Master The Popliteal Fossa: Applied Surgical Anatomy of the Knee
Key Takeaway
This topic focuses on Master The Popliteal Fossa: Applied Surgical Anatomy of the Knee, The popliteal fossa is a diamond-shaped anatomical space located behind the knee joint. It is superiorly bounded by the semimembranosus, semitendinosus, and biceps femoris muscles, and inferiorly by the gastrocnemius heads. Its roof is formed by the popliteal fascia, with the floor comprising the distal femur. Understanding the anatomy of fossa the popliteal is crucial for posterior surgical approaches to the knee.
Master The Popliteal Fossa: Applied Surgical Anatomy of the Knee
Introduction & Epidemiology
The posterior aspect of the knee, dominated by the popliteal fossa, represents a critical anatomical region for orthopedic surgeons. While less frequently accessed than anterior or medial approaches, mastery of the popliteal fossa anatomy and the posterior approach to the knee is paramount for addressing a specific spectrum of pathologies. These include posterior cruciate ligament (PCL) avulsion fractures, complex posterior meniscal tears (especially root tears), popliteal cyst excision, management of posterior impingement osteophytes, posterior capsular releases, and specific neurovascular conditions such as popliteal artery entrapment syndrome.
Injuries to the posterior knee structures, particularly the PCL, are often high-energy events, frequently associated with multi-ligamentous trauma. While PCL injuries constitute a smaller percentage of all knee ligamentous injuries compared to anterior cruciate ligament (ACL) tears, their impact on knee stability and long-term joint health necessitates precise surgical management. Similarly, posterior horn meniscal root tears significantly disrupt meniscal function, leading to increased contact pressures and accelerating degenerative changes if not adequately addressed. Popliteal cysts, commonly known as Baker's cysts, while often asymptomatic, can cause significant pain and dysfunction, occasionally requiring surgical excision, particularly when they are large, symptomatic, or recur following conservative management.
The historical understanding of this region has evolved from rudimentary dissections to sophisticated imaging and minimally invasive techniques. However, open posterior approaches remain indispensable for complex reconstructions, direct repairs, or when arthroscopic access is limited or contraindicated. A thorough understanding of the intricate neurovascular and musculoskeletal relationships within the popliteal fossa is not merely academic but a fundamental prerequisite for safe and effective surgical intervention, minimizing iatrogenic injury and optimizing patient outcomes.
Surgical Anatomy & Biomechanics
The anatomy of the posterior approach to the knee is inextricably linked to the popliteal fossa, a diamond-shaped region located posteriorly to the knee joint. While classically described as diamond-shaped in cadaveric specimens, in live patients, the inferior "V" of the diamond, formed by the divergence of the gastrocnemius heads, is often less pronounced until these muscular heads are actively retracted.
Boundaries of the Popliteal Fossa
The well-defined borders of the popliteal fossa are critical for surgical orientation:
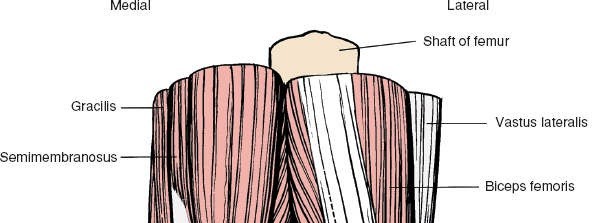
- Superomedial: Semimembranosus and semitendinosus muscles.
- Superolateral: Biceps femoris muscle.
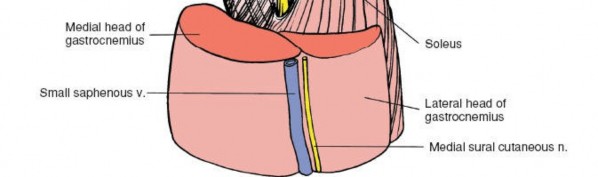
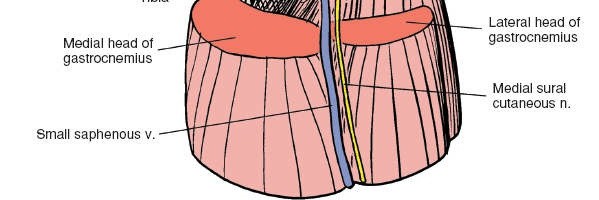
- Inferomedial: Medial head of the gastrocnemius muscle.
- Inferolateral: Lateral head of the gastrocnemius muscle.

Gross anatomical boundaries of the popliteal fossa.
Roof and Floor
- Roof: Formed by the popliteal fascia, which is a continuation of the fascia lata of the thigh and continuous with the crural fascia of the leg. This robust fascial layer provides structural support and helps contain the neurovascular structures. Overlying the fascia are the skin and subcutaneous tissues, which contain the small saphenous vein, posterior femoral cutaneous nerve branches, and the sural nerve.
- Floor: Composed of the popliteal surface of the distal femur, the posterior capsule of the knee joint, and the popliteus muscle, which overlies the proximal tibia.
Deep structures forming the floor of the popliteal fossa.
Contents of the Popliteal Fossa: The Neurovascular Triad
The most critical structures within the popliteal fossa are the popliteal artery, popliteal vein, and the tibial nerve, forming the neurovascular triad. Their relative positions are consistent, which is crucial for safe dissection:
- Tibial Nerve: Most superficial, lying immediately deep to the popliteal fascia, and the most lateral of the triad superiorly, becoming more superficial and midline as it descends. It gives off sural nerve branches and muscular branches to the gastrocnemius, soleus, plantaris, and popliteus.
- Popliteal Vein: Intermediate in depth, typically lying anterior (deep) to the tibial nerve.
- Popliteal Artery: Deepest, lying directly on the floor of the fossa (femur, capsule, popliteus muscle). It is a continuation of the femoral artery and gives off genicular branches around the knee.

Anatomical depiction of the neurovascular bundle: nerve, vein, artery relationship.
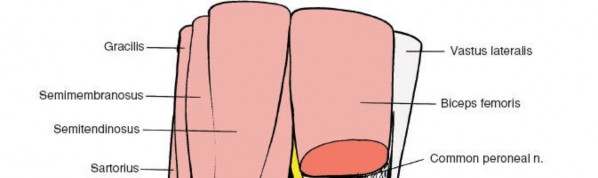
The common fibular (peroneal) nerve diverges from the tibial nerve superiorly in the fossa, coursing along the superolateral border (medial aspect of the biceps femoris tendon) and wrapping around the fibular head to enter the anterior compartment.
Muscular Anatomy
- Hamstring Muscles: The semimembranosus and semitendinosus insert on the posteromedial aspect of the proximal tibia (pes anserinus), while the biceps femoris inserts on the fibular head. These form the superior boundaries.
- Gastrocnemius Muscle: The medial and lateral heads originate from the femoral condyles, forming the inferior boundaries. They are superficial and must often be retracted. The plantaris muscle, a small, often rudimentary muscle, lies between the lateral head of the gastrocnemius and the soleus, with its long, slender tendon often mistaken for the common fibular nerve.
- Popliteus Muscle: Originates from the lateral femoral condyle and inserts onto the posteromedial aspect of the proximal tibia. It forms part of the floor of the fossa and is crucial for knee stability and internal rotation, "unlocking" the knee from extension.

Muscles forming the boundaries and floor of the popliteal fossa.
Ligamentous Structures and Capsule
Deep within the fossa, superficial to the popliteal artery, lies the posterior knee capsule. This robust structure is reinforced by several ligaments:
- Oblique Popliteal Ligament: A broad, flat band that reinforces the central posterior capsule, originating from the semimembranosus tendon and ascending superolaterally to the lateral femoral condyle.
- Arcuate Popliteal Ligament: Part of the posterolateral corner (PLC) complex, it originates from the fibular head and arches over the popliteus muscle, attaching to the lateral femoral condyle and posterior capsule.
- Posterior Cruciate Ligament (PCL): The primary posterior stabilizer of the knee, originating from the lateral aspect of the medial femoral condyle and inserting onto the posterior intercondylar area of the tibia. Direct access to its tibial insertion is a key indication for the posterior approach.
- Posterior Horns of Menisci: The posterior horns of both medial and lateral menisci lie deep to the capsule and are important for load transmission and stability.

Posterior view of knee ligaments, including the oblique and arcuate popliteal ligaments.
Bursae
The most clinically relevant bursa in this region is the gastrocnemius-semimembranosus bursa, which when enlarged and symptomatic forms a Baker's cyst. It typically communicates with the knee joint through a posteromedial capsular defect.
Biomechanics
The posterior structures of the knee collectively resist posterior tibial translation and provide rotational stability. The PCL is the primary restraint to posterior translation. The popliteus muscle and the posterolateral corner structures (arcuate ligament, popliteofibular ligament, lateral collateral ligament, popliteus tendon) are crucial for resisting posterolateral rotation and varus stress. Injury to these structures significantly compromises knee stability and function, often leading to progressive degenerative changes if not adequately managed.
Indications & Contraindications
The posterior approach to the knee is a targeted surgical exposure with specific indications and relatively few absolute contraindications.
Indications
The decision to approach the posterior knee surgically is based on the specific pathology, its location, and the need for direct visualization and repair.
Operative Indications (Posterior Approach Preferred/Required)
-
PCL Tibial Avulsion Fractures:
Direct reduction and internal fixation of the avulsed fragment (e.g., using screws or suture anchors).
Tibial avulsion fracture of the PCL, an indication for posterior approach. - PCL Reconstruction: Particularly for tibial inlay techniques, allowing direct access to create a bone tunnel or trough for graft fixation on the posterior tibia. This minimizes graft kinking and maximizes fixation strength.
-
Posterior Meniscal Pathologies:
- Posterior Horn Medial Meniscal Root Tears: Direct repair with suture anchors or transtibial pull-out sutures.
- Complex Posteromedial/Posterolateral Meniscal Tears: When arthroscopic access is limited or inadequate, or for concurrent posterior capsular repair.
- Popliteal Cysts (Baker's Cysts) Excision: Especially large, symptomatic, recurrent cysts, or those with underlying intra-articular pathology requiring open treatment. Direct visualization minimizes recurrence by addressing the stalk and underlying capsular defect.
- Excision of Posterior Osteophytes: Causing posterior impingement, often seen in advanced osteoarthritis or after trauma.
- Removal of Loose Bodies: When located in the posterior compartment and not amenable to arthroscopic retrieval.
- Popliteal Artery Entrapment Syndrome (PAES): Decompression of the popliteal artery due to anatomical variants of the gastrocnemius muscle or fibrous bands.
- Resection of Posterior Knee Tumors: Benign (e.g., osteochondroma) or malignant lesions located in the posterior compartment, requiring wide margins.
- Posterior Capsular Release: For severe flexion contractures not responsive to conservative measures.
- Repair of Posterolateral Corner (PLC) Injuries: In conjunction with other approaches, or for specific components like the popliteofibular ligament, if direct posterior access is advantageous.
Non-Operative Indications (Typically Managed Conservatively)
- Asymptomatic Popliteal Cysts: Most Baker's cysts are managed symptomatically, with aspiration, corticosteroid injection, or addressing underlying intra-articular pathology (e.g., meniscus tear, arthritis) via arthroscopy.
- Mild PCL Sprains (Grade I/II): Without avulsion, these are often managed with bracing, physical therapy, and activity modification.
- Minor Posterior Meniscal Tears: Without mechanical symptoms or instability, often managed conservatively.
- Minor Posterior Impingement: If symptoms are mild and responsive to NSAIDs, physical therapy, and activity modification.
Contraindications
-
Absolute Contraindications:
- Active infection in the surgical field or systemic sepsis.
- Severe, uncorrectable coagulopathy.
- Patient's medical comorbidities precluding safe anesthesia and surgery.
-
Relative Contraindications:
- Severe peripheral vascular disease: Increased risk of vascular compromise; requires careful preoperative evaluation and potential vascular surgery consultation.
- Prior extensive scarring, radiation, or chronic wounds in the popliteal fossa: Increases dissection difficulty and wound complication risk.
- Extreme obesity: May make dissection more challenging and increase risk of wound complications.
- Lack of clear surgical indication.
Table: Operative vs. Non-Operative Indications for Posterior Knee Pathology
| Indication Type | Operative (Posterior Approach) | Non-Operative (Conservative Management) |
|---|---|---|
| PCL Injury | PCL tibial avulsion fractures (repair/fixation) | Grade I/II PCL sprains (bracing, PT, activity modification) |
| PCL reconstruction (tibial inlay technique) | ||
| Meniscal Tears | Posterior horn meniscal root tears (repair) | Asymptomatic or small peripheral tears |
| Complex posteromedial/posterolateral tears (when arthroscopy fails) | ||
| Popliteal Cysts | Large, symptomatic, recurrent Baker's cysts (excision) | Asymptomatic cysts, small cysts, initial management of symptomatic cysts |
| Bony Pathologies | Posterior osteophytes causing impingement (excision) | Minor posterior impingement (NSAIDs, PT) |
| Removal of large/fixed posterior loose bodies | Small, asymptomatic loose bodies | |
| Resection of posterior knee tumors | ||
| Neurovascular | Popliteal Artery Entrapment Syndrome (decompression) | |
| Capsular | Severe flexion contracture (posterior capsular release) | Mild flexion contractures (PT, stretching) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical to optimize exposure, minimize complications, and ensure a successful outcome when approaching the posterior knee.
Pre-Operative Assessment
- Clinical Evaluation: A thorough history and physical examination are essential to identify the precise pathology, assess neurovascular status, and evaluate knee stability. Document pre-existing neurovascular deficits.
-
Imaging:
- Plain Radiographs: AP, lateral, and Merchant views to assess bony alignment, degenerative changes, and identify avulsion fractures or osteophytes.
- Magnetic Resonance Imaging (MRI): The gold standard for evaluating soft tissue pathology within the popliteal fossa, including PCL tears, meniscal lesions, posterior capsule integrity, presence of popliteal cysts, and neurovascular anatomy. It is crucial for delineating the spatial relationship of the lesion to the neurovascular bundle.
- Computed Tomography (CT) Scan: Indicated for complex tibial avulsion fractures to assess fragment size, displacement, and comminution.
- Vascular Studies (Doppler Ultrasound, CT Angiography, MRI Angiography): Essential if popliteal artery entrapment is suspected or if there are concerns about vascular patency, especially in cases of chronic swelling or claudication.

Pre-operative MRI demonstrating posterior knee pathology (e.g., PCL avulsion, meniscal tear, or Baker's cyst).
- Medical Optimization: Assess and optimize patient comorbidities to minimize anesthetic and surgical risks. Discuss DVT prophylaxis strategies.
- Informed Consent: Detailed discussion with the patient regarding the procedure, potential benefits, risks (especially neurovascular injury, infection, stiffness), and expected post-operative course.
Patient Positioning
The standard position for a posterior approach to the knee is prone .
- Anesthesia: General anesthesia is typically employed. Regional nerve blocks can be a useful adjunct for post-operative pain control.
-
Prone Position Setup:
- Patient is carefully transferred to the operating table and positioned prone.
- Support is crucial to prevent pressure points and ensure adequate exposure.
- Chest Rolls/Bolsters: Placed longitudinally from the clavicle to the iliac crest, medial to the shoulders and hips. This ensures the abdomen is free, allowing for unimpeded respiration and preventing vena caval compression.
- Thigh Bolster: A rolled sheet or specialized bolster placed transversely just proximal to the patella, suspending the lower leg and allowing for approximately 30-45 degrees of knee flexion. This slight flexion relaxes the posterior soft tissues and makes the popliteal fossa more accessible.
- Ankle Support: The foot and ankle are usually supported with additional padding or allowed to hang free over the end of the table.
- Padding: Ensure all pressure points (knees, shins, dorsum of feet, iliac crests, shoulders, face) are well-padded.
- Tourniquet: A pneumatic tourniquet is typically applied high on the thigh. While not strictly mandatory for all posterior knee procedures (some vascular surgeons prefer not to use it for PAES), it provides a bloodless field, significantly aiding visualization and meticulous dissection, particularly around the neurovascular bundle.
-
Sterile Preparation and Draping:
- The entire lower extremity, from the iliac crest to the toes, is prepared with an antiseptic solution.
- Sterile draping isolates the operative limb, allowing for free manipulation of the knee joint. A sterile stockinette and impervious drapes are utilized.
- Ensure adequate space for the surgeon and assistants.
Patient positioned prone with appropriate bolsters and knee flexion for posterior approach.
Detailed Surgical Approach / Technique
The posterior approach to the knee demands meticulous dissection, precise anatomical identification, and careful handling of neurovascular structures. The following describes a generalized technique, with specific variations for common pathologies.
1. Incision
The standard incision for the posterior approach to the knee is a gentle transverse S-shaped or inverted lazy-S incision in the popliteal fossa.
- Rationale: This curved incision typically follows Langer's lines of cleavage more closely than a straight longitudinal incision, especially in the medial and lateral aspects, potentially resulting in a more cosmetically acceptable scar. Crucially, its orientation, nearly parallel to the major flexion crease at the back of the knee, minimizes the risk of post-operative flexion contracture, which can be a significant concern with straight longitudinal incisions in this mobile region.
- Location: Centered over the popliteal crease, extending approximately 5-7 cm medially and laterally. The exact length and curvature may vary based on the required exposure and patient's anatomy.
- Alternatives: A straight longitudinal incision can be used, particularly for vascular procedures or when extensive longitudinal exposure is needed, but carries a higher risk of scar contracture. A posteromedial incision may be favored for specific pathologies like posterior horn medial meniscus root repairs or medial PCL avulsions.

Marking of the skin incision in the popliteal fossa.
2. Superficial Dissection
- Skin Incision: Incise the skin with a scalpel.
-
Subcutaneous Tissue:
Continue dissection through the subcutaneous fat. Identify and ligate or coagulate any superficial veins (e.g., small saphenous vein tributaries). Be aware of superficial nerves:
- Posterior Femoral Cutaneous Nerve: Supplies sensation to the posterior thigh and popliteal fossa, usually superior to the incision.
- Sural Nerve: Formed by contributions from the tibial and common fibular nerves, it descends superficially in the midline of the calf and crosses the popliteal fossa superficially. Identify and protect it, retracting it to minimize traction injury.
- Popliteal Fascia: The fatty layer is carefully dissected to expose the underlying popliteal fascia. This dense fascial layer forms the roof of the popliteal fossa.

Initial skin incision and subcutaneous dissection, exposing the popliteal fascia.
3. Deep Dissection & Neurovascular Identification
This is the most critical stage. The popliteal fascia is incised longitudinally, typically slightly lateral to the midline, carefully avoiding underlying structures.
-
Neurovascular Bundle Identification:
Once the fascia is opened, the key neurovascular structures must be identified in a consistent order, often described as the "NV Triad" from superficial to deep:
Nerve, Vein, Artery.
- Tibial Nerve: This is usually the first structure encountered, lying most superficially, often just deep to the popliteal fascia. It is typically the largest and most readily identifiable, appearing as a thick, whitish cord. It runs relatively centrally within the fossa. The nerve is mobilized and carefully retracted, typically medially or laterally depending on the target pathology and desired exposure.
- Popliteal Vein: Lies anterior (deep) to the tibial nerve. It is thinner-walled and typically more mobile than the artery. Multiple tributaries often drain into the popliteal vein, requiring careful ligation or coagulation.
- Popliteal Artery: The deepest of the three, lying directly on the floor of the fossa. It is thick-walled and pulsatile.

Identification and careful isolation of the tibial nerve.

Deeper dissection revealing the popliteal vein and artery.
- Common Fibular (Peroneal) Nerve: Located more laterally, often running along the medial border of the biceps femoris tendon. It branches off the sciatic nerve in the upper popliteal fossa. It should also be identified and protected, as it is vulnerable during lateral retraction.
-
Muscle Retraction:
- The medial and lateral heads of the gastrocnemius muscles form the inferior boundaries. They must be carefully retracted. For most posterior approaches, the primary interval is between the semimembranosus/semitendinosus medially and the medial head of the gastrocnemius.
- The plantaris tendon, if present, is a thin, shiny cord often found between the lateral gastrocnemius head and soleus, usually harmlessly sectioned or preserved.

Retraction of the medial head of the gastrocnemius to expose deeper structures.
4. Exposure of the Posterior Knee Capsule and Deeper Structures
With the neurovascular bundle safely retracted (typically medially with the tibial nerve, laterally with the common fibular nerve), and the gastrocnemius heads retracted, the posterior knee capsule comes into view.
- Popliteus Muscle: This muscle forms part of the floor of the fossa and originates from the lateral femoral condyle, inserting on the posterior aspect of the tibia. Its tendon runs obliquely deep to the lateral collateral ligament.
- Oblique Popliteal Ligament and Arcuate Complex: These capsular reinforcements are identifiable.
- Capsulotomy: A posterior capsulotomy is performed to gain access to the joint. The orientation of this incision depends on the target pathology. For PCL repairs/reconstructions, a transverse or inverted U-shaped incision in the posterior capsule is often made, carefully avoiding the popliteus tendon (laterally) and hamstring insertions (medially).

Exposure of the posterior knee capsule.

Incision of the posterior knee capsule to gain intra-articular access.
5. Specific Surgical Maneuvers
A. PCL Tibial Avulsion Fracture Fixation
- Exposure: Retract the medial gastrocnemius and neurovascular bundle medially. The posterior capsule is incised to expose the posterior intercondylar area of the tibia.
- Reduction: The avulsed PCL fragment is carefully reduced to its anatomical position using bone hooks, reduction clamps, or sutures. The knee may be flexed to relax the PCL during reduction.
-
Fixation:
- Screws: Small fragment screws (e.g., 3.5mm cortical or cannulated screws) are commonly used, placed from posterior to anterior, ensuring good purchase and avoiding intra-articular prominence.
- Suture Anchors: May be used if the fragment is too small or comminuted for screw fixation, allowing reattachment of the ligamentous tissue.
- Transtibial Sutures: Non-absorbable sutures are passed through the ligamentous portion of the fragment, then through drilled tunnels from anterior to posterior in the tibia, and tied over a button on the anterior tibia.

Reduction of a PCL tibial avulsion fragment.

Fixation of the avulsion fragment with screws or suture anchors.
B. PCL Reconstruction (Tibial Inlay Technique)
- Exposure: Similar to avulsion fixation, but exposure of the posterior tibia is often more extensive. The medial gastrocnemius may need partial release for better visualization.
- Graft Preparation: Autograft (e.g., hamstring, quadriceps) or allograft is prepared.
- Tibial Trough/Tunnel Creation: A trough is created on the posterior tibia at the PCL insertion site, or a single tunnel is drilled from posterior to anterior. This technique avoids the acute turn of a transtibial tunnel, which can lead to graft abrasion and failure.
- Femoral Tunnel: A femoral tunnel is typically drilled arthroscopically or through a separate anteromedial incision.
- Graft Passage and Fixation: The graft is passed through the femoral tunnel and then seated securely into the posterior tibial trough or passed through the posterior tibial tunnel. Fixation is achieved with screws, staples, or suture fixation.

Creation of a tibial trough for PCL inlay reconstruction.
C. Posterior Horn Meniscal Root Repair
- Exposure: Access is gained via a posteromedial capsulotomy, usually between the semimembranosus tendon and the medial head of the gastrocnemius.
- Visualization: The posterior horn of the meniscus, particularly the medial meniscus root, is identified. The tear is debrided if necessary.
- Repair: Suture anchors are placed into the tibial bone near the anatomical root attachment. Non-absorbable sutures are passed through the meniscal root tissue and then tied down to the anchors, securing the meniscus back to bone. Alternatively, transtibial pull-out sutures can be used, passed through anterior tibial tunnels and tied over a button.

Direct repair of a posterior horn meniscal root tear using suture anchors.
D. Popliteal Cyst Excision
- Exposure: Dissect through the popliteal fascia. The cyst is typically found superficial to the neurovascular bundle, often protruding between the medial head of the gastrocnemius and the semimembranosus.
- Identification of Stalk: Carefully dissect the cyst circumferentially, identifying its neck or stalk, which usually communicates with the knee joint through a defect in the posteromedial capsule.
- Excision: The cyst is excised, and the capsular defect at its origin is repaired if possible, or imbricated, to reduce recurrence. Care must be taken to ensure complete excision and meticulous hemostasis.

Excision of a popliteal (Baker's) cyst, with identification of its communication stalk.
6. Internervous Planes
The posterior approach utilizes specific internervous planes to minimize muscle damage and optimize exposure. The primary plane for deeper access is typically between the medial head of the gastrocnemius and the semimembranosus tendon for posteromedial pathologies, or between the lateral head of the gastrocnemius and the biceps femoris tendon for posterolateral pathologies. The neurovascular bundle itself lies within the deep fascia of the popliteal fossa, requiring careful isolation and retraction rather than utilizing a distinct internervous plane within the bundle itself. Careful blunt dissection along fascial planes is key.
7. Closure
- Hemostasis: Achieve meticulous hemostasis to prevent hematoma formation, which can compress neurovascular structures.
- Drainage: A suction drain (e.g., a 1/4-inch Hemovac) may be placed deep to the popliteal fascia, particularly if extensive dissection was performed or significant bleeding is anticipated.
- Capsular Closure: The posterior knee capsule is repaired with absorbable sutures if an incision was made.
- Fascial Closure: The popliteal fascia is closed with absorbable sutures.
- Subcutaneous Tissue: The subcutaneous layer is closed to reduce dead space.
- Skin Closure: The skin is closed with staples or non-absorbable sutures.
- Dressing: A sterile dressing is applied.
- Post-operative Brace: A hinged knee brace may be applied, depending on the procedure (e.g., PCL repair/reconstruction).
Layered closure of the wound, including capsular and fascial repair.
Complications & Management
Despite meticulous technique, the posterior approach to the knee carries inherent risks due to the critical neurovascular structures within the popliteal fossa. Awareness of potential complications and strategies for prevention and management is paramount.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approximate) | Prevention Strategies | Salvage Strategies |
|---|---|---|---|
| Vascular Injury | 0.1-1.0% | Meticulous dissection, clear identification (NV triad), blunt dissection, tourniquet use (if appropriate). | Immediate vascular surgery consultation, primary repair, vein graft. |
| Neurological Injury | 1-5% (Tibial/Peroneal) | Clear identification, gentle retraction, avoid electrocautery near nerves, careful use of sharp instruments. | Observation for neuropraxia, neurolysis, nerve repair/graft if transection. |
| Infection | 1-3% (Superficial/Deep) | Strict aseptic technique, prophylactic antibiotics, thorough wound irrigation, meticulous closure. | IV antibiotics, surgical debridement, washout, hardware removal (if deep). |
| Hematoma/Seroma | 2-5% | Meticulous hemostasis, judicious drain placement, compression dressing. | Aspiration, re-exploration for drainage and source control. |
| Knee Stiffness/Arthrofibrosis | 5-10% | Early controlled range of motion (ROM), diligent physical therapy, tension-free capsular closure. | Manipulation under anesthesia, arthroscopic or open arthrolysis. |
| Wound Healing Issues | 3-7% (Dehiscence, necrosis) | Atraumatic tissue handling, tension-free skin closure, avoid excessive skin retraction, careful incision planning. | Local wound care, debridement, flap coverage for severe cases. |
| Recurrence (e.g., Baker's Cyst) | 10-20% for cysts | Complete cyst excision, repair of capsular defect, address underlying intra-articular pathology. | Re-excision, management of underlying pathology. |
| DVT/Pulmonary Embolism (PE) | <1% (with prophylaxis) | Pharmacological and mechanical DVT prophylaxis, early mobilization. | Anticoagulation, inferior vena cava filter. |
| Compartment Syndrome | Rare | Monitor for post-operative pain, swelling, neurovascular compromise. | Emergent fasciotomy. |
Specific Complications and Management Details
-
Vascular Injury (Popliteal Artery/Vein):
The most catastrophic complication. Injury to the popliteal artery can lead to limb ischemia and potential amputation if not recognized and treated promptly.
- Prevention: The artery is the deepest structure, lying on the bone. Always dissect in the "NV triad" sequence. Use blunt dissection and gentle retraction. Maintain a bloodless field with a tourniquet.
- Management: If injury occurs, immediately release the tourniquet, apply direct pressure, and notify a vascular surgeon. Repair typically involves primary anastomosis or interposition vein grafting.
-
Neurological Injury (Tibial Nerve, Common Fibular Nerve, Sural Nerve):
- Prevention: Identify and isolate these nerves early. Use vessel loops for gentle retraction. Avoid prolonged or excessive traction, direct trauma from instruments, or thermal injury from electrocautery.
- Management: For neuropraxia (transient loss of function), observation is often sufficient, as recovery can occur over weeks to months. For neurapraxia that does not resolve or suspected neurotmesis (nerve transection), early referral to a peripheral nerve specialist for neurolysis or surgical repair is indicated.
- Infection: Superficial infections respond to oral antibiotics and local wound care. Deep infections (periprosthetic or intra-articular) require aggressive surgical debridement, intravenous antibiotics, and potentially hardware removal.
- Knee Stiffness/Arthrofibrosis: Common after significant knee trauma or surgery. Early, controlled range of motion exercises as tolerated and prescribed by rehabilitation protocols are crucial. If severe, manipulation under anesthesia or arthroscopic/open lysis of adhesions may be necessary.
- Wound Healing Issues: The posterior knee skin can be prone to poor healing due to tension and blood supply. Careful skin handling, tension-free closure, and avoiding excessive cautery are important. If necrosis or dehiscence occurs, local wound care, debridement, and potentially plastic surgery consultation for flap coverage may be required.

Example of a healed surgical incision, demonstrating adequate cosmetic outcome and minimal contracture.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following a posterior knee approach is highly dependent on the specific procedure performed, the stability achieved during surgery, and the patient's individual healing capacity. The overriding goals are to protect the repair/reconstruction, restore range of motion, regain strength, and facilitate a safe return to function.
General Principles
- Pain Management: Multimodal analgesia (oral medications, regional blocks, cryotherapy) is essential to facilitate early mobilization.
- Wound Care: Maintain a clean, dry dressing. Monitor for signs of infection or wound healing issues. Suture/staple removal typically at 10-14 days.
- DVT Prophylaxis: Standard orthopedic guidelines for pharmacological and mechanical prophylaxis.
- Early Mobilization: As tolerated, to prevent stiffness and DVT. However, specific weight-bearing and range-of-motion (ROM) restrictions are crucial to protect repairs.
Procedure-Specific Protocols
1. PCL Repair/Reconstruction (e.g., Tibial Inlay)
The PCL is load-bearing in flexion, thus rehabilitation focuses on minimizing posterior tibial sag.
-
Phase I: Protection (Weeks 0-6)
- Weight-Bearing: Non-weight-bearing or partial weight-bearing with crutches.
- Bracing: A hinged knee brace locked in extension or slight flexion (e.g., 0-30 degrees) for ambulation to prevent posterior sag.
- Range of Motion: Passive ROM initially, with caution. Avoid isolated hamstring contraction and open-chain resisted knee flexion beyond 70 degrees for 3-4 months. Focus on gentle knee extension. Some protocols advocate for a "prone hang" to promote extension.
- Exercises: Quadriceps setting, ankle pumps, hip abduction/adduction exercises.

Patient in a hinged knee brace, locked in extension, for protection post-PCL surgery.
-
Phase II: Controlled Motion & Early Strengthening (Weeks 6-12)
- Weight-Bearing: Progress to full weight-bearing as tolerated with brace.
- Bracing: Continue brace for ambulation, may unlock for controlled ROM.
- Range of Motion: Gradual increase in active and passive flexion and extension. Aim for full extension.
- Exercises: Closed-chain quadriceps strengthening (e.g., mini-squats, leg press with limited flexion), core stability, light hip exercises. Avoid deep squats or hamstring-dominant exercises.
-
Phase III: Advanced Strengthening & Proprioception (Months 3-6)
- Bracing: Discontinue brace when adequate quadriceps control is achieved and gait is normalized.
- Range of Motion: Achieve full, pain-free ROM.
- Exercises: Progress closed-chain strengthening, introduce light proprioceptive drills (balance board, single-leg stance), elliptical, swimming. Gradually introduce hamstring strengthening with caution.
-
Phase IV: Return to Activity (Months 6-12+)
- Criteria: Full, pain-free ROM, symmetrical strength (>90% compared to contralateral limb), excellent proprioception, and no effusion.
- Activities: Gradual return to sports-specific drills, running, jumping. Contact sports typically not before 9-12 months.
2. Posterior Horn Meniscal Root Repair
- Weight-Bearing: Non-weight-bearing or partial weight-bearing for 4-6 weeks to protect the repair. Crutches are used.
- Bracing: Hinged knee brace locked in extension for ambulation.
- Range of Motion: Restricted flexion (e.g., 0-90 degrees) for 4-6 weeks to prevent excessive hoop stress on the repair. Gradual progression thereafter.
- Exercises: Quadriceps setting, ankle pumps, hip strengthening. Avoid deep flexion, squatting, or twisting motions for several months.
- Progression: Similar to PCL, with careful increase in ROM and weight-bearing, followed by progressive strengthening and return to activity over 6-9 months.
3. Popliteal Cyst Excision
- Weight-Bearing: Full weight-bearing as tolerated immediately post-op, unless there are other concomitant procedures.
- Bracing: Not typically required.
- Range of Motion: Early, gentle active and passive ROM. Avoid forced knee flexion/extension in the immediate post-operative period if the capsular repair is tight.
- Exercises: Quadriceps strengthening, hamstring stretching, gentle cycling. Focus on restoring full motion quickly. Return to full activity is generally faster, often within 4-6 weeks, provided there are no complications.
4. Posterior Osteophyte Excision / Posterior Capsular Release
- Weight-Bearing: Full weight-bearing as tolerated.
- Bracing: Not typically required unless there is significant instability or risk of re-contracture.
- Range of Motion: Aggressive ROM exercises, particularly targeting extension for capsular release. Continuous passive motion (CPM) machine may be utilized.
- Exercises: Focus on restoring full knee flexion and extension, then progressive strengthening.
Importance of Physical Therapy: Close collaboration with a physical therapist specializing in orthopedic rehabilitation is crucial for guiding patients through these protocols, ensuring proper technique, and modifying plans based on individual progress and surgeon's directives.
Summary of Key Literature / Guidelines
The literature on posterior knee approaches and popliteal fossa pathologies emphasizes anatomical precision, judicious patient selection, and tailored rehabilitation. While advancements in arthroscopy have reduced the need for open approaches for some conditions, a thorough understanding of the posterior approach remains indispensable for specific indications.
PCL Reconstruction
- Tibial Inlay vs. Transtibial: The posterior approach for tibial inlay PCL reconstruction is supported by literature as a biomechanically sound technique. Studies by Bergfeld et al. and Race and Sachs highlighted concerns with the acute angle and potential for graft abrasion with transtibial tunnel techniques, advocating for the inlay approach to minimize these issues. While some contemporary arthroscopic techniques have attempted to mitigate these concerns with alternative tibial tunnel placements or guidewire configurations, the open inlay still provides direct, anatomical fixation.
- Combined Injuries: PCL injuries frequently occur in multi-ligamentous trauma. Fanelli et al. and Shelbourne et al. have contributed significantly to understanding the diagnosis and management of these complex knee dislocations, often necessitating combined approaches and careful sequencing of repairs.
- Outcomes: Long-term outcomes for PCL reconstruction are generally positive, with improvements in stability and function, but often do not fully restore baseline activity levels, especially in high-grade or chronic injuries. Persistent mild posterior laxity is not uncommon.
Posterior Meniscal Root Repairs
- Importance: Studies by LaPrade et al. and Keyes et al. have underscored the critical role of meniscal root attachments in maintaining hoop stress and preventing extrusion. Unrepaired root tears are biomechanically equivalent to total meniscectomy, leading to accelerated osteoarthritis.
- Technique: Both arthroscopic and open techniques exist. The posterior approach offers direct visualization and secure suture anchor or transtibial pull-out repair, particularly for complex or large posterior root tears. Evidence suggests that repair of meniscal root tears can restore knee kinematics and reduce progression to osteoarthritis.
Popliteal Cysts
- Etiology and Recurrence: Baker's original description and subsequent studies have confirmed the communication of symptomatic popliteal cysts with the knee joint, often secondary to underlying intra-articular pathology (e.g., meniscal tear, osteoarthritis). Surgical excision addresses the cyst but recurrence rates, ranging from 10-20%, highlight the importance of addressing the underlying intra-articular cause if present.
- Surgical vs. Non-Surgical: Current guidelines, such as those by the American Academy of Orthopaedic Surgeons (AAOS) , generally recommend conservative management initially. Surgical excision is reserved for large, refractory, or symptomatic cysts, with outcomes generally favorable for symptom relief.
Popliteal Artery Entrapment Syndrome (PAES)
- Diagnosis and Management: PAES is a rare but critical cause of exertional leg pain or claudication in young, active individuals. Rich et al. and other vascular surgery literature emphasize early diagnosis through dynamic vascular studies and surgical decompression. The posterior approach is essential for direct visualization and release of the entrapping structures (e.g., aberrant gastrocnemius heads or fibrous bands). Untreated PAES can lead to arterial damage, thrombosis, and chronic limb ischemia.
Overall Principles
- Anatomical Mastery: The consistent theme across all literature pertaining to the posterior knee is the absolute necessity of mastering the three-dimensional anatomy of the popliteal fossa. The close confines and critical structures necessitate careful and deliberate dissection.
- Neurovascular Protection: Techniques to identify and protect the tibial nerve, common fibular nerve, popliteal artery, and vein are paramount.
- Personalized Approach: While general guidelines exist, the optimal surgical strategy and rehabilitation protocol must be individualized based on the specific pathology, patient factors, and intraoperative findings.
- Evolving Techniques: Continuous advancements in arthroscopic techniques allow for less invasive management of some posterior knee pathologies. However, open posterior approaches remain a vital tool in the orthopedic surgeon's armamentarium for complex or challenging cases.

Cadaveric dissection highlighting the critical neurovascular structures and their relationship to bony and muscular landmarks.
Clinical & Radiographic Imaging



You Might Also Like