Find Your Best Knee Arthroscopy Doctor in San Jose, CA
Key Takeaway
For anyone wondering about Find Your Best Knee Arthroscopy Doctor in San Jose, CA, Knee arthroscopy is a minimally invasive surgical procedure using a tiny camera and specialized instruments to diagnose and treat problems inside the knee joint, such as torn meniscus or ACL tears. This technique offers less pain, fewer complications, and faster recovery. Residents in san jose ca can find top-rated surgeons to address knee pain, stiffness, and reduced mobility effectively.
Introduction & Epidemiology
Knee arthroscopy has fundamentally transformed the diagnostic and therapeutic landscape for intra-articular knee pathologies since its inception in the early 20th century, particularly gaining widespread adoption and refinement in the latter half. Initially a tool for diagnostic visualization, advancements in instrument miniaturization, optical technology, and surgical technique have established arthroscopy as the gold standard for numerous knee conditions, offering a minimally invasive alternative to traditional open arthrotomy. This approach is associated with reduced post-operative pain, shorter hospital stays, accelerated rehabilitation, and improved cosmetic outcomes.
Epidemiologically, knee pain remains a leading cause of musculoskeletal disability, contributing significantly to healthcare burden. The global prevalence of knee pain is high, with various etiologies ranging from traumatic injuries (e.g., meniscal tears, ligamentous ruptures) to degenerative processes (e.g., osteoarthritis, chondral lesions) and inflammatory conditions. Arthroscopic knee procedures are among the most frequently performed orthopedic surgeries worldwide. Data from various national registries consistently demonstrate high volumes of knee arthroscopy, with demographics varying based on the primary indication. For instance, meniscal repairs and ACL reconstructions are more prevalent in younger, active populations, while arthroscopic debridement and loose body removal may be more common across a broader age spectrum. Understanding the evolving indications, technical nuances, potential complications, and evidence-based post-operative management strategies is paramount for contemporary orthopedic practice.
Surgical Anatomy & Biomechanics
A thorough understanding of knee anatomy and biomechanics is foundational to successful arthroscopic intervention. The knee is a complex diarthrodial hinge joint, primarily involving the articulation between the distal femur and proximal tibia, with the patella articulating with the femoral trochlea.
Relevant Intra-Articular Structures
-
Menisci
: The medial and lateral menisci are crescent-shaped fibrocartilaginous structures that deepen the tibial plateau, distribute axial loads, absorb shock, enhance joint stability, and contribute to joint lubrication.
- Medial Meniscus : C-shaped, broader posteriorly, and more firmly attached to the tibia via the coronary ligaments and deep medial collateral ligament, making it less mobile and thus more prone to injury. Its anterior horn attaches to the intercondylar area, and its posterior horn attaches just anterior to the PCL insertion.
- Lateral Meniscus : More O-shaped, smaller coverage area, and more mobile due to its looser attachments and connection to the popliteus tendon. Its anterior horn attaches to the intercondylar area, and its posterior horn attaches to the lateral tibial spine. The popliteal hiatus is a critical landmark.
- Vascularity : The outer one-third (red-red zone) is vascularized by genicular arteries and has healing potential. The inner two-thirds (white-red and white-white zones) are largely avascular, limiting intrinsic healing.
- Articular Cartilage : Hyaline cartilage covers the femoral condyles, tibial plateaus, and posterior patellar facet. Its primary function is to reduce friction and distribute loads across the joint surfaces. Cartilage defects can range from fibrillation to full-thickness chondral lesions, often leading to progressive degeneration.
-
Ligaments
:
- Anterior Cruciate Ligament (ACL) : Originates from the posteromedial aspect of the lateral femoral condyle and inserts into the anteromedial aspect of the tibial intercondylar eminence. It resists anterior tibial translation and rotational forces. Its two main bundles are the anteromedial (taut in flexion) and posterolateral (taut in extension).
- Posterior Cruciate Ligament (PCL) : Originates from the anterolateral aspect of the medial femoral condyle and inserts into the posterior aspect of the tibial intercondylar eminence. It resists posterior tibial translation.
- Medial Collateral Ligament (MCL) : Composed of superficial and deep layers. Resists valgus stress. The deep layer blends with the medial meniscus.
- Lateral Collateral Ligament (LCL) : A cord-like structure extending from the lateral femoral epicondyle to the fibular head. Resists varus stress. Part of the posterolateral corner (PLC).
- Synovium : The synovial membrane lines the joint capsule, excluding articular cartilage. It produces synovial fluid, which lubricates the joint and nourishes the avascular cartilage. Synovial plicae (medial patellar plica, suprapatellar plica) are common anatomical variants, occasionally symptomatic.
- Patellofemoral Joint : Articulation between the patella and femoral trochlea. Its stability relies on bony congruence, static soft tissue restraints (medial patellofemoral ligament MPFL, lateral retinaculum), and dynamic stabilizers (quadriceps mechanism).
Biomechanical Considerations for Arthroscopy
- Load Transmission : Menisci bear significant loads (up to 50% in extension, 85% in 90° flexion). Meniscectomy significantly increases contact pressures on articular cartilage, accelerating degenerative changes. Meniscal repair aims to preserve this crucial biomechanical function.
- Joint Stability : The cruciates are primary stabilizers, while collaterals are secondary. Arthroscopic ligament reconstruction aims to restore native kinematics and stability patterns, requiring precise tunnel placement and graft tensioning.
- Cartilage Healing : Articular cartilage has limited intrinsic healing capacity due to its avascular nature. Arthroscopic techniques for chondral defects (microfracture, OATS, ACI) aim to stimulate fibrocartilage or hyaline-like cartilage formation.
- Kinematics : Understanding the "screw-home" mechanism, patellar tracking, and the coupled motions of the tibiofemoral joint (e.g., during ACL reconstruction) is essential for successful functional restoration.
Indications & Contraindications
Knee arthroscopy is indicated for a wide array of intra-articular pathologies that have failed non-operative management or require definitive surgical intervention. Patient selection is critical to optimize outcomes.
Indications for Arthroscopy
| Indication Category | Operative (Arthroscopic) | Non-Operative |
|---|---|---|
| Meniscal Pathology | Symptomatic meniscal tears (degenerative, traumatic, meniscal cyst) unresponsive to conservative treatment, unstable tears amenable to repair (e.g., vertical longitudinal, bucket-handle, root tears). | Asymptomatic tears, stable tears (e.g., small, horizontal cleavage tears) in patients without mechanical symptoms, patients with severe degenerative arthritis where meniscectomy may exacerbate symptoms, patients with contraindications to surgery. |
| Ligamentous Pathology | ACL rupture (primary indication for reconstruction in active individuals), PCL rupture (selective cases), symptomatic chronic instability after MCL/LCL tears (rarely addressed in isolation arthroscopically, often part of multi-ligament injury). | Acute partial ACL/PCL tears with minimal instability, low-demand individuals, isolated grade I/II MCL/LCL injuries, patients with significant medical comorbidities precluding surgery. |
| Articular Cartilage Lesions | Symptomatic chondral defects (traumatic or focal degenerative) amenable to marrow stimulation (microfracture, drilling), osteochondral autograft/allograft transplantation, or autologous chondrocyte implantation. | Asymptomatic lesions, diffuse severe osteoarthritis (arthroplasty indicated), lesions with spontaneous healing potential (e.g., very small, superficial), patients opting for conservative management. |
| Synovial Pathology | Symptomatic plicae (medial patellar plica syndrome), pigmented villonodular synovitis (PVNS), synovial chondromatosis, persistent synovitis unresponsive to medical management, removal of synovial impingement. | Asymptomatic plicae, mild synovitis responsive to NSAIDs/injections, diffuse inflammatory arthritis (medical management primary). |
| Loose Bodies | Symptomatic intra-articular loose bodies causing locking, catching, or pain. | Asymptomatic, non-impinging loose bodies, small loose bodies in patients with severe diffuse osteoarthritis. |
| Patellofemoral Pathology | Recurrent patellar dislocation (medial patellofemoral ligament reconstruction, lateral retinacular release), chondromalacia patellae with mechanical symptoms (chondroplasty, debridement), symptomatic plicae. | Asymptomatic instability, patellofemoral pain syndrome without mechanical symptoms (physical therapy focus), diffuse patellofemoral osteoarthritis. |
| Arthrofibrosis/Stiffness | Persistent mechanical blockage or significant loss of range of motion post-injury or surgery unresponsive to aggressive physical therapy. | Mild stiffness responsive to physical therapy, patients with ongoing infection, complex regional pain syndrome. |
| Diagnostic Arthroscopy | Unexplained knee pain, swelling, or mechanical symptoms refractory to thorough non-invasive workup (imaging, physical exam) when an intra-articular pathology is suspected. | When non-invasive diagnostic tools (MRI, clinical exam) provide a clear diagnosis and guide treatment, or when a clear contraindication to surgery exists. |
Contraindications to Arthroscopy
Absolute Contraindications:
* Active local or systemic infection (e.g., septic arthritis, cellulitis overlying surgical site).
* Severe uncontrolled medical comorbidities precluding safe anesthesia and surgery (e.g., unstable angina, recent MI, severe coagulopathy).
* Ankylosed knee joint.
* Poor skin integrity or active skin lesions in the surgical field.
Relative Contraindications:
* Severe diffuse osteoarthritis (arthroplasty often preferred if symptoms are debilitating).
* Extreme obesity (increased technical difficulty, higher complication rates).
* Severe arthrofibrosis (may require open approach or staged procedures).
* Severe neurovascular disease of the lower extremity.
* Complex regional pain syndrome (CRPS).
* Inability to comply with post-operative rehabilitation protocols.
* Venous stasis or severe peripheral vascular disease.
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for optimizing surgical efficiency and minimizing complications.
Pre-Operative Planning
- Patient History and Physical Examination : Detailed history including mechanism of injury, symptom duration, mechanical symptoms (locking, catching, giving way), pain characteristics, and functional limitations. Comprehensive physical exam assessing range of motion, effusion, tenderness, ligamentous stability (Lachman, pivot shift, posterior drawer, varus/valgus stress), and meniscal signs (McMurray, Apley).
-
Imaging Review
:
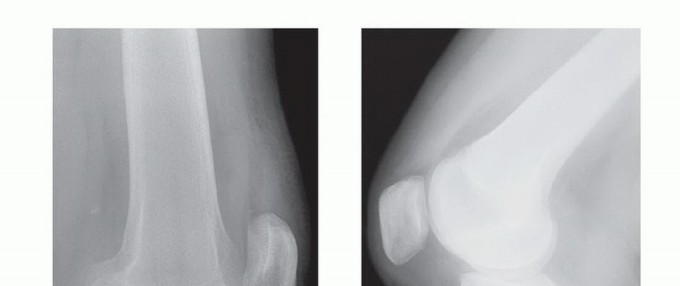
- Radiographs : AP, lateral, Merchant (patellofemoral), and weight-bearing views are essential to assess bony alignment, joint space narrowing, osteophytes, and loose bodies.
- MRI : The gold standard for evaluating soft tissue pathology (menisci, ligaments, articular cartilage, synovium, bone marrow edema). Correlate MRI findings with clinical symptoms.
- CT : May be useful for complex fractures, osteochondral defects, or assessing patellofemoral trochlear morphology (e.g., trochlear dysplasia).
- Anesthesia Consultation : Assess patient's fitness for anesthesia (general, regional, or local with sedation). Regional anesthesia (spinal, epidural, or femoral nerve block) can provide excellent post-operative pain control.
- Equipment Review : Ensure all necessary arthroscopic instruments, power tools, fluid management systems, and imaging equipment are available and functional. Anticipate specific repair devices (e.g., meniscal repair kits, ACL graft preparation tools).
Patient Positioning
The most common position for knee arthroscopy is supine, typically with the operative leg secured in a leg holder or suspended to allow full knee flexion.
-
Supine Position :
- Setup : Patient supine on the operating table. A pneumatic tourniquet is applied to the proximal thigh of the operative leg, padded adequately. The contralateral leg is supported.
- Leg Suspension : The operative leg can be suspended in a commercially available leg holder/distraction tower or manually held by an assistant. Leg holders facilitate manipulation, allowing various degrees of flexion and valgus/varus stress. Manual holding offers greater flexibility but requires a dedicated assistant.
- Foot Holder : A foot holder can be used to apply traction or to maintain knee flexion, particularly useful for diagnostic arthroscopy and posterior compartment viewing.
- Pad Positioning : A bump under the ipsilateral gluteal region may be used to internally rotate the hip, facilitating portal placement and access to the lateral compartment.
- Fluid Management : An arthroscopy pump is connected to an inflow cannula, regulating joint distension pressure and flow rate. This helps maintain visualization and washes away debris.
- Limb Prep and Drape : Standard sterile preparation and draping to expose the entire knee from mid-thigh to mid-calf.
-
Alternatives (Less Common for Primary Arthroscopy) :
- Lateral Decubitus : Occasionally used for specific posterior compartment approaches or complex multi-ligament reconstructions.
- PCL Positioning : For specific PCL reconstruction techniques, a prone or exaggerated supine flexion position may be utilized.
Detailed Surgical Approach / Technique

The arthroscopic procedure generally follows a systematic sequence: portal creation, diagnostic arthroscopy, and then targeted therapeutic interventions. A thorough understanding of anatomical landmarks and intra-articular relationships is paramount.
Portal Placement
Standard portals provide access to the various compartments of the knee. Careful placement avoids neurovascular structures.
-
Anteromedial (AM) Portal :
- Location : Typically 1 cm medial to the patellar tendon, at or just above the joint line.
- Purpose : Primary viewing portal for the lateral compartment, secondary working portal for the medial compartment. Often used for inflow.
- Neurovascular Consideration : Avoid the infrapatellar branch of the saphenous nerve.
-
Anterolateral (AL) Portal :
- Location : Typically 1 cm lateral to the patellar tendon, at or just above the joint line.
- Purpose : Primary viewing portal for the medial compartment, secondary working portal for the lateral compartment.
- Neurovascular Consideration : Avoid the common peroneal nerve laterally (though less risk at this anterior location).
-
Superomedial / Superolateral Portals :
- Location : Proximal to the patella, either medial or lateral to the quadriceps tendon.
- Purpose : Primarily for inflow, outflow, or access to the suprapatellar pouch.
- Neurovascular Consideration : Generally safer as no major neurovascular structures are in close proximity here.
-
Posteromedial (PM) Portal :
- Location : Approximately 1 cm posterior and 1 cm distal to the medial femoral epicondyle, anterior to the medial head of the gastrocnemius.
- Purpose : Essential for viewing and treating posterior horn meniscal pathology (medial), loose bodies in the posterior compartment, and PCL visualization.
- Neurovascular Consideration : Proximity to the saphenous nerve and artery, and care must be taken to avoid the posterior capsule and neurovascular bundle in the popliteal fossa. A transillumination technique and careful cannula insertion are recommended.
-
Posterolateral (PL) Portal :
- Location : Approximately 1 cm posterior and 1 cm distal to the lateral femoral epicondyle, anterior to the lateral head of the gastrocnemius.
- Purpose : Viewing and treating posterior horn meniscal pathology (lateral), popliteus tendon region, posterolateral corner.
- Neurovascular Consideration : High risk for common peroneal nerve injury. Often performed under direct arthroscopic visualization from an anterior portal by "splitting" the interval between the lateral head of the gastrocnemius and the iliotibial band.
Diagnostic Arthroscopy: Systematic Evaluation
A systematic approach ensures no pathology is missed. Typically, the scope is inserted through the AL portal, and inflow through the AM portal.
- Suprapatellar Pouch : Evaluate patellar articular cartilage, femoral trochlea, quadriceps tendon, plicae (medial patellar, suprapatellar), and any loose bodies or synovitis.
- Patellofemoral Joint : Flex and extend the knee to assess patellar tracking and articular cartilage integrity.
- Medial Gutter : Inspect the medial wall of the intercondylar notch, including the PCL and medial femoral condyle.
-
Medial Compartment
:
- Insert the scope into the medial compartment (often requires valgus stress or "figure-of-four" position).
- Inspect the medial femoral condyle, medial tibial plateau, and the entire medial meniscus (anterior horn, body, posterior horn). Probe the meniscus for stability, tears, and meniscocapsular separation.
- Evaluate the MCL.
-
Intercondylar Notch
:
- Identify the ACL, assessing its integrity, tension, and any tears.
- Identify the PCL, assessing its integrity.
- Inspect the roof of the notch for impingement or osteophytes.
-
Lateral Compartment
:
- Insert the scope into the lateral compartment (often requires varus stress).
- Inspect the lateral femoral condyle, lateral tibial plateau, and the entire lateral meniscus. Probe for tears, stability, and popliteus tendon impingement.
- Evaluate the LCL and popliteus tendon.
-
Posterior Compartment (if indicated)
:
- Utilize PM/PL portals or "drive-through" technique (passing the scope through the intercondylar notch into the posterior compartment).
- Inspect posterior horns of menisci, posterior capsule, and loose bodies.
Therapeutic Arthroscopy: Common Procedures
Once pathologies are identified, appropriate therapeutic interventions are performed.
Meniscal Pathology
-
Partial Meniscectomy (Debridement)
:
- Indications : Irreparable meniscal tears (complex, degenerative, tears in avascular zones), or stable tears causing mechanical symptoms where repair is not feasible.
- Technique : Using grasping forceps and motorized shavers, unstable, fibrillated, or torn portions of the meniscus are resected back to a stable rim. The goal is to preserve as much functional meniscal tissue as possible to maintain load-bearing capacity. Smooth the edges to prevent further tearing or mechanical irritation.
-
Meniscal Repair
:
- Indications : Acute, unstable, vertical longitudinal tears, bucket-handle tears, and radial tears in the vascular (red-red or red-white) zones, especially in younger, active patients. Meniscal root tears are a specific indication for repair.
-
Technique
:
- Preparation : Roughening the tear edges and capsule to promote healing, often by debridement or trephination.
-
Repair Methods
:
- Inside-Out : Requires accessory incisions for suture passage and tying. Provides strong, reproducible repairs.
- Outside-In : Useful for anterior horn tears or difficult-to-reach areas.
- All-Inside : Utilizes specialized devices (e.g., fasteners, anchors, sutures) delivered entirely arthroscopically. Minimizes soft tissue dissection but may have higher costs and specific learning curves.
- Fixation : Restore the anatomical configuration of the meniscus, aiming for stable apposition of the torn edges. Evaluate stability with probing.
Articular Cartilage Lesions
-
Chondroplasty/Debridement
:
- Indications : Fibrillation, unstable flaps of articular cartilage, or minor defects.
- Technique : Using shavers or motorized burrs, unstable cartilage is debrided back to a stable rim. Avoid excessive removal of healthy tissue.
-
Marrow Stimulation (Microfracture, Drilling, Abrasion Arthroplasty)
:
- Indications : Contained full-thickness chondral defects (ICRS Grade IV) with healthy surrounding cartilage and stable subchondral bone, typically < 2-4 cm², in younger patients.
- Technique (Microfracture) : After debriding the defect to stable margins, subchondral bone is perforated with an awl (microfracture awl) to create channels for mesenchymal stem cells and growth factors from the bone marrow to form a "superclot," leading to fibrocartilage formation.
-
Osteochondral Autograft Transplantation (OATS) / Allograft (OCA)
:
- Indications : Larger, symptomatic full-thickness defects. OATS for smaller defects (plugs harvested from less weight-bearing areas). OCA for larger defects, particularly in older patients.
- Technique : Arthroscopically or arthroscopically-assisted, cylindrical osteochondral plugs are harvested and press-fit into prepared recipient sites.
-
Autologous Chondrocyte Implantation (ACI) / Matrix-Associated Autologous Chondrocyte Implantation (MACI)
:
- Indications : Larger, unipolar full-thickness chondral defects (>4 cm²), in younger patients, often after failed marrow stimulation.
- Technique : A two-stage procedure (harvesting chondrocytes, then implanting them) or single-stage MACI where chondrocytes are cultured on a scaffold prior to implantation. Often requires an arthrotomy.
Ligamentous Instability (e.g., ACL Reconstruction Principles)
While a full ACL reconstruction is extensive, arthroscopy is central to the procedure.
- Graft Harvest : Can be performed open or arthroscopically-assisted (e.g., hamstring tendon autograft from semitendinosus and gracilis, patellar tendon autograft, quadriceps tendon autograft).
-
Femoral Tunnel Creation
:
- Transtibial : The femoral tunnel is drilled through the tibial tunnel, limiting anatomical placement.
- Anteromedial (AM) Portal : Allows for independent drilling of the femoral tunnel, facilitating more anatomical placement on the femoral footprint.
- Outside-In : Femoral tunnel is drilled from the lateral cortex of the femur, also allowing anatomical placement.
- Tibial Tunnel Creation : Drilled through the tibia from an anteromedial approach, aiming for the anatomical footprint of the ACL on the tibia.
- Graft Passage and Fixation : The prepared graft is passed through the tunnels and fixed securely in both the femur and tibia using various methods (interference screws, suspensory devices, staples, posts) to achieve appropriate tension and provide stability.
Synovial Pathology & Loose Bodies
-
Synovectomy
:
- Indications : Chronic inflammatory synovitis (e.g., PVNS), symptomatic plicae, or persistent synovitis refractory to medical treatment.
- Technique : Using motorized shavers and electrocautery, hypertrophic or inflamed synovial tissue is resected.
-
Loose Body Removal
:
- Indications : Symptomatic intra-articular loose bodies causing mechanical symptoms.
- Technique : Loose bodies are identified, often manipulated into an accessible area, and removed using grasping forceps or suction cannulas. Large loose bodies may require enlargement of a portal or creation of an accessory portal.
Complications & Management
While knee arthroscopy is generally safe, a range of complications can occur. Recognition and prompt management are crucial.
| Complication | Incidence (Approx.) | Salvage / Management Strategy |
|---|---|---|
| Infection (Septic Arthritis) | 0.01% - 0.5% | Prompt irrigation and debridement (arthroscopic or open), IV broad-spectrum antibiotics, aspiration. |
| Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) | DVT: 0.1% - 1.5%; PE: 0.01% - 0.1% | Prophylactic anticoagulation (low molecular weight heparin, aspirin), early mobilization. Treatment: therapeutic anticoagulation, IVC filter for recurrent PE. |
| Neurovascular Injury | < 0.1% | Nerve : Direct repair if identified, neurolysis. Conservative management, physical therapy, pain control for neuropraxia. Vessel : Immediate surgical exploration, repair of vessel, management of compartment syndrome. |
| Arthrofibrosis / Stiffness | 1% - 5% | Intensive physical therapy, manipulation under anesthesia (MUA), arthroscopic lysis of adhesions, open arthrolysis for recalcitrant cases. |
| Reflex Sympathetic Dystrophy (CRPS) | < 0.1% - 1% | Multidisciplinary pain management, physical therapy, nerve blocks, sympathetic blocks, medication (gabapentin, tricyclic antidepressants). |
| Instrument Breakage / Retained Fragments | < 0.1% | Arthroscopic retrieval, open arthrotomy if not removable arthroscopically. Prevention: meticulous instrument handling. |
| Fluid Extravasation / Compartment Syndrome | < 0.1% (Compartment Syndrome) | Monitor fluid pressures, discontinue inflow, elevate limb, fasciotomy if compartment syndrome develops. Prevention: limit operative time, use appropriate pump pressures. |
| Haemarthrosis | 0.5% - 2% | Aspiration if severe, rest, ice, compression, elevation. Prevention: meticulous hemostasis. |
| Chondral Damage (Iatrogenic) | 0.1% - 0.5% | Varies by severity: observation, microfracture, debridement. Prevention: careful instrument insertion and manipulation. |
| Portal Site Complications | 1% - 5% (local) | Nerve injury (e.g., saphenous, peroneal) : Observation, neurolysis. Wound infection : Local wound care, antibiotics. Persistent drainage/sinus : Excision. |
| Anesthetic Complications | Rare, variable | Managed according to specific anesthetic event (e.g., anaphylaxis, aspiration, cardiac event). |
Management Principles
- Prevention : Adherence to sterile technique, meticulous hemostasis, careful portal placement, appropriate patient positioning, and experienced surgical technique are paramount.
- Early Recognition : Vigilance for signs and symptoms of complications (e.g., fever, increasing pain, swelling, neurological deficit, decreased range of motion).
- Prompt Intervention : Timely diagnosis and appropriate management (conservative, medical, or surgical) can significantly mitigate the long-term impact of complications. For instance, septic arthritis requires immediate and aggressive treatment to preserve joint function.
- Patient Education : Informing patients pre-operatively about potential complications and encouraging them to report any concerning symptoms post-operatively.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as the surgical procedure itself in achieving optimal functional outcomes. Protocols vary significantly based on the specific procedure performed, the extent of pathology, patient factors, and surgeon preference. However, general principles apply.
General Principles
- Pain and Swelling Management : RICE (Rest, Ice, Compression, Elevation) protocol, analgesics (NSAIDs, acetaminophen, opioids as needed).
- Early Mobilization : Preventing stiffness and promoting circulation, often within the limits of specific precautions.
- Protection of Surgical Repair : Strict adherence to weight-bearing restrictions, range of motion (ROM) limitations, and bracing, as dictated by the procedure.
- Gradual Progression : Rehabilitation is typically phased, progressing from protecting the repair to restoring full ROM, then strength, proprioception, and finally functional activities and return to sport.
- Patient Education and Compliance : Patients must understand their specific restrictions and the rationale behind them to ensure adherence.
Meniscectomy
-
Immediate Post-Op (Days 0-7)
:
- Weight-bearing: Generally full weight-bearing as tolerated (FWBAT) with crutches for comfort initially.
- ROM: Encourage full active and passive ROM within pain limits.
- Goals: Reduce pain/swelling, restore quadriceps activation, achieve full extension.
-
Intermediate Phase (Weeks 1-4)
:
- Progressive strengthening (quadriceps, hamstrings, gluteals).
- Balance and proprioception exercises.
- Gradual increase in activity.
- Return to Activity : Typically 3-6 weeks, depending on activity level and surgeon discretion.
Meniscal Repair
Meniscal repair protocols are more conservative due to the need for biological healing.
*
Immediate Post-Op (Weeks 0-4)
:
* Weight-bearing: Often non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) with crutches. Partial weight-bearing (PWB) may be allowed in flexion with a brace locked in extension.
* ROM: Limited, usually 0-90° flexion, with no active flexion against resistance, and limited terminal extension to protect the repair. Brace often locked in extension for ambulation.
* Goals: Control pain/swelling, protect repair, maintain quadriceps activation, achieve full passive extension.
*
Intermediate Phase (Weeks 4-12)
:
* Gradual increase in weight-bearing and ROM.
* Progressive strengthening, avoiding deep squats or loaded flexion initially.
* Initiate proprioception and balance exercises.
*
Advanced Phase (Weeks 12-24)
:
* Full weight-bearing and ROM.
* Advanced strengthening, agility, and sport-specific drills.
* Return to sport typically 4-6 months, often guided by clinical examination and functional testing.
ACL Reconstruction
ACL reconstruction protocols are aggressive but structured to protect the graft during its maturation phases (ligamentization).
*
Immediate Post-Op (Weeks 0-2)
:
* Weight-bearing: FWBAT with crutches and a brace. Some surgeons prefer locked extension for ambulation.
* ROM: Focus on achieving full passive extension immediately. Gradual progression of flexion (e.g., 0-90° by end of week 2).
* Goals: Control pain/swelling, achieve full extension, initiate quadriceps activation (neuromuscular electrical stimulation often used), patellar mobilization.
*
Early Strengthening (Weeks 2-6)
:
* Progressive ROM to full flexion.
* Closed-chain strengthening exercises (mini-squats, leg press) avoiding open-chain terminal knee extension against resistance to protect graft.
* Proprioception exercises.
*
Intermediate Phase (Weeks 6-16)
:
* Continue strengthening, incorporating balance and agility drills.
* Initiate light jogging and sport-specific movements if strength and mechanics allow.
* Emphasize neuromuscular control and proper landing mechanics.
*
Advanced Phase (Weeks 16-24+)
:
* Plyometric training, advanced agility, cutting drills.
* Isokinetic testing to assess strength symmetry.
*
Return to Sport (6-12 months)
:
* Criteria include symmetrical strength (typically >90% limb symmetry index), absence of pain/effusion, full ROM, excellent neuromuscular control, and successful completion of functional hop tests. Return to sport typically not before 6-9 months, with many favoring 9-12 months, especially for contact sports, due to ongoing graft maturation.
Summary of Key Literature / Guidelines
Contemporary knee arthroscopy practice is guided by a robust body of literature, including systematic reviews, meta-analyses, and clinical practice guidelines from organizations such as the American Academy of Orthopaedic Surgeons (AAOS), the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS), and the European Society of Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA).
Meniscal Pathology
:
*
Degenerative Meniscal Tears
: The role of arthroscopic partial meniscectomy for degenerative tears in the setting of mild-to-moderate osteoarthritis is highly debated. Multiple randomized controlled trials (e.g., TEAR study, KNEEMO study, Sihvonen et al.) have demonstrated that arthroscopic partial meniscectomy offers no significant benefit over conservative treatment (physical therapy) for such tears, particularly when mechanical symptoms like true locking are absent. Surgical intervention for these patients should be carefully considered, often favoring non-operative management initially.
*
Traumatic Meniscal Tears
: Repair is generally favored over meniscectomy in young, active patients with reparable tears (e.g., longitudinal tears in the red-red zone, bucket-handle tears) to preserve meniscal function and prevent accelerated osteoarthritis. The success rates for meniscal repair are influenced by tear pattern, location, stability, and patient age. Root repairs, while technically challenging, show promise in restoring tibiofemoral contact mechanics.
*
Meniscal Preservation
: Current guidelines strongly advocate for meniscal preservation whenever biologically and mechanically feasible, due to the critical role of menisci in load transmission and joint health.
ACL Reconstruction
:
*
Timing
: While early reconstruction for acute ACL tears was historically advocated, recent evidence suggests that delaying surgery to allow for pre-operative rehabilitation and swelling resolution may lead to improved range of motion and reduced rates of arthrofibrosis, without compromising graft outcomes.
*
Graft Choice
: Hamstring autografts, patellar tendon autografts, and quadriceps tendon autografts are the most common choices. Each has specific advantages and disadvantages concerning harvest site morbidity, graft strength, and bone integration. There is no single "best" graft, and choice is often individualized based on patient factors (age, activity level, sport), surgeon preference, and potential concomitant injuries. Allografts are typically reserved for revision surgeries or multi-ligament injuries due to concerns regarding disease transmission and slower incorporation.
*
Tunnel Placement
: Anatomical tunnel placement is crucial for restoring native knee kinematics and preventing impingement. Femoral tunnel placement via the anteromedial portal or an outside-in technique is often favored over a transtibial approach to achieve more anatomical graft positioning.
*
Accelerated Rehabilitation
: Evidence supports accelerated rehabilitation protocols focusing on early weight-bearing and full extension, while carefully protecting the graft during its ligamentization phase.
Articular Cartilage Repair
:
*
Marrow Stimulation
: Microfracture remains a cost-effective option for smaller, contained full-thickness chondral defects. However, it typically results in fibrocartilage formation, which is biomechanically inferior to hyaline cartilage and may degenerate over time.
*
Restorative Procedures
: OATS, OCA, ACI, and MACI are more complex procedures aimed at restoring hyaline or hyaline-like cartilage. Indications and outcomes vary, with these techniques often reserved for larger, focal defects in specific patient populations. The long-term durability of these treatments is an area of ongoing research.
Complications
:
*
Infection Prevention
: Strict aseptic technique, antibiotic prophylaxis (single dose intravenous cefazolin pre-incision), and meticulous fluid management are standard to minimize infection risk.
*
DVT Prophylaxis
: Routine prophylactic anticoagulation for all arthroscopic knee procedures is generally not recommended unless specific risk factors for VTE are present. Early mobilization is the cornerstone of prevention.
In conclusion, knee arthroscopy is a sophisticated surgical modality continuously evolving with technological advancements and a growing evidence base. Optimal outcomes are predicated on a nuanced understanding of knee anatomy and biomechanics, precise surgical technique, judicious patient selection, meticulous complication avoidance, and adherence to structured, evidence-based rehabilitation protocols. The role of arthroscopy continues to be refined, particularly concerning degenerative conditions, where careful consideration of non-operative alternatives is increasingly emphasized.
You Might Also Like