.
*
Posterior Cruciate Ligament (PCL):
Originates from the anterior-lateral aspect of the medial femoral condyle and inserts onto the posterior aspect of the tibial plateau. It is the primary restraint to posterior tibial translation. It also comprises two bundles: the anterolateral bundle (tighter in flexion) and the posteromedial bundle (tighter in extension).
*
Collateral Ligaments (Extra-articular):
*
Medial Collateral Ligament (MCL):
Composed of superficial and deep layers. The superficial MCL originates from the medial femoral epicondyle and inserts onto the medial tibia (approximately 5 cm distal to the joint line). The deep MCL is a thickening of the joint capsule. The MCL is the primary static restraint to valgus stress.
*
Lateral Collateral Ligament (LCL):
A cord-like structure originating from the lateral femoral epicondyle and inserting into the fibular head. It is the primary static restraint to varus stress.
*
Posterolateral Corner (PLC):
A complex of structures including the LCL, popliteus tendon, popliteofibular ligament, and posterior capsule. It is critical for resisting varus and external rotational stresses. Injuries here often lead to significant instability and require careful assessment.
Synovium and Plicae
The synovial membrane lines the non-articular surfaces of the joint, producing synovial fluid for lubrication and nutrition of avascular cartilage. Synovial inflammation (synovitis) can be a source of pain and effusion. Plicae are normal synovial folds that, in some individuals, can become thickened, inflamed, and symptomatic (e.g., medial patellar plica syndrome), requiring arthroscopic excision.
Neurovascular Structures
Awareness of adjacent neurovascular structures is paramount during portal placement and instrument manipulation.
*
Saphenous Nerve and Artery:
Located medially, close to the anteromedial portal.
*
Common Peroneal Nerve:
Courses around the fibular neck, susceptible to injury with lateral portals or extensive dissection in the posterolateral aspect.
*
Popliteal Artery and Vein:
Posterior to the knee joint, especially vulnerable during posterior portal placement or deep posterior compartment procedures.
Biomechanics
The knee joint exhibits complex kinematics, including rolling and gliding motions, coupled with axial rotation, particularly during flexion and extension. The "screw-home mechanism" describes the obligatory external rotation of the tibia on the femur during the final degrees of extension, locking the knee. Menisci facilitate these movements and enhance joint congruity. Ligamentous tension varies throughout the range of motion, ensuring stability. Pathological conditions, such as meniscal tears or ligamentous ruptures, disrupt these normal biomechanical relationships, leading to altered load distribution, instability, pain, and accelerated degenerative changes.
Indications & Contraindications
The decision for arthroscopic intervention necessitates a thorough clinical evaluation, imaging assessment, and consideration of patient-specific factors.
General Indications (Diagnostic and Therapeutic)
- Persistent Knee Pain: Unresponsive to conservative management, especially when associated with mechanical symptoms.
- Mechanical Symptoms: Locking, catching, or giving way, often suggestive of meniscal tears, loose bodies, or patellar instability.
- Acute Knee Trauma: For diagnosis and treatment of internal derangements (e.g., ACL rupture, meniscal tears).
- Chronic Synovitis: For diagnostic biopsy or therapeutic synovectomy in conditions like pigmented villonodular synovitis (PVNS) or rheumatoid arthritis.
- Inconclusive Imaging: When physical examination and non-invasive imaging (MRI) do not fully explain symptoms, diagnostic arthroscopy can be warranted.
Specific Operative Indications
-
Meniscal Pathology:
- Meniscal Tears: Unstable tears causing mechanical symptoms (locking, catching), tears in vascularized zones amenable to repair, complex tears causing instability.
- Cystic Lesions: Meniscal cysts not responsive to aspiration.
-
Ligamentous Instability:
- ACL Reconstruction: Symptomatic instability after ACL rupture, particularly in active individuals.
- PCL Reconstruction: Less common, typically for high-grade PCL injuries causing significant instability.
- MCL/LCL Repair/Reconstruction: In conjunction with other ligamentous injuries, though often managed non-operatively.
-
Chondral and Osteochondral Lesions:
- Chondroplasty: Debridement of unstable chondral flaps.
- Microfracture: For small, contained full-thickness chondral defects.
- Osteochondral Autograft Transfer System (OATS) / Allograft Transplantation: For larger osteochondral defects.
- Autologous Chondrocyte Implantation (ACI) / Matrix-Associated Autologous Chondrocyte Implantation (MACI): For large, symptomatic chondral defects.
- Loose Bodies: Symptomatic intra-articular fragments causing mechanical symptoms.
-
Synovial Pathology:
- Synovectomy: For chronic inflammatory synovitis (e.g., PVNS, synovial chondromatosis, rheumatoid arthritis) unresponsive to medical management.
- Plica Excision: For symptomatic medial patellar plica syndrome.
-
Patellofemoral Disorders:
- Lateral Retinacular Release: For recalcitrant lateral patellar compression syndrome or maltracking.
- Medial Patellofemoral Ligament (MPFL) Reconstruction: For recurrent patellar instability.
- Infection: Septic arthritis requiring joint lavage and debridement.
- Fracture Management: Arthroscopic-assisted reduction and internal fixation of tibial plateau fractures or intercondylar eminence avulsion fractures.
- Biopsy: For suspicious intra-articular lesions.
Contraindications
-
Absolute Contraindications:
- Active Local Infection (unless the procedure is for septic arthritis): Introduction of instruments into an already infected field or through an infected skin lesion can disseminate infection.
- Severe Uncontrolled Systemic Illness: Significant cardiovascular, pulmonary, or metabolic disease that contraindicates general or regional anesthesia.
-
Relative Contraindications:
- Severe Osteoarthritis: While arthroscopy may offer temporary relief for mechanical symptoms (e.g., meniscal tears) in early osteoarthritis, it is generally not indicated for global osteoarthritic pain without specific mechanical causes. Outcomes are often poor in advanced disease, where arthroplasty is more appropriate.
- Severe Soft Tissue Compromise: Extensive skin lesions, cellulitis, or open wounds around the knee.
- Ankylosis: Inability to achieve adequate joint distension or instrument manipulation.
- Uncorrectable Coagulopathy: Increased risk of intra-articular hemorrhage.
- Morbid Obesity: Technically challenging due to deep surgical field, but not an absolute contraindication.
- Non-Cooperative Patient: Inability to comply with post-operative rehabilitation protocols.
Table: Operative vs. Non-Operative Indications for Common Knee Pathologies
| Indication Category | Operative Management (Arthroscopic) | Non-Operative Management |
|
Ligamentous Injuries
|
ACL Rupture with Instability
: Isolated ACL tear with functional instability, or concomitant with meniscal tears.
PCL Rupture with Instability
: High-grade tears causing symptomatic instability.
Multi-ligamentous Knee Injuries
: Complex injuries involving multiple ligaments requiring staged or simultaneous reconstruction. |
|
Chondral Lesions
|
Full-thickness defects with clear mechanical symptoms
: Microfracture, chondroplasty.
Focal, symptomatic full-thickness defects (>2-4 cm²)
: Osteochondral autograft/allograft transfer (OATS), autologous chondrocyte implantation (ACI/MACI). | | |
|
Infections/Inflammation
|
Septic Arthritis
: Joint washout and targeted antibiotics.
Chronic Synovitis (e.g., PVNS, RA)
: Synovectomy if refractory to medical management. |
|
Loose Bodies
|
Symptomatic Loose Bodies
: Causing pain, catching, or mechanical locking. |
Pre-Operative Planning & Patient Positioning
Successful knee arthroscopy is predicated upon meticulous pre-operative planning and optimal patient positioning.
Pre-operative Assessment
- Comprehensive History: Detailed information regarding the onset, mechanism of injury (if traumatic), progression of symptoms, mechanical symptoms (locking, catching, giving way), pain characteristics, previous knee injuries or surgeries, and response to non-operative treatments. Assessment of patient activity level and expectations is crucial for surgical goal setting.
-
Thorough Physical Examination:
- Inspection: Swelling, effusion, ecchymosis, muscle atrophy, alignment abnormalities.
- Palpation: Joint line tenderness (meniscus), ligamentous insertions, patellar facets.
- Range of Motion (ROM): Active and passive, noting any limitations, crepitus, or pain.
- Ligamentous Stability Testing: Valgus/varus stress tests (MCL/LCL), Lachman test, Anterior Drawer, Pivot Shift (ACL), Posterior Drawer, Posterior Sag (PCL).
- Meniscal Tests: McMurray's test, Apley's grind test.
- Patellofemoral Assessment: Patellar apprehension, patellar tilt, J-sign, quadriceps alignment (Q-angle).
- Neurovascular Status: Essential to document baseline function.
-
Imaging Studies:
- Standard Radiographs: Anteroposterior (AP), lateral, Merchant (patellofemoral) views, and weight-bearing AP views (Rosenberg view) are standard to assess bony alignment, degenerative changes, osteophytes, and loose bodies. Full-length lower extremity alignment films may be indicated for significant varus/valgus deformities.
- Magnetic Resonance Imaging (MRI): The gold standard for evaluating soft tissue pathology, including meniscal tears, ligamentous injuries (ACL, PCL, collaterals), chondral defects, synovitis, and bone marrow edema.
- Computed Tomography (CT) Scan: Useful for complex intra-articular fractures, osteochondral defects, or assessing bony anatomy for tunnel placement in revision ligament surgery.
- Anesthesia Consultation: Evaluation of patient comorbidities. General anesthesia is common, but regional anesthesia (spinal or epidural) or a combination with peripheral nerve blocks (e.g., femoral nerve block, adductor canal block, sciatic nerve block) are frequently employed for improved post-operative analgesia.
- Pre-operative Optimization: Addressing any modifiable risk factors (e.g., smoking cessation, glycemic control in diabetics, nutritional optimization). Review of medications, especially anticoagulants or antiplatelet agents, to manage bleeding risk.
Patient Positioning and Preparation
-
Positioning on the Operating Table:
The patient is typically positioned supine.
- Tourniquet Application: A pneumatic tourniquet is applied high on the ipsilateral thigh. It is typically inflated after exsanguination of the limb with an Esmarch bandage, set to a pressure of 250-350 mmHg or approximately 100 mmHg above the patient's systolic blood pressure. The use of a tourniquet improves visualization by minimizing bleeding, but care must be taken to minimize inflation time to reduce risks of nerve palsy or compartment syndrome. Some surgeons elect not to use a tourniquet for certain procedures to assess dynamic vascularity or in cases with significant vascular disease.
- Leg Holder/Post: The leg may be placed in a specialized knee holder that allows free flexion and extension, or the foot of the bed can be broken or lowered. For medial or lateral compartment access, a lateral post or thigh holder can be used to apply a valgus or varus stress, respectively, opening the desired compartment. Adequate padding is essential under the tourniquet, peroneal nerve region, and all pressure points to prevent skin breakdown or neuropathies.
- Leg Draping: The entire lower extremity, from the midthigh to the ankle or foot, is prepared with an antiseptic solution (e.g., povidone-iodine or chlorhexidine gluconate) and draped sterilely. This allows for manipulation of the entire limb during the procedure. An impervious stockinette may be rolled up to the mid-thigh, and the foot and ankle often wrapped in a sterile self-adherent wrap, leaving the knee free for manipulation.
Joint Distension and Fluid Management
An arthroscopy pump is used to deliver continuous irrigation fluid (typically lactated Ringer's solution or normal saline) into the joint.
*
Functions:
Distends the joint capsule, separates articular surfaces, flushes out debris and blood, and improves visualization.
*
Pressure Management:
The pump pressure is typically set between 40-80 mmHg, adjusted to optimize visualization and manage extravasation. Excessive pressure or prolonged operative time can lead to significant fluid extravasation into surrounding soft tissues, potentially causing pain, swelling, and rarely, compartment syndrome. Some procedures, particularly those involving thermal ablation or shaver use, may require higher pressures to maintain clarity.
Detailed Surgical Approach / Technique
The general principles of arthroscopy involve establishing portals, systematic diagnostic evaluation, and subsequent therapeutic interventions specific to the pathology. The following outlines a common approach.
Portal Placement
Portal placement is critical to safely and effectively access the entire knee joint. Skin incisions are typically small (5-7 mm) and vertical or oblique.
1.
Anterolateral (AL) Portal:
*
Location:
Typically established first, approximately 1 cm lateral to the patellar tendon and at or slightly above the superior pole of the joint line.
*
Function:
Primary viewing portal.
*
Technique:
After local infiltration, a small skin incision is made. A blunt trocar and cannula are advanced through the capsule and synovium, aiming towards the intercondylar notch. Confirmation of intra-articular placement is obtained by observing fluid egress.
2.
Anteromedial (AM) Portal:
*
Location:
Approximately 1 cm medial to the patellar tendon and at or slightly above the joint line.
*
Function:
Primary working portal.
*
Technique:
Often created under direct arthroscopic visualization (from the AL portal) using an "inside-out" technique to ensure optimal positioning and prevent iatrogenic damage to articular cartilage or menisci. A spinal needle is first inserted to identify the ideal entry point. The needle tip should be visualized entering the intercondylar notch, avoiding the femoral condyles, tibial plateau, and menisci. Once the optimal position is confirmed, the skin incision is made, and a blunt trocar is advanced along the path of the needle. Care is taken to avoid injury to the infrapatellar branch of the saphenous nerve and saphenous vein.
3.
Accessory Portals (as needed):
*
Superolateral/Superomedial Portals:
Located superior to the patella, either for inflow (if the AL portal is used for instrumentation), accessory instrument insertion, or loose body retrieval.
*
Posteromedial (PM) Portal:
*
Location:
Typically 1 cm proximal to the medial joint line and 1 cm posterior to the posterior margin of the MCL.
*
Function:
Visualizes the posterior horn of the medial meniscus, posterior cruciate ligament (PCL), and posterior compartment.
*
Technique:
Established with caution due to the proximity of the saphenous nerve and vein anteriorly and the popliteal neurovascular bundle posteriorly. Often performed by transilluminating from the anterior portal or using an outside-in technique with a spinal needle for localization.
*
Posterolateral (PL) Portal:
*
Location:
Often aligned with the lateral femoral epicondyle, slightly posterior.
*
Function:
Visualizes the posterior horn of the lateral meniscus, popliteus tendon, and posterior compartment.
*
Technique:
Extremely close to the common peroneal nerve. Should be made with careful palpation for the fibular head and nerve, and preferably under direct visualization or with a spinal needle.
*
Transpatellar Tendon Portal:
Less common, used for specific patellofemoral or intercondylar notch pathology, but risks weakening the patellar tendon.
Diagnostic Arthroscopy: A Systematic Joint Survey
Once portals are established and joint distension achieved, a systematic diagnostic arthroscopy is performed to evaluate all compartments.
1.
Suprapatellar Pouch:
* Inspect the patellofemoral joint: Patellar cartilage, femoral trochlea, patellar tracking during flexion/extension.
* Assess for synovial hypertrophy, plicae (medial patellar plica), and loose bodies.
2.
Medial Gutter:
* Evaluate the space between the patella and medial femoral condyle for loose bodies, synovitis.
3.
Medial Compartment:
* Thoroughly inspect the medial femoral condyle and medial tibial plateau articular cartilage.
* Evaluate the medial meniscus: Probe the entire meniscus from anterior to posterior horn to assess stability, tear patterns (longitudinal, radial, horizontal, complex), and tissue quality. Assess the attachment to the capsule (meniscocapsular separation).
* Assess the MCL: Its integrity can be observed indirectly.
4.
Intercondylar Notch:
* Evaluate the Anterior Cruciate Ligament (ACL): Assess fiber continuity, tension, and any impingement. Distinguish between AM and PL bundles if possible.
* Evaluate the Posterior Cruciate Ligament (PCL): Assess its integrity and tension, typically visualized by looking posteriorly through the notch.
* Identify any loose bodies or cyclops lesions (fibrous nodule after ACL reconstruction).
5.
Lateral Compartment:
* Inspect the lateral femoral condyle and lateral tibial plateau articular cartilage.
* Evaluate the lateral meniscus: Probe for stability and tear patterns. Note the popliteal hiatus and its relation to the lateral meniscus.
* Assess the LCL and popliteus tendon from within the joint, though these are largely extracapsular.
6.
Lateral Gutter:
* Assess for loose bodies, synovitis.
7.
Posterior Compartments (if indicated):
* Using a 70-degree arthroscope through anterior portals or dedicated posterior portals, visualize the posterior aspects of menisci, PCL, and assess for loose bodies, synovial pathology, or Baker's cyst communication.
Therapeutic Procedures (Common Examples)
The therapeutic phase involves specific interventions based on the identified pathology.
1.
Partial Meniscectomy:
*
Principle:
Resect only the unstable, irreparable portion of the meniscus, preserving as much healthy tissue as possible to maintain function and prevent early degeneration.
*
Technique:
Unstable flaps or torn fragments are grasped with basket forceps and resected. A motorized shaver is used to smooth the remaining rim, ensuring no unstable edges remain to catch or cause further symptoms. A stable meniscal rim is critical.
2.
Meniscal Repair:
*
Principle:
Suture unstable meniscal tears, primarily in the vascular red-red or red-white zones, to restore meniscal function.
*
Tear Patterns:
Vertical longitudinal (bucket-handle) tears are ideal for repair. Radial and root tears may also be repaired with specific techniques.
*
Techniques:
*
Inside-out:
Sutures are placed from inside the joint, exited through the capsule, and tied over a knot on the capsule/soft tissue outside. Requires a small incision to retrieve and tie sutures.
*
Outside-in:
Needles are passed from outside the joint, through the capsule and meniscus, and retrieved intra-articularly for knot tying.
*
All-inside:
Utilizes specialized devices that deploy anchors and sutures entirely within the joint, eliminating the need for accessory incisions. These devices have evolved significantly, offering various designs.
*
Factors influencing success:
Tear location (vascularity), tear length, tear stability, chronicity of tear, and concomitant ACL reconstruction (which increases vascular inflow to the meniscus).
3.
ACL Reconstruction:
*
Principle:
Restore anterior-posterior and rotational stability of the knee by replacing the torn ACL with a graft.
*
Graft Choice:
Common autografts include patellar tendon (bone-patellar tendon-bone, BPTB), hamstring tendon (semitendinosus and gracilis), and quadriceps tendon. Allografts (tibialis anterior, patellar tendon) are also used.
*
Steps:
*
Debridement:
Arthroscopic debridement of torn ACL remnants from the intercondylar notch.
*
Graft Harvest:
If using autograft, this is performed prior to or concurrently with arthroscopic debridement.
*
Femoral Tunnel Creation:
Key for anatomical reconstruction. Techniques include the anteromedial (AM) portal technique (allowing a more anatomical placement) or transtibial drilling. The tunnel should be placed to replicate the native ACL footprint, often aiming for the "over-the-top" or "anatomic" position.
*
Tibial Tunnel Creation:
Drilled from the anteromedial tibia into the ACL footprint on the tibial plateau, ensuring proper angle to prevent impingement.
*
Graft Passage:
The graft is passed through the tibial and femoral tunnels.
*
Graft Fixation:
Various methods exist, including interference screws (metal or bioabsorbable), suspensory devices (endobuttons), staples, or post screws. Fixation should be strong enough to allow early motion and facilitate graft incorporation.
4.
Chondroplasty/Microfracture:
*
Principle:
Address focal chondral defects. Chondroplasty involves debriding unstable cartilage flaps to a stable rim. Microfracture aims to stimulate fibrocartilage formation from mesenchymal stem cells in the subchondral bone marrow.
*
Technique (Microfracture):
After debridement of unstable cartilage, the subchondral bone is perforated using an awl or K-wire to create bleeding and expose marrow elements.
*
Indications:
Small, contained full-thickness defects (<2-4 cm²), especially on weight-bearing surfaces.
5.
Loose Body Removal:
*
Principle:
Identify and remove intra-articular fragments (cartilage, bone, synovium) causing mechanical symptoms.
*
Technique:
Localization with the arthroscope, grasping with specialized forceps, and extraction through an existing or accessory portal. Shavers or suction may aid in fragmentation or removal of smaller pieces.
6.
Synovectomy:
*
Principle:
Remove inflamed or hypertrophic synovial tissue.
*
Technique:
Motorized shavers are used to resect pathological synovium throughout the joint.
7.
Plica Excision:
*
Principle:
Resect a thickened, symptomatic synovial plica causing impingement.
*
Technique:
The plica is identified and resected using a shaver or electrocautery.
Closure
After ensuring hemostasis and confirming removal of all instruments and foreign bodies, the portals are closed. Typically, a single suture (e.g., 3-0 Nylon or absorbable suture) closes the skin, or Steri-Strips are applied. A sterile dressing is applied, often with a compressive wrap or brace.
Complications & Management
While knee arthroscopy is considered a safe procedure with a relatively low complication rate, awareness and prompt management of potential adverse events are crucial.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approximate) | Etiology/Mechanism |
|
Other Conditions
|
Synovial Chondromatosis
: Arthroscopic removal of loose cartilage/bone fragments.
Loose Bodies
: Arthroscopic removal.
Plica Syndrome
: Arthroscopic resection if conservative care fails.
Septic Arthritis
: Emergent arthroscopic lavage and debridement. | |
| |
| |
|
Traumatic Injuries
|
ACL/PCL Reconstruction
: For functional instability.
Complex Meniscal Tears
: Repair if repairable, otherwise partial meniscectomy for unstable tears.
Tibial Plateau/Intercondylar Avulsion Fractures
: Arthroscopic-assisted reduction and internal fixation. | | | | | |
You Might Also Like