Vascularized Joint, Physeal, and Nerve Transfers in Orthopaedics
Key Takeaway
Vascularized free flaps containing joints, epiphyses, and nerves represent the pinnacle of reconstructive microsurgery. These advanced techniques are indicated for massive composite tissue defects, pediatric physeal reconstruction, and extensive nerve gaps within avascular beds. By preserving intrinsic microcirculation, vascularized transfers ensure superior tissue survival, continued longitudinal growth in pediatric patients, and accelerated axonal regeneration compared to conventional non-vascularized grafting methods.
INTRODUCTION TO ADVANCED COMPOSITE TISSUE TRANSFERS
The evolution of reconstructive microsurgery has fundamentally altered the algorithmic approach to massive composite tissue defects. While conventional free tissue transfer effectively addresses soft tissue and diaphyseal bone loss, the reconstruction of articular surfaces, growing physes, and massive peripheral nerve gaps presents a uniquely complex biomechanical and physiological challenge. The clinical experiences of pioneer microsurgeons have demonstrated that whole joints and epiphyseal plates, when transplanted on a meticulously preserved vascular pedicle, can survive, function, and grow without the rapid deterioration characteristic of avascular grafts.
Furthermore, the application of microvascular techniques to peripheral nerve reconstruction—specifically the vascularized nerve graft—has revolutionized the management of extensive nerve defects situated within hostile, avascular recipient beds. This masterclass delineates the indications, biomechanical rationale, step-by-step surgical techniques, and postoperative protocols for vascularized free flaps containing joints and epiphyses, as well as vascularized nerve grafts.
VASCULARIZED FREE FLAPS CONTAINING JOINTS AND EPIPHYSES
The transplantation of a vascularized joint or physis is a formidable undertaking, typically reserved for severe pediatric trauma, post-tumor resection reconstruction, or the correction of profound congenital anomalies. Clinical reports by Weiland et al. and Wray et al. have definitively established that longitudinal growth continues after the vascularized transfer of physes. The meticulous experimental work of Brown et al. further corroborates that long-term survival and useful, predictable growth occur following free vascularized physeal transplantation, provided the microvascular anastomosis remains patent and the delicate epiphyseal blood supply is uncompromised.
Indications and Patient Selection
Patient selection is paramount. These procedures are highly technically demanding and carry significant risks of donor-site morbidity and graft failure.
* Pediatric Post-Traumatic Reconstruction: Reconstruction of joints or long bones following traumatic loss where continued longitudinal growth is mandatory to prevent severe limb-length discrepancies.
* Oncologic Resection: Following wide local excision of primary bone sarcomas (e.g., Ewing sarcoma, osteosarcoma) involving the epiphysis in skeletally immature patients.
* Congenital Deformities: Severe manifestations of radial longitudinal deficiency (radial club hand) or other aplasias requiring joint reconstruction with growth potential.
* Avascular Necrosis: Advanced stages of osteonecrosis where joint preservation is attempted via vascularized joint transfer (e.g., vascularized metatarsophalangeal joint transfer for advanced Kienböck's or Preiser's disease).
Biomechanics and Physeal Physiology
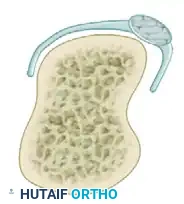
Understanding the dual blood supply of the physis is critical for successful transfer. The physis relies on two distinct vascular networks:
1. Epiphyseal Vessels: Supply the resting and proliferative zones of the physis. Interruption of these vessels leads to immediate cessation of chondrogenesis and irreversible growth arrest.
2. Metaphyseal Vessels: Supply the zone of provisional calcification and the hypertrophic zone. Interruption here disrupts endochondral ossification, leading to a widened, hypertrophic physis, though growth may resume if revascularization occurs rapidly.
Surgical Warning: A vascularized physeal transfer must include both the epiphyseal and metaphyseal blood supplies. Harvesting a bone flap that inadvertently ligates the epiphyseal vessels will result in a viable metaphyseal bone graft but a dead, prematurely fusing physis.
Surgical Technique: Vascularized Proximal Fibula Transfer
The vascularized proximal fibula (containing the fibular head and proximal physis) is the workhorse flap for pediatric physeal reconstruction, commonly utilized to reconstruct the proximal humerus or distal radius.
1. Preoperative Planning and Positioning
- Imaging: High-resolution CT angiography of both the donor and recipient limbs is mandatory to map the vascular anatomy. The proximal fibula is typically supplied by the anterior tibial recurrent artery (ATRA) or the inferior lateral genicular artery (ILGA).
- Positioning: The patient is positioned supine with a bump under the ipsilateral hip of the donor leg to allow internal rotation. A sterile tourniquet is applied to the proximal thigh.
2. Donor Site Approach and Harvest
- Incision: A longitudinal incision is made over the lateral aspect of the leg, extending from the lateral femoral condyle, across the fibular head, and distally along the fibular shaft.
- Nerve Identification: The common peroneal nerve is meticulously identified at the posterior border of the biceps femoris tendon, neurolysed, and protected as it wraps around the fibular neck.
- Vascular Dissection: The anterior compartment musculature is elevated off the interosseous membrane. The ATRA and its venae comitantes are identified branching from the anterior tibial vessels. The pedicle is traced proximally to ensure adequate length.
- Osteotomy and Joint Capsule: The proximal tibiofibular joint capsule is incised. The fibular osteotomy is performed distally at the calculated length using an oscillating saw, preserving the periosteum.
- Harvest: The fibula is isolated on its vascular pedicle. The tourniquet is deflated to confirm perfusion of the fibular head and physis before pedicle ligation.
3. Recipient Site Preparation and Inset
- Bed Preparation: The recipient site is radically debrided to healthy, bleeding tissue. Recipient vessels (e.g., radial artery, brachial artery) are isolated and prepared under the operating microscope.
- Osteosynthesis: The fibular graft is inset. Fixation must be rigid but biologically respectful. Smooth Kirschner wires or bridging plates are utilized. Crucially, hardware must never cross the transplanted physis.
- Microvascular Anastomosis: End-to-end or end-to-side anastomoses are performed using 8-0 or 9-0 nylon sutures. Venous outflow is equally critical; two veins should be anastomosed for every artery if anatomically feasible.
Postoperative Protocol
- Monitoring: Clinical monitoring of a skin paddle (if included) or implantable venous Doppler is utilized for 5 to 7 days.
- Immobilization: The limb is immobilized in a custom orthosis or cast, avoiding any pressure over the pedicle.
- Weight-Bearing: Strict non-weight-bearing or non-loading of the reconstructed extremity is enforced until radiographic evidence of metaphyseal union is observed (typically 8 to 12 weeks).
VASCULARIZED NERVE GRAFTS
When a massive peripheral nerve defect is encountered, standard non-vascularized cable grafts (e.g., sural nerve autografts) are the traditional gold standard. However, standard grafts rely entirely on plasmatic imbibition and subsequent neovascularization from the recipient bed. If the recipient bed is heavily scarred, irradiated, or avascular, standard grafts fail. Furthermore, thick nerve trunks transferred without a blood supply undergo central ischemic necrosis, leading to dense intraneural fibrosis that blocks axonal regeneration.
To circumvent this, Taylor pioneered the vascularized nerve graft. By transferring a donor nerve with its main arterial and venous systems and reestablishing circulation via microvascular techniques, the nerve graft regains immediate, excellent microcirculation throughout its length.
Physiological Rationale and Advantages
Based on extensive experimental and clinical work, vascularized nerve grafts offer profound physiological advantages:
* Schwann Cell Survival: Immediate perfusion prevents Wallerian degeneration-induced Schwann cell death, maintaining a viable cellular environment that actively supports advancing growth cones.
* Prevention of Central Necrosis: The graft does not rely on diffusion, allowing for the transfer of thick nerve trunks without central fibrosis.
* Accelerated Regeneration: Axonal regeneration rates are significantly enhanced. Taylor demonstrated that innervation through revascularized nerve grafts occurs at a rate of 3.2 to 6 cm per month—approximately twice the rate seen in control non-vascularized cable grafts.
Clinical Pearl: Taylor recommended restricting vascularized nerve grafting to younger patients facing massive defects (>10–12 cm) in hostile beds, where conventional nerve grafting techniques are virtually guaranteed to fail.
Indications
- Massive Nerve Gaps: Defects exceeding 10 to 12 cm, particularly involving the median, ulnar, or sciatic nerves.
- Hostile Recipient Beds: Volkmann ischemic contracture, high-voltage electrical burns, severe crush injuries, or post-radiation beds.
- Brachial Plexus Reconstruction: Utilizing a vascularized ulnar nerve graft (from an avulsed C8-T1 root) to reconstruct upper trunk defects.
Surgical Technique: Vascularized Sural Nerve Graft
The sural nerve, supplied by the superficial sural artery (a branch of the popliteal artery), is a common donor for vascularized nerve transfer.
1. Donor Harvest
- Positioning: The patient is placed prone or in a lateral decubitus position.
- Incision: A longitudinal incision is made over the posterior calf, extending from the popliteal fossa to the lateral malleolus.
- Dissection: The lesser saphenous vein and the sural nerve are identified distally. The dissection proceeds proximally, elevating the nerve along with a cuff of surrounding fascia and the superficial sural artery and its venae comitantes.
- Pedicle Isolation: The pedicle is traced to its origin at the popliteal vessels. A skin paddle may be included to monitor postoperative perfusion.
2. Recipient Bed Preparation
- Neuroma Excision: The proximal and distal stumps of the injured nerve are resected back to healthy, bleeding fascicles. The "bread-loafing" technique is used under high magnification until normal fascicular architecture is visualized.
- Vessel Preparation: Healthy recipient arteries and veins in the vicinity of the nerve defect are isolated.
3. Inset, Anastomosis, and Coaptation
- Orientation: The nerve graft is reversed to prevent axonal loss through collateral branches.
- Microvascular Repair: The arterial and venous anastomoses are performed prior to nerve coaptation to minimize ischemia time. Immediate return of bleeding from the epineurial vessels of the graft confirms successful revascularization.
- Nerve Coaptation: Epineurial or group fascicular repair is performed using 8-0 or 9-0 monofilament nylon under the operating microscope. Tensionless coaptation is absolutely critical; the graft must have slight redundancy.
Complications and Pitfalls
While the theoretical and physiological benefits of vascularized nerve grafts are immense, the procedure is fraught with technical challenges.
Surgical Pitfall: The most devastating complication is microvascular thrombosis. If the pedicle thromboses, the massive vascularized nerve graft is instantly converted into a thick, avascular trunk graft. Because of its thickness, it will undergo complete central necrosis, resulting in zero axonal regeneration.
Other complications include:
* Donor Site Morbidity: Loss of sensation in the sural nerve distribution, scarring, and potential neuroma formation.
* Size Mismatch: Discrepancy between the diameter of the donor nerve and the recipient nerve stumps, requiring complex interfascicular splitting and grouping.
FUTURE DIRECTIONS: ALLOGRAFTS AND IMMUNOSUPPRESSION
The principles of vascularized joint, physeal, and nerve transfers are currently being extrapolated into the realm of Composite Tissue Allotransplantation (CTA). As noted in the clinical reports by Gabl et al. regarding bilateral hand transplantation, the use of modern immunosuppressive regimens (e.g., tacrolimus, mycophenolate mofetil, and prednisolone) allows for the survival of allogeneic bone, joints, and nerves.
While autologous vascularized transfers remain the gold standard due to the absence of immunosuppression-related morbidity, the future of pediatric joint reconstruction and massive nerve defect management may lie in off-the-shelf vascularized allografts. Until the risk-benefit ratio of systemic immunosuppression is optimized for non-life-saving procedures, the autologous vascularized free flap remains the most powerful tool in the reconstructive orthopaedic surgeon's armamentarium for salvaging the unsalvageable limb.
You Might Also Like