Unlock Surgical Precision: Anatomy of the Lateral Knee
Key Takeaway
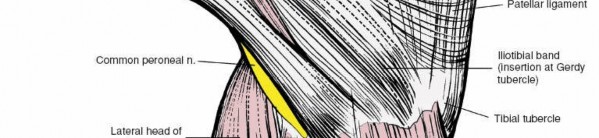
Discover the latest medical recommendations for Unlock Surgical Precision: Anatomy of the Lateral Knee. The anatomy of the lateral side of the knee consists of three layers of supporting structures. The outer layer includes the iliotibial band, biceps femoris muscle, and lateral patellar retinaculum. The middle layer features the superficial lateral ligament (fibular collateral ligament) and the recently described anterolateral ligament. A clear understanding of these structures' normal anatomy is crucial for surgical contexts.
Unlock Surgical Precision: Anatomy of the Lateral Knee
Introduction & Epidemiology
The lateral compartment of the knee is a complex anatomical region critical for knee stability, kinematics, and overall function. Injuries to the lateral structures, particularly the posterolateral corner (PLC), represent a significant clinical challenge due to the intricate interplay of static and dynamic stabilizers. These injuries are often misdiagnosed or undertreated, leading to chronic instability, accelerated degenerative changes, and functional impairment. A profound understanding of the nuanced anatomy and biomechanics of the lateral knee is paramount for accurate diagnosis, meticulous surgical planning, and successful outcomes.
Epidemiologically, isolated lateral knee ligament injuries are less common than medial-sided injuries, but they frequently occur in conjunction with anterior cruciate ligament (ACL) tears, posterior cruciate ligament (PCL) tears, or multiligamentous knee dislocations. The reported incidence of PLC injury accompanying ACL rupture ranges from 10% to 28%, with some studies suggesting even higher rates in specific athletic populations. Such combined injuries are associated with significantly worse outcomes if the PLC pathology is not addressed. Mechanisms of injury typically involve a varus stress, often combined with external rotation or hyperextension, commonly seen in contact sports, skiing accidents, and motor vehicle trauma. The diagnostic challenge stems from the subtlety of physical exam findings in acute settings and the potential for occult injury on standard imaging. Therefore, a comprehensive knowledge base is essential for all orthopedic surgeons, residents, and medical students managing knee pathology.
Surgical Anatomy & Biomechanics
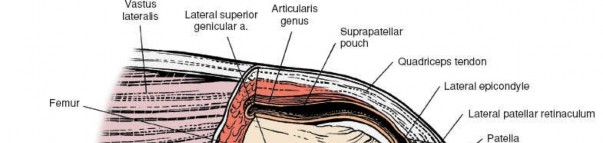
The supporting structures on the lateral side of the knee are conventionally described in three distinct layers, from superficial to deep. This layered understanding is critical for surgical dissection and reconstruction, as pathologic states can significantly distort normal anatomical relationships. A clear understanding of the normal anatomy is required before explorations are carried out.
Layer I: The Outer Layer
The most superficial layer comprises the iliotibial band (ITB) and its associated fascial extensions.
-
Iliotibial Band (ITB):
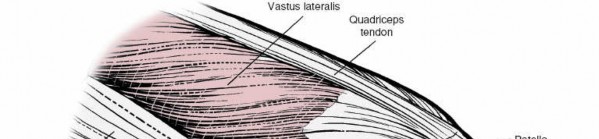
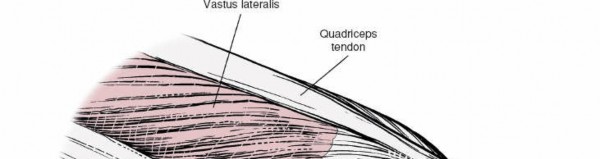
This robust, longitudinal aponeurotic band is a thickening of the deep fascia of the thigh. Proximally, it receives fibers from the tensor fascia latae and the gluteus maximus muscles. Its fibers run longitudinally along the lateral thigh. Distally, the ITB inserts into a smooth facet on the anterior surface of the lateral condyle of the tibia, known as
Gerdy tubercle
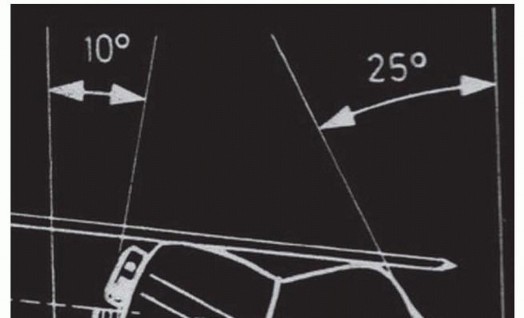
. It also sends fibers into the deep fascia of the leg and reinforces the lateral patellar retinaculum. In injuries to the knee involving severe varus stress, its insertion may be avulsed. Biomechanically, the ITB plays a dynamic role; when the knee is in extension, it is anterior to the axis of rotation and functions as an extensor. With the knee flexed to 90 degrees, it moves behind the axis of rotation and acts as a flexor. This variable relationship to the axis of rotation may be a feature in the genesis of the pivot shift test for a torn anterior cruciate ligament.

Layer II: The Middle Layer
Deep to the ITB lies Layer II, consisting primarily of the fibular collateral ligament (FCL), the lateral patellar retinaculum, and components of the posterolateral capsule.
-
Fibular Collateral Ligament (FCL):
This is a cord-like, extra-articular ligament originating from the lateral femoral epicondyle, proximal to the popliteus tendon origin. It courses distally and slightly posteriorly to insert onto the lateral aspect of the fibular head. The FCL is the primary static stabilizer against varus stress throughout the knee's range of motion and also acts as a secondary restraint to external rotation. Its distinct cord-like nature allows it to be palpated and distinguished from the broad, flat medial collateral ligament. The common peroneal nerve courses posterior to the FCL, making it vulnerable during surgical exposure.

- Lateral Patellar Retinaculum: This fibrous expansion connects the ITB to the patella and provides stability to the patellofemoral joint, influencing patellar tracking.
-
Biceps Femoris Tendon:
The long head of the biceps femoris inserts into the fibular head, often splitting to envelop the FCL insertion. The short head inserts directly onto the lateral tibia. Its complex insertion contributes to posterolateral stability and acts as a dynamic external rotator and flexor of the knee.

Layer III: The Deep Layer (Posterolateral Corner - PLC)
The deepest layer is the most complex and includes the lateral capsule, popliteus muscle-tendon unit, and the arcuate ligament complex, which collectively form the posterolateral corner (PLC). This layer is crucial for resisting external rotation, varus stress, and posterior tibial translation.
-
Popliteus Muscle-Tendon Unit:
The popliteus tendon originates from a sulcus on the lateral femoral epicondyle, distal and anterior to the FCL origin. It courses obliquely, traversing the posterolateral aspect of the knee joint. The muscle belly originates from the posterior tibia. This unit is a key dynamic stabilizer of the PLC, acting as an internal rotator of the tibia on the femur (unlocking the knee) and a flexor. It also provides significant static restraint to external rotation through its tendinous attachments.


-
Arcuate Ligament Complex:
This is a confluence of ligamentous structures reinforcing the posterolateral capsule. It includes:
- Popliteofibular Ligament (PFL): This strong ligament connects the popliteus tendon to the fibular styloid. It is considered the primary static stabilizer of the PLC against external rotation and posterior tibial translation, particularly in conjunction with the FCL.
- Arcuate Ligament Proper: This Y-shaped structure has medial and lateral limbs that extend from the fibular styloid to the posterior joint capsule and popliteus muscle.
- Fabellofibular Ligament: Present in cases where a fabella (sesamoid bone in the lateral gastrocnemius tendon) exists, connecting it to the fibular head.
-
Posterolateral Capsule:
This broad capsular structure is reinforced by the aforementioned ligaments.



- Lateral Meniscus: The lateral meniscus is uniquely more mobile than its medial counterpart due to fewer peripheral attachments and the presence of the meniscopopliteal fascicles, which allow the popliteus tendon to pass through the capsule, creating a hiatus. This mobility can protect it from some compressive forces but also predisposes it to tears, especially root tears or ramp lesions. It attaches to the tibia via meniscotibial ligaments and sometimes to the femur via meniscofemoral ligaments (ligaments of Wrisberg and Humphry), which pass posterior and anterior to the PCL, respectively.
Associated Structures
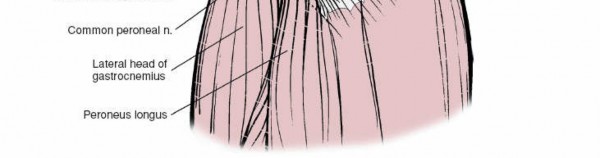
- Common Peroneal Nerve: This nerve, a branch of the sciatic nerve, courses superficially to the lateral head of the gastrocnemius and then winds around the fibular neck. It is exquisitely vulnerable during surgical approaches to the lateral knee, particularly during fibular head fixation or tunnel drilling. Meticulous identification and protection are non-negotiable.
The complex interplay of these structures provides both static and dynamic stability to the lateral knee. The FCL and PFL are the primary static restraints to varus and external rotation, respectively. The popliteus muscle-tendon unit and the biceps femoris provide dynamic stability. Varus instability is primarily resisted by the FCL. External rotation instability, particularly at 30° of knee flexion, is a hallmark of PLC injury, involving the PFL, popliteus tendon, and posterolateral capsule. Combined varus and external rotation instability is indicative of a more extensive PLC disruption.
Indications & Contraindications
The decision-making process for intervention in lateral knee pathology requires careful consideration of the specific injury pattern, chronicity, patient's functional demands, and overall medical status.
Operative Indications
- Acute High-Grade FCL/PLC Injuries: Grade III FCL tears, isolated or combined with other ligamentous injuries (e.g., ACL, PCL), especially those with fibular head avulsions or significant instability on examination/stress radiographs.
- Chronic PLC Instability: Symptomatic chronic varus or posterolateral rotational instability despite non-operative management, leading to recurrent giving-way episodes, pain, or functional limitations. Often coexists with chronic ACL/PCL deficiency.
- Lateral Meniscus Tears: Symptomatic tears (e.g., bucket-handle, radial, root tears) amenable to repair, or unstable complex tears requiring partial meniscectomy, particularly in younger, active patients.
- Osteochondral Lesions: Symptomatic lesions of the lateral femoral condyle or tibial plateau.
- ITB Pathology: Recalcitrant ITB friction syndrome unresponsive to extensive non-operative management, requiring surgical release or debridement. Avulsion of the ITB insertion.
- Proximal Tibial Osteotomy: For symptomatic varus malalignment, often in conjunction with lateral compartment unloader bracing or as a prelude to unicompartmental or total knee arthroplasty.
- Tibial Plateau Fractures: Lateral compartment involvement requiring open reduction and internal fixation (ORIF).
- Patellofemoral Instability: Cases of lateral patellar instability requiring lateral retinacular release or realignment procedures.
Non-Operative Indications
- Low-Grade FCL/PLC Sprains (Grade I/II): Stable injuries with minimal laxity, managed with RICE, bracing, physical therapy focusing on strengthening and proprioception.
- Acute ITB Friction Syndrome: Initial management typically involves activity modification, NSAIDs, physical therapy (stretching, strengthening of hip abductors/core), corticosteroid injections.
- Asymptomatic Lateral Meniscus Tears: Incidental findings on imaging without mechanical symptoms (locking, catching, pain).
- Mild Osteoarthritis of the Lateral Compartment: Managed with conservative measures like activity modification, NSAIDs, injections, and bracing.
Contraindications
-
Absolute Contraindications:
- Active local or systemic infection.
- Profound systemic illness precluding safe anesthesia and surgery.
- Severe peripheral vascular disease compromising wound healing.
-
Relative Contraindications:
- Severe generalized osteoarthritis of the knee (may warrant arthroplasty instead of isolated ligamentous reconstruction).
- Unrealistic patient expectations or non-compliance with post-operative rehabilitation.
- Inadequate soft tissue envelope or prior extensive scarring.
Table: Operative vs. Non-Operative Indications for Lateral Knee Pathology
| Pathology | Operative Indications | Non-Operative Indications |
|---|---|---|
| Fibular Collateral Ligament (FCL) | Acute Grade III tears, fibular head avulsions, chronic symptomatic varus instability, combined multiligamentous injuries requiring reconstruction/repair. | Grade I/II sprains, stable on stress testing, minimal laxity, managed with bracing, physical therapy, activity modification. |
| Posterolateral Corner (PLC) | Acute Grade III injuries (PFL, popliteus), chronic symptomatic posterolateral rotational instability, combined PLC-ACL/PCL tears. Surgical repair for acute avulsions, reconstruction for mid-substance tears or chronic instability. | Grade I/II sprains, stable on stress testing, minimal laxity, managed with bracing, physical therapy, activity modification. |
| Lateral Meniscus | Symptomatic tears (e.g., bucket-handle, radial, root tears) amenable to repair, unstable flap tears causing mechanical symptoms, persistent effusion, or pain. | Asymptomatic tears, stable peripheral tears in avascular zones, degenerative tears in older patients without mechanical symptoms, small stable tears responsive to conservative management. |
| Iliotibial Band (ITB) | Recalcitrant ITB friction syndrome unresponsive to >6 months of conservative treatment, symptomatic ITB avulsion injuries. | Acute ITB friction syndrome (rest, ice, NSAIDs, stretching, strengthening of hip abductors, core stability, corticosteroid injections). |
| Osteochondral/Articular Cartilage | Symptomatic, unstable lesions, focal defects in active patients (microfracture, OATs, MACI), larger defects requiring allograft or osteotomy for unicompartmental overload. | Small, asymptomatic, or stable lesions, mild pain responsive to conservative measures (NSAIDs, activity modification, injections), advanced osteoarthritis (often managed non-operatively until arthroplasty indicated). |
| Patellofemoral Instability | Recurrent symptomatic lateral patellar dislocations/subluxations, failed conservative management, significant anatomical predisposing factors (trochlear dysplasia, patella alta, increased TT-TG distance) in need of surgical realignment (e.g., MPFL reconstruction, lateral release, tibial tubercle osteotomy). | First-time dislocation without significant risk factors, stable subluxation, mild symptoms responsive to physical therapy (quadriceps strengthening, VMO retraining, hip abductor strengthening), bracing. |
| Tibial Plateau Fractures (Lateral) | Displaced or unstable fractures involving the articular surface, requiring anatomical reduction and stable internal fixation to restore joint congruity and alignment. | Stable, non-displaced fractures, typically managed with bracing, protected weight-bearing, and close radiographic follow-up. |
| Varus Malalignment/Osteoarthritis | Symptomatic varus malalignment with focal lateral compartment arthritis in younger, active patients, unresponsive to conservative care, requiring high tibial osteotomy to shift weight-bearing axis. | Mild-moderate varus osteoarthritis with intermittent symptoms, managed with NSAIDs, activity modification, injections, physical therapy, bracing. Severe osteoarthritis in older, less active patients often indicates arthroplasty. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical to optimize exposure, protect neurovascular structures, and ensure accurate surgical execution.
Pre-Operative Planning
- Clinical Assessment: A thorough history and physical examination, including specific stress tests for varus instability (varus stress test at 0° and 30° flexion), posterolateral rotational instability (dial test at 30° and 90° flexion), and the pivot shift test, are paramount.
-
Imaging:
- Radiographs: Standard AP, lateral, and Merchant views. Stress radiographs (telos or manual) are invaluable for quantifying varus and posterolateral gapping. Long-leg alignment views are crucial for assessing overall limb alignment, especially if an osteotomy is contemplated.
- MRI: The gold standard for assessing soft tissue injuries (ligaments, tendons, menisci, capsule). Specific sequences can delineate FCL, popliteus tendon, PFL, and meniscocapsular lesions.
- CT: Useful for assessing bony avulsions (e.g., fibular head, Gerdy tubercle), occult fractures, and pre-operative planning for osteotomies (e.g., 3D reconstruction for accurate cut placement).
- Graft Selection (for reconstructions): Autograft options include semitendinosus/gracilis, quadriceps tendon, or tibialis anterior tendon. Allografts (e.g., Achilles, tibialis anterior, semitendinosus) are also commonly used, especially in multiligamentous injuries or revisions. The choice depends on surgeon preference, patient factors, and the specific structures being reconstructed.
- Hardware Templating: Pre-operative templating using radiographs or CT scans assists in determining appropriate implant sizes (screws, tunnels, plates) and ensuring accurate anatomical placement.
Patient Positioning
The typical patient position for lateral knee surgery is supine , often with a bump under the ipsilateral hip to allow for easier access to the lateral aspect of the knee.
- Limb Preparation: A thigh tourniquet is applied as proximally as possible. The entire limb is prepped and draped to allow full range of motion of the hip, knee, and ankle, which is essential for intra-operative graft tensioning and assessment of stability.
- Leg Holder: A lateral post or leg holder can be utilized to maintain knee flexion and provide stability, though some surgeons prefer a freely movable limb for dynamic assessment.
-
Common Peroneal Nerve Protection:
This is perhaps the most critical aspect of positioning. The nerve courses around the fibular neck. Meticulous padding of the fibular head region is essential to prevent iatrogenic compression neuropathy.

- Arthroscopy Cart: If diagnostic or therapeutic arthroscopy is planned concurrently, the arthroscopy tower and instrument cart are positioned appropriately.
- Fluoroscopy: C-arm fluoroscopy may be required for precise tunnel placement or hardware fixation, and its position should be considered.
Detailed Surgical Approach / Technique
The surgical approach to the lateral knee is highly dependent on the specific pathology, but a common extensile approach allows access to all three layers and key structures of the posterolateral corner. This section outlines a general approach, emphasizing crucial dissection steps, internervous planes, and principles of reconstruction.
Incision and Superficial Dissection
- Skin Incision: A curvilinear or straight longitudinal incision is typically made over the lateral aspect of the knee, extending from the lateral femoral epicondyle distally towards the fibular head. For more extensive PLC reconstruction, a "hockey stick" incision curving posteriorly around the fibular head may be used.
- Subcutaneous Tissue: Dissect through the subcutaneous fat and superficial fascia. Identify and protect any superficial neurovascular structures.
-
Layer I Exposure (Iliotibial Band):
The ITB is the first robust structure encountered. Its fibers run longitudinally. The ITB may be incised longitudinally or elevated subperiosteally from Gerdy tubercle, depending on the need for exposure or if it is part of the pathology requiring reconstruction.
Identification and Protection of the Common Peroneal Nerve
This is the most critical step in the lateral knee approach.
- Location: The common peroneal nerve courses posterior to the biceps femoris tendon and wraps around the fibular neck.
- Dissection: Carefully dissect through the deep fascia posterior to the ITB and anterior to the biceps femoris. Blunt dissection can be used to isolate the nerve. Follow it distally around the fibular neck until its bifurcation into superficial and deep peroneal nerves.
- Protection: Once identified, the nerve is meticulously protected with a vessel loop or rubber drain, carefully retracted, and monitored throughout the procedure.
Layer II & III Dissection and Exposure
- Biceps Femoris Tendon: Retract the biceps femoris tendon posteriorly. The FCL lies deep to the long head of the biceps femoris.
- Fibular Head Exposure: The fibular head is a critical landmark. Identify the insertion of the FCL onto the fibular head.
-
Fibular Collateral Ligament (FCL) Exposure:
If the FCL is torn mid-substance, identify its femoral and fibular attachments. For reconstruction, the FCL origin on the lateral femoral epicondyle is identified, slightly posterior and proximal to the popliteus tendon origin.

-
Popliteus Tendon and Arcuate Complex Exposure:
- Carefully dissect deep to the FCL and posterior to the lateral femoral condyle to identify the popliteus tendon as it emerges from the popliteal hiatus. Its femoral origin is distal and anterior to the FCL origin.
-
The posterolateral capsule is deep to these structures. The arcuate ligament complex, including the popliteofibular ligament, reinforces this capsule. The PFL connects the popliteus tendon to the fibular styloid.


Reconstruction Principles (General)
The goal of PLC reconstruction is to restore native anatomy and biomechanics. Multiple techniques exist, but key principles include anatomical tunnel placement, appropriate graft tensioning, and robust fixation.
-
FCL Reconstruction:
- Femoral Tunnel: Typically placed at the isometric point on the lateral femoral epicondyle, slightly proximal and posterior to the popliteus origin.
- Fibular Tunnel: Placed at the anatomical FCL insertion on the fibular head.
- Graft Passage: The graft (e.g., autograft hamstring, allograft Achilles) is passed through these tunnels.
- Tensioning: The FCL graft is tensioned with the knee in approximately 20-30° of flexion and neutral rotation, followed by secure fixation (e.g., interference screw, post-and-washer).
-
Popliteofibular Ligament (PFL) Reconstruction:
- Often reconstructed as part of an overall PLC repair or reconstruction.
- Femoral Tunnel: Placed at the popliteus origin on the lateral femoral epicondyle, distinct from the FCL origin.
- Fibular Tunnel: Placed at the fibular styloid, where the PFL inserts.
- Graft Passage and Tensioning: The PFL graft (often a separate limb of a larger graft) is passed and tensioned in approximately 70-90° of flexion and neutral rotation or slight internal rotation, then fixed.
-
Combined PLC Reconstruction (e.g., Modified Larson Technique, Anatomical LaPrade Technique):
These techniques aim to reconstruct multiple PLC structures simultaneously, often using a single large graft (e.g., Achilles allograft) or multiple smaller grafts. The principle involves creating anatomical tunnels at the femoral FCL, femoral popliteus, fibular head, and fibular styloid sites. The grafts are then fixed in a sequential and specific manner to restore varus and rotational stability.

- Meniscus Repair: If lateral meniscal tears are present, repair techniques (e.g., all-inside, inside-out, outside-in sutures) are performed. Concomitant repair of the posterolateral capsule or popliteal hiatus may be necessary.
- Soft Tissue Closure: After reconstruction and stability assessment, the layers are closed anatomically. The ITB is repaired, followed by subcutaneous tissue and skin. A drain may be placed if significant bleeding is anticipated.
Internervous Planes
The key internervous planes for lateral knee approaches typically involve the interval between the ITB anteriorly and the biceps femoris/common peroneal nerve posteriorly. Further dissection involves carefully navigating around the common peroneal nerve and deep to the FCL to access the popliteus and posterolateral capsule. Understanding these planes is critical to minimize muscle damage and protect neural structures.
Complications & Management
Complications following lateral knee surgery, particularly for PLC reconstruction, can be significant due to the complex anatomy and high forces across the joint. Vigilant attention to detail and early recognition are crucial for effective management.
Common Complications
-
Common Peroneal Nerve Injury:
- Incidence: Varies widely, reported from 0.8% to over 30% in some series, especially in multiligamentous or revision surgeries. The risk is highest during exposure of the fibular head, tunnel drilling, or graft passage and tensioning.
- Presentation: Foot drop, paresthesia in the dorsum of the foot, or motor weakness of ankle dorsiflexion and eversion. Can be neurapraxia, axonotmesis, or neurotmesis.
-
Management:
- Intra-operative: If identified, immediately release compression, assess for nerve integrity. If lacerated, primary repair or grafting.
- Post-operative: If delayed onset or worsening, initiate observation, physical therapy, ankle-foot orthosis (AFO) for foot drop. If no improvement, EMG/NCS studies to assess severity. Consideration for nerve exploration, neurolysis, or repair/grafting at 3-6 months if no recovery. Tendon transfers (e.g., tibialis posterior to dorsum of foot) or fusion may be considered for permanent paralysis.
-
Stiffness/Arthrofibrosis:
- Incidence: Up to 20-30%, particularly in multiligamentous injuries or complex reconstructions.
- Presentation: Limited range of motion, often flexion contracture or loss of terminal extension.
- Management: Aggressive physical therapy, continuous passive motion (CPM). If conservative measures fail, manipulation under anesthesia (MUA) or arthroscopic/open arthrolysis may be necessary. Prevention is key through early, controlled range of motion.
-
Persistent Instability / Failed Reconstruction:
- Incidence: Can range from 5-15%, often higher in revision cases or if concomitant injuries (e.g., PCL) are not adequately addressed.
- Presentation: Recurrent varus gapping, posterolateral rotational instability, "giving way," pain.
- Management: Thorough diagnostic workup including stress radiographs and MRI to identify the cause of failure (e.g., graft laxity, non-anatomic tunnel placement, unrecognized concomitant injury, malalignment). Revision surgery with meticulous attention to anatomical reconstruction and possibly addressing underlying malalignment (e.g., osteotomy).
-
Infection:
- Incidence: Low (1-3%), but potentially devastating.
- Presentation: Pain, erythema, swelling, fever, purulent drainage.
- Management: Early detection. Superficial infections: oral antibiotics. Deep infections: surgical debridement, irrigation, retention or removal of hardware/grafts based on presentation and time to diagnosis, intravenous antibiotics.
-
Hardware-Related Issues:
- Incidence: Variable, depends on implant type.
- Presentation: Prominent hardware causing pain, soft tissue irritation, loosening, migration.
- Management: Symptomatic hardware may require removal after adequate healing of the reconstruction. Loose or migrated hardware may require early removal and potential revision.
-
Thromboembolic Events (DVT/PE):
- Incidence: Relatively low in isolated knee ligament surgery but increases significantly in multiligamentous injuries, prolonged immobilization, or patients with risk factors.
- Presentation: DVT: calf pain, swelling, tenderness. PE: dyspnea, chest pain, tachycardia.
- Management: Prophylaxis (mechanical/pharmacological). Diagnosis via ultrasound (DVT) or CT pulmonary angiography (PE). Treatment with anticoagulation.
-
Complex Regional Pain Syndrome (CRPS):
- Incidence: Rare but debilitating.
- Presentation: Disproportionate pain, allodynia, hyperalgesia, swelling, vasomotor changes, trophic changes.
- Management: Early diagnosis is key. Multidisciplinary approach: physical therapy, pain management (nerve blocks, medications), psychological support.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approximate) | Salvage Strategies |
|---|---|---|
| Common Peroneal Nerve Injury | 0.8% - 30% |
Intra-op:
Release compression, primary repair if transected.
Post-op: Observation, physical therapy, AFO. EMG/NCS at 6 weeks. If no improvement by 3-6 months, nerve exploration/neurolysis/repair/grafting. Tendon transfers (e.g., tibialis posterior to dorsum of foot) for permanent foot drop. |
| Stiffness / Arthrofibrosis | 20% - 30% | Aggressive physical therapy, CPM. Manipulation under anesthesia (MUA) if plateaued. Arthroscopic or open arthrolysis for recalcitrant cases. Prevention through early, controlled ROM. |
| Persistent Instability / Failure | 5% - 15% | Detailed workup (stress XR, MRI) to identify failure mechanism (non-anatomic tunnels, graft laxity, unrecognized concomitant injury, malalignment). Revision surgery with meticulous anatomical technique. Consider corrective osteotomy if underlying malalignment contributes to failure. |
| Infection | 1% - 3% |
Superficial:
Oral antibiotics.
Deep: Urgent surgical irrigation & debridement. If acute, graft/hardware retention possible with prolonged antibiotics. If chronic, graft/hardware removal often necessary, followed by staged reconstruction. Culture-specific IV antibiotics. |
| Hardware Irritation/Failure | Variable | Symptomatic hardware removal after graft healing (typically >6-12 months). If hardware failure (e.g., screw pullout) contributes to instability, revision of fixation/reconstruction may be necessary. |
| Thromboembolic Events (DVT/PE) | <5% (higher in MKL) | Prophylaxis (mechanical, pharmacological for high-risk). DVT: Anticoagulation (e.g., LMWH, oral factor Xa inhibitors) for 3-6 months. PE: Emergency medical management, anticoagulation. IVC filter for recurrent PE or contraindication to anticoagulation. |
| Complex Regional Pain Syndrome | <1% | Early diagnosis. Multidisciplinary approach: Physical therapy (desensitization, graded motor imagery), pain management (nerve blocks, gabapentin, pregabalin, antidepressants), psychological support. Refer to pain specialist. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following lateral knee surgery, particularly for PLC reconstruction, is crucial for optimizing outcomes, preventing complications, and facilitating a safe return to activity. Protocols are typically phased, emphasizing protection, controlled motion, progressive strengthening, and neuromuscular re-education. Specific protocols may vary based on the extent of injury, surgical technique, and surgeon preference, but general principles apply.
Phase I: Protection & Early Motion (Weeks 0-6)
- Goals: Protect repairs/reconstructions, control pain and swelling, restore early, controlled range of motion (ROM).
- Weight Bearing: Non-weight bearing (NWB) or touch-down weight bearing (TDWB) with crutches for 4-6 weeks to protect the healing soft tissues, especially the posterolateral corner.
- Bracing: A hinged knee brace is typically worn, often locked in extension for the first 0-2 weeks, then gradually progressing to allow ROM from 0-90° (or as per surgeon's specific instructions to prevent varus stress or external rotation). Brace worn during all activities and sleep.
-
Range of Motion (ROM):
- Passive ROM (PROM): Initiated immediately, often with continuous passive motion (CPM) machine or gentle therapist-assisted exercises. Goals: 0-90° flexion by week 2-4, cautiously increasing to full flexion by week 6, avoiding excessive varus or external rotation stress.
- Active ROM (AROM): Gentle quadriceps and hamstring sets, ankle pumps.
- Edema/Pain Control: RICE (Rest, Ice, Compression, Elevation), NSAIDs, pain medication.
-
Therapeutic Exercises:
- Quad sets, hamstring sets (gentle), gluteal sets.
- Ankle pumps, straight leg raises (SLR) in multiple planes (hip flexion/extension/abduction), ensuring no knee flexion.
- Patellar mobilizations.
Phase II: Strength & Proprioception (Weeks 6-12)
- Goals: Gradual increase in weight bearing, progressive strengthening, restore full ROM, initiate proprioceptive training.
- Weight Bearing: Progress to partial weight bearing (PWB) and then full weight bearing (FWB) over 2-4 weeks, as tolerated and based on stability. Crutches are discontinued once FWB is comfortable and gait is normalized.
- Bracing: Brace worn for ambulation, potentially unlocked. May be discontinued for activities of daily living (ADLs) as strength and stability improve.
- Range of Motion (ROM): Progress towards full, pain-free ROM (0-135° or full flexion).
-
Therapeutic Exercises:
-
Strengthening:
- Closed kinetic chain exercises: Mini-squats, leg presses, wall slides, calf raises, step-ups.
- Open kinetic chain exercises: Gentle hamstring curls (avoiding excessive external rotation), knee extension (limited range initially).
- Hip abduction/adduction strengthening.
- Proprioception: Balance board, single-leg stance, beginning with stable surfaces and progressing to unstable surfaces.
- Cardiovascular: Stationary cycling (low resistance), elliptical, swimming (kickboard initially).
-
Strengthening:
Phase III: Return to Activity (Weeks 12-24+)
- Goals: Maximize strength, power, endurance, agility, and sport-specific skills. Prepare for return to desired activities.
- Weight Bearing: Full unrestricted weight bearing.
- Bracing: May be discontinued or used for high-risk activities as directed by the surgeon.
-
Therapeutic Exercises:
- Advanced Strengthening: Progressive resistance training with emphasis on eccentric control, plyometrics (box jumps, hopping), lunges, squats with increased weight/depth.
- Agility Drills: Ladder drills, cone drills, cutting maneuvers, shuttle runs.
- Sport-Specific Training: Gradually introduce sport-specific activities and drills, ensuring proper form and control.
- Running Program: Initiate a graduated running program.
-
Criteria for Return to Sport:
- Full, pain-free ROM.
- No effusion or tenderness.
- Strength testing (isokinetic or manual) demonstrating >90% strength symmetry compared to the contralateral limb.
- Satisfactory performance on functional tests (e.g., single-leg hop test, agility tests).
- No instability on clinical examination.
- Psychological readiness.
- Clearance from the surgeon.
Key Considerations:
- Individualization: Protocols must be individualized based on patient healing, progress, and goals.
- Graft Protection: The initial phases are critical for graft incorporation and maturation. Overstressing the repair/reconstruction can lead to failure.
- Varus and External Rotation Avoidance: Special caution must be exercised to avoid stressing the healing PLC structures with varus loads or excessive external rotation, particularly in early flexion.
- Patient Education: Patients must be thoroughly educated on the importance of adherence to the protocol and activity restrictions.
Summary of Key Literature / Guidelines
The understanding and management of lateral knee instability, particularly posterolateral corner (PLC) injuries, have evolved significantly due to extensive anatomical, biomechanical, and clinical research. Key literature and established guidelines provide the framework for contemporary practice.
1. Foundational Anatomical and Biomechanical Studies:
*
Hughston et al. (1976):
Pioneering work describing the posterolateral instability patterns and introducing the concept of the arcuate ligament complex, laying the groundwork for understanding the PLC as a distinct entity.
*
Seebacher et al. (1982):
Further delineated the layers of the lateral knee, contributing to the layered understanding used in surgical approaches.
*
LaPrade et al. (2003, 2005, 2010):
Extensive and detailed anatomical dissection studies precisely mapping the origins and insertions of the FCL, popliteus tendon, and popliteofibular ligament. These works, often cited as the basis for "anatomic" PLC reconstructions, established quantitative guidelines for tunnel placement and graft tensioning, demonstrating the critical role of the PFL as the primary static stabilizer to external rotation. Their work highlighted the importance of addressing all injured structures rather than isolated repair.
2. Diagnostic and Classification Systems:
*
Hughston's Classification:
Early classification system based on laxity (Grade I, II, III), providing a general guide for severity.
*
Stress Radiography:
Quantifying varus gapping at 0° and 30° flexion, and posterolateral rotation (dial test) at 30° and 90° flexion, has become a standard diagnostic tool to objectively assess the degree of instability and differentiate isolated FCL injury from combined FCL/PLC injury.
*
Magnetic Resonance Imaging (MRI):
Advanced imaging has become indispensable for detailed soft tissue assessment, confirming clinical suspicions and identifying specific injured structures (e.g., FCL tear, popliteus tendon avulsion, PFL injury, meniscal pathology).
3. Surgical Techniques & Evolution:
*
Non-Anatomic Reconstructions:
Early techniques, such as the Larson procedure or modified MacIntosh tenodesis, aimed to provide extra-articular stability but often resulted in over-constraining the joint or persistent laxity due to non-anatomic graft placement.
*
Anatomic Reconstructions:
Driven by the detailed anatomical studies, current trends favor anatomic reconstructions that aim to replicate the native FCL, popliteus tendon, and PFL. Techniques like the LaPrade "anatomic" PLC reconstruction or the modified anatomic techniques are widely adopted. These involve multiple femoral and fibular tunnels to recreate the precise origins and insertions of the key stabilizers, using single or multiple tendon grafts.
*
Repair vs. Reconstruction:
Acute avulsion injuries (e.g., FCL from femur, PFL from fibula styloid) may be amenable to direct repair with suture anchors, especially if diagnosed and treated early. Mid-substance tears or chronic instabilities typically require formal reconstruction with autograft or allograft.
4. Consensus Statements and Guidelines:
*
International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS):
Regularly publishes consensus statements and instructional courses on multiligamentous knee injuries, including comprehensive recommendations for PLC diagnosis, classification, and surgical management.
*
American Academy of Orthopaedic Surgeons (AAOS):
Provides clinical practice guidelines and educational resources addressing knee ligament injuries, emphasizing evidence-based approaches.
*
Multiligamentous Knee Injury (MKL) Protocols:
Numerous institutions and specialized centers have developed comprehensive diagnostic algorithms and treatment protocols for MKLs, recognizing that PLC injuries rarely occur in isolation in severe trauma. These protocols emphasize simultaneous or staged reconstruction of all injured ligaments to optimize outcomes.
5. Emerging Concepts and Future Directions:
*
Biologic Augmentation:
The use of platelet-rich plasma (PRP) or stem cells to enhance healing and graft incorporation is an area of ongoing research.
*
Kinematic Analysis:
Advanced motion analysis techniques are being used to refine understanding of knee kinematics before and after reconstruction.
*
Patient-Reported Outcome Measures (PROMs):
Increasing emphasis on patient-centered outcomes, utilizing validated PROMs (e.g., KOOS, Lysholm, IKDC) to assess functional recovery and quality of life.
*
Role of Osteotomy:
Recognition of the importance of addressing concomitant varus malalignment, often through high tibial osteotomy (HTO), especially in chronic PLC instability, to offload the lateral compartment and prevent reconstruction failure.
In summary, surgical precision in the lateral knee is predicated upon an exhaustive understanding of its intricate anatomy, derived from decades of dedicated research. Adherence to established diagnostic algorithms, meticulous surgical technique, and structured rehabilitation protocols, all informed by the evolving body of literature, are the cornerstones of successful patient management.
Clinical & Radiographic Imaging


You Might Also Like