Principles of Tendon Transfer in the Upper Extremity: A Master Academic Guide
Key Takeaway
Tendon transfer surgery is a cornerstone of upper extremity reconstruction, designed to restore lost motor function following neurologic, traumatic, or congenital deficits. Success relies on strict adherence to biomechanical principles, including donor muscle expendability, adequate amplitude of excursion, synergistic action, and optimal tensioning. Furthermore, a pristine soft tissue bed, supple joints, and skeletal stability are absolute prerequisites before undertaking any transfer procedure to ensure predictable, functional outcomes.
INTRODUCTION TO TENDON TRANSFER SURGERY
Tendon transfer surgery remains one of the most elegant and biomechanically demanding disciplines within operative orthopaedics and hand surgery. The fundamental objective is the restoration of lost motor function—whether secondary to traumatic peripheral nerve injury, congenital anomalies, infectious sequelae (such as poliomyelitis), or vascular insults—by re-routing a functioning, expendable muscle-tendon unit to substitute for a paralyzed or absent one.
The success of a tendon transfer is not merely dictated by surgical execution but by meticulous preoperative planning, a profound understanding of upper extremity biomechanics, and strict adherence to established physiological principles. Failure to respect these principles invariably leads to functional failure, exacerbation of muscular imbalance, and the genesis of secondary deformities.
PREOPERATIVE EVALUATION AND STRATEGIC PLANNING
The foundation of a successful tendon transfer lies in the exhaustive evaluation of the hand and upper extremity, categorizing the functional deficits and cataloging the retained assets.
The Functional Ledger
A systematic approach, originally popularized by pioneers such as Boyes and Brand, involves creating a "functional ledger." The surgeon must list the critical functions that have been lost in one column, and the available, expendable muscles in the opposite column.
When matching available muscles to needed functions, the surgeon must prioritize the restoration of fundamental biomechanical pillars:
1. Wrist Extension: The cornerstone of hand function, providing the stable platform necessary for the tenodesis effect and powerful grip.
2. Finger Flexion: Essential for grasp.
3. Finger and Thumb Extension: Necessary for the release of objects.
4. Thumb Opposition/Abduction: Critical for pinch and fine motor manipulation.
Clinical Pearl: Never attempt to restore a secondary function at the expense of a primary one. For example, restoring finger extension is strictly contraindicated if it requires sacrificing a major wrist or finger flexor that compromises the patient's grip strength.
BIOMECHANICAL PRINCIPLES OF MUSCLE SELECTION
Selecting the appropriate donor muscle requires a rigorous assessment of four primary biomechanical parameters: expendability, strength, amplitude of excursion, and synergy.
1. Expendability
A muscle is deemed expendable only if its removal does not create a new, unacceptable functional deficit. The donor muscle must have a synergist or secondary muscle left in situ that can adequately assume its original role. For instance, the flexor carpi radialis (FCR) is often preserved to stabilize the wrist, while the palmaris longus (PL) or flexor carpi ulnaris (FCU) may be utilized as donors.
2. Muscle Strength and the "One-Grade Loss" Rule
The absolute power of a muscle is proportional to its physiological cross-sectional area (PCSA). Muscle strength is evaluated clinically using the Medical Research Council (MRC) grading system:
* 0 (Zero): No palpable or visible contraction.
* 1 (Trace): Palpable contraction, no joint motion.
* 2 (Poor): Moves joint with gravity eliminated.
* 3 (Fair): Moves joint against gravity.
* 4 (Good): Moves joint against gravity and moderate resistance.
* 5 (Normal): Normal strength against full resistance.
Surgical Warning: A transferred muscle universally loses at least one MRC grade of strength due to the trauma of mobilization, altered biomechanics, and the formation of postoperative adhesions. Therefore, a donor muscle must be graded as 4 (Good) or 5 (Normal) preoperatively to yield a satisfactory functional result.
3. Amplitude of Excursion
Excursion refers to the maximum linear distance a muscle can contract. It is directly proportional to the resting length of the muscle fibers. Tendons must possess sufficient excursion to replicate the function of the paralyzed unit.
* Wrist Flexors/Extensors: ~33 mm of excursion.
* Finger Extensors: ~50 mm of excursion.
* Finger Flexors: ~70 mm of excursion.
A donor muscle with a short excursion cannot fully replace a muscle requiring a long excursion. However, surgical modifications can optimize this. The brachioradialis (BR), an excellent and highly expendable donor, inherently possesses a short excursion. As demonstrated by Boyes, the excursion of the BR can be significantly augmented by aggressively dissecting its tendon proximally and releasing all fascial attachments to the surrounding septa. Despite this, the BR is generally insufficient to restore full finger flexion but is highly effective for restoring thumb flexion (FPL), where even limited interphalangeal joint motion is functionally invaluable.
4. Synergy and Cortical Re-education
Muscles that function together during a specific movement pattern are synergistic. For example, wrist flexors act synergistically with finger extensors (the tenodesis effect). Utilizing a synergistic muscle for transfer (e.g., transferring the FCU to the Extensor Digitorum Communis) dramatically simplifies postoperative cortical re-education. The patient intuitively fires the donor muscle during the desired action, leading to faster and more reliable rehabilitation.
PREREQUISITES FOR TENDON TRANSFER: THE TISSUE BED AND TIMING
Tendon transfer is the final step in the reconstructive ladder of the hand. It is doomed to fail if the foundational elements of the limb are not optimized prior to surgery.
The Soft Tissue Bed
Transferred tendons must glide seamlessly. They must be routed through healthy, well-vascularized subcutaneous fat. Routing a tendon through dense scar tissue, or allowing it to rest directly against raw bone, guarantees dense adhesion formation and functional failure. If the soft tissue envelope is compromised, a preliminary procedure—such as a pedicled groin flap, anterolateral thigh (ALT) free flap, or local fascial flap—must be performed to provide a pliable, fat-rich bed.
Joint Suppleness and Skeletal Stability
Surgical Pitfall: Tendon transfers cannot overcome joint contractures. A transferred tendon lacks the power to mobilize a stiff joint and will rapidly stretch out or rupture if forced to pull against a fixed deformity.
A full, satisfactory range of passive joint motion is an absolute prerequisite. Any capsular contractures must be addressed via serial splinting, therapy, or surgical capsulotomy prior to the transfer. Furthermore, skeletal architecture must be stable. Malunions must be corrected via osteotomy, and nonunions must be bone-grafted and healed before tendon transfer is contemplated.
Restoration of Sensibility
A hand without protective sensation is a blind hand. While motor function is critical, the utility of a reconstructed hand is severely limited if sensibility is absent. Nerve repairs, grafts, or sensory nerve transfers should precede or accompany motor tendon transfers whenever feasible.
Timing of the Transfer
The timing of intervention is dictated by the etiology of the paralysis:
* Poliomyelitis: Spontaneous recovery of muscle power may occur up to 18 months post-acute infection. Tendon transfers must be delayed until this plateau is reached, as premature transfer may sacrifice a muscle that would have otherwise recovered.
* Syringomyelia and Progressive Neuropathies: Extreme caution is advised. Weakness may progress postoperatively, rendering the transfer ineffective or exacerbating imbalances.
* Peripheral Nerve Injuries: Each nerve lesion is evaluated individually based on the distance from the injury to the motor endplate (nerve regeneration occurs at ~1 mm/day).
* Radial Nerve: For mid-humeral lesions, definitive transfers for finger/thumb extension are typically delayed for 6 months post-neurorrhaphy. However, an early "internal splint" transfer (Pronator Teres to Extensor Carpi Radialis Brevis) is highly recommended. This immediately restores wrist extension, eliminates the need for cumbersome external splinting, and dramatically improves hand function while awaiting radial nerve regeneration.
* Median Nerve: In high median nerve lesions, proximal muscle function (e.g., Pronator Teres, FCR) should show signs of recovery within 4 months. In low lesions, thenar muscle recovery should begin by 3 months. If clinical or electromyographic (EMG) evidence of recovery is absent by these milestones, surgical exploration or definitive tendon transfers should be executed.
TECHNICAL CONSIDERATIONS AND SURGICAL EXECUTION
The intraoperative execution of a tendon transfer requires meticulous tissue handling, precise routing, and exact tensioning.
Intraoperative Muscle Evaluation
Clinical grading is paramount, but intraoperative visual inspection provides the final confirmation of muscle viability.
* Healthy Muscle: Dark pink or red, indicating robust vascularity, normal nutrition, and healthy muscle fibers. It will demonstrate brisk contractility when mechanically stimulated.
* Unsuitable Muscle: Pale pink, atrophic, and fibrotic. A muscle that exhibits these characteristics, or demonstrates less-than-normal excursion when pulled intraoperatively, must be abandoned as a donor (see Figure 68-3 in standard texts).
Routing the Transfer: The Line of Pull
The biomechanical efficiency of a muscle is maximized when it pulls in a straight line from its origin to its new insertion.
* Avoid Acute Angles: A muscle and its tendon should never form an acute angle. The straighter the line of pull, the more efficient the force transmission. If an angle is unavoidable, a biomechanical pulley system must be utilized, though this increases friction and the risk of adhesions.
* Angle of Approach and Bowstringing: The greater the angle of approach of a tendon to the bone, the greater the rotational force (torque) exerted across the joint. However, without a competent retinacular pulley system, this steep angle creates a "bowstring" effect, which drastically reduces the tendon's effective excursion and creates cosmetic and functional deformities.
Distal vs. Proximal Attachment
The biomechanical lever arm dictates that the further distal a tendon is anchored from the axis of rotation of a joint, the greater the moment arm and the more power the muscle can exert. However, this mechanical advantage comes at a cost: a distally attached tendon requires significantly more amplitude of excursion to achieve the same arc of joint motion compared to a proximally attached tendon.
Tensioning the Transfer
Tensioning is arguably the most critical and technically demanding step of the procedure. It relies on the physiological length-tension relationship (the Blix curve).
* A muscle transferred too loosely will expend its entire excursion merely taking up the slack, resulting in a severe lag and functional failure.
* A muscle transferred too tightly will cause ischemia of the muscle belly, subsequent fibrosis, and a fixed contracture of the joint.
The Resting Cascade: When tensioning a transfer for finger flexion or extension, the surgeon must observe the natural tenodesis cascade of the hand. With the wrist in neutral, the fingers should assume a natural cascade of increasing flexion from the index to the small finger.
* Chronically Detached Muscles: A muscle that has been detached or paralyzed for a prolonged period will have developed a physiologic contracture. These tendons must be anchored under slightly higher tension than normal, as the muscle belly will inevitably stretch and undergo stress-relaxation postoperatively, regaining some of its excursion.
Fixation Techniques
Robust fixation is required to allow for early active rehabilitation.
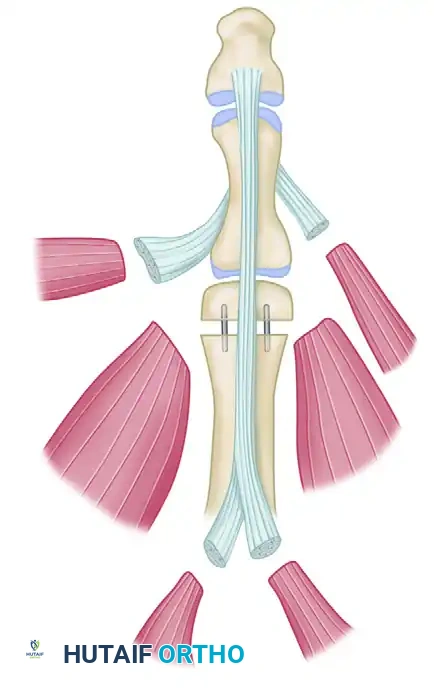
* Tendon-to-Tendon: The Pulvertaft weave remains the gold standard. The donor tendon is woven through the recipient tendon a minimum of three times, with each pass oriented at 90 degrees to the previous one. This maximizes the surface area for healing and provides immense biomechanical pull-out strength. The weaves are secured with non-absorbable mattress sutures (e.g., 3-0 or 4-0 braided polyester).
* Tendon-to-Bone: When inserting directly into bone, techniques such as interference screws, suture anchors, or transosseous drill holes over a cortical button are utilized. The tendon must be stripped of its paratenon and placed directly against bleeding cancellous bone to promote osteointegration.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The surgical procedure is only half the battle; rigorous, specialized hand therapy is mandatory.
Phase I: Immobilization (0 to 3-4 Weeks)
The limb is immobilized in a custom orthosis that places the transferred tendon in a position of minimal tension. For example, following an FCU to EDC transfer for finger extension, the wrist is splinted in 30-40 degrees of extension, and the metacarpophalangeal (MCP) joints are splinted in full extension. This protects the Pulvertaft weave during the vulnerable inflammatory and early fibroblastic phases of tendon healing.
Phase II: Early Mobilization and Cortical Re-education (4 to 8 Weeks)
Once early tensile strength is achieved, the cast is removed, and a removable thermoplastic splint is fabricated.
* Active Assisted Range of Motion (AAROM): Initiated to promote tendon gliding and prevent dense adhesions.
* Cortical Re-education: The therapist works with the patient to fire the donor muscle in its new role. Biofeedback and mirror therapy are highly effective adjuncts. If a synergistic transfer was used, this phase progresses rapidly.
Phase III: Strengthening and Integration (8+ Weeks)
Progressive resistance exercises are introduced. The focus shifts from isolated joint motion to integrating the transferred muscle into complex, multi-joint functional tasks, such as power grasp, key pinch, and fine motor manipulation. Maximum medical improvement following a tendon transfer is typically not realized until 9 to 12 months postoperatively.
CONCLUSION
Tendon transfer surgery is a powerful tool in the orthopaedic surgeon's armamentarium for restoring independence and function to the paralyzed upper extremity. By strictly adhering to the principles of donor expendability, matching excursion and strength, ensuring a pristine soft tissue bed, and executing precise surgical tensioning, the surgeon can achieve predictable, life-altering outcomes for their patients. Mastery of these principles is essential for any resident, fellow, or consultant undertaking complex reconstructive surgery of the hand and upper limb.
You Might Also Like