Comprehensive Management of Congenital Hand Anomalies: Abductor Digiti Minimi Opponensplasty and Central Deficiencies
Key Takeaway
The Huber abductor digiti minimi opponensplasty is a highly effective tendon transfer utilized primarily for congenital thenar aplasia or post-pollicization weakness. By mobilizing the abductor digiti minimi on its neurovascular pedicle and transferring it subcutaneously to the thumb, surgeons can restore critical opposition and pinch kinematics. This guide details the Manske and McCarroll technique, biomechanical principles, and the comprehensive management of associated central hand deficiencies.
INTRODUCTION TO CONGENITAL THUMB AND RAY ANOMALIES
The reconstruction of congenital hand anomalies demands a profound understanding of pediatric biomechanics, neurovascular anatomy, and the natural history of embryological failures. Among the most functionally critical reconstructions is the restoration of thumb opposition in the setting of thenar hypoplasia or aplasia. The abductor digiti minimi (ADM) opponensplasty, originally described by Huber, remains a cornerstone technique for this purpose. Furthermore, the management of central ray deficiencies (cleft hand) requires meticulous classification and staged reconstruction to optimize both prehension and cosmesis. This masterclass delineates the operative nuances of the Huber opponensplasty and the academic framework surrounding central hand deficiencies.
ABDUCTOR DIGITI MINIMI OPPONENSPLASTY (HUBER PROCEDURE)
The abductor digiti minimi opponensplasty is a highly specialized muscle transfer designed to restore thumb opposition. Unlike traditional tendon transfers (such as the flexor digitorum superficialis or extensor indicis proprius transfers), the Huber procedure transfers the entire ADM muscle belly to the thenar region. This provides a dual benefit: it restores the biomechanical vector of opposition and simultaneously reconstructs the cosmetic bulk of the deficient thenar eminence.
Indications and Patient Selection
The Huber opponensplasty is primarily indicated for pediatric patients presenting with absent or severely deficient thumb opposition. Specific clinical scenarios include:
* Isolated Thenar Aplasia: A rare congenital anomaly (often associated with Cavanagh's syndrome) where the thumb is otherwise structurally sound but lacks intrinsic thenar musculature.
* Radial Longitudinal Deficiency (Radial Club Hand): When associated with a hypoplastic thumb (Blauth Type II or IIIA) that requires stabilization and opposition reconstruction.
* Post-Pollicization: Patients who exhibit weakness in apposition and pinch strength following index finger pollicization for thumb aplasia.
Clinical Pearl: Manske and McCarroll reported significant improvements in appearance, dexterity, strength, and overall usefulness of the thumb in 20 out of 21 patients undergoing this procedure. The average age at the time of operation in their landmark series was 4 years and 9 months, highlighting the efficacy of early intervention before abnormal compensatory pinch patterns become rigidly established.
Surgical Anatomy and Biomechanics
Successful execution of the Huber transfer relies on the preservation of the ADM's neurovascular pedicle.
* Origin: Pisiform bone and the tendon of the flexor carpi ulnaris (FCU).
* Insertion: The ulnar base of the proximal phalanx of the little finger and the ulnar slip of the extensor expansion.
* Innervation: The deep motor branch of the ulnar nerve, which enters the muscle on its deep, proximal, and radial aspect.
* Vascular Supply: Branches of the ulnar artery, arborizing in the same proximal-radial neurovascular hilum.
By mobilizing the ADM on this proximal pedicle and folding it over 180 degrees (like a page in a book) into the thenar space, the muscle's line of pull is redirected to mimic the abductor pollicis brevis (APB), providing a robust pronation and palmar abduction vector.
Surgical Technique (Manske and McCarroll)
The procedure is performed under general anesthesia with the patient supine. A well-padded upper extremity tourniquet is utilized, and loupe magnification is highly recommended for neurovascular dissection.
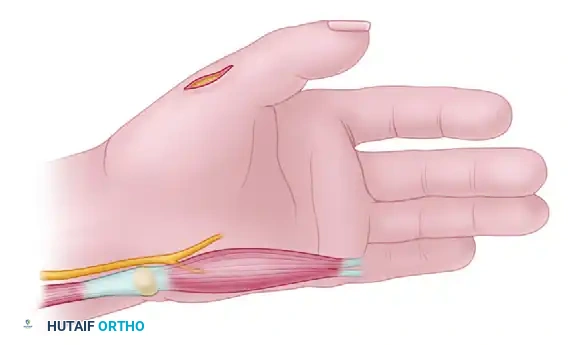
1. Incision and Exposure
Make an initial incision beginning over the ulnar border of the proximal phalanx of the little finger and the palm. Curve the incision radialward proximal to the metacarpophalangeal (MCP) joint, crossing the wrist crease on the radial side of the pisiform.
2. Tendon Detachment
Identify the distal insertions of the ADM. Carefully detach the tendinous insertions into the extensor hood and the base of the proximal phalanx of the little finger. It is critical to retain as much tendon length as possible to facilitate secure fixation at the thumb.
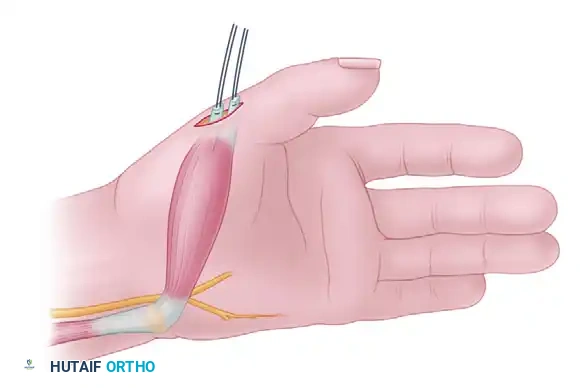
3. Muscle Mobilization
Starting distally, dissect the ADM muscle out of its fascial sheath, elevating it proximally toward its origin at the pisiform.
Surgical Warning: Strict avoidance of dissection on the proximal and radial sides of the muscle belly is mandatory. The neurovascular bundle (deep ulnar nerve and arterial branches) enters the muscle in this zone. Overzealous proximal dissection will result in denervation or devascularization of the transfer.
4. Tunnel Creation and Muscle Transfer
Make a second incision over the dorsoradial aspect of the MCP joint of the thumb. Create a large, capacious subcutaneous tunnel connecting the thumb incision to the proximal ulnar incision across the palm. Pass the mobilized ADM muscle through this tunnel.
Ensure that the muscle glides freely within the tunnel. A tight tunnel will cause venous congestion, muscle ischemia, and ultimate failure of the transfer. The muscle should be rotated 180 degrees on its longitudinal axis so that its deep surface becomes superficial, optimizing the vector of pull.
5. Tendon Insertion Strategies
The method of insertion at the thumb MCP joint is dictated by the patient’s specific pathoanatomy:
- Thenar Aplasia with Other Radial Anomalies: Suture one of the transferred tendinous slips to the soft tissue at the radial aspect of the base of the proximal phalanx. Suture the second slip to the extensor pollicis longus (EPL) muscle at the level of the MCP joint, as recommended by Riordan, Powers, and Hurd. This dual insertion provides both abduction and extension-pronation vectors.
- Isolated Thenar Aplasia: These patients often present with profound MCP joint instability. Stabilize the MCP joint by imbricating the redundant ulnar capsule in a "pants-over-vest" fashion. Following stabilization, suture one of the ADM tendinous insertions to the radial capsule, and the other to the imbricated ulnar capsule and the EPL tendon.
- Post-Pollicization: If the opponensplasty is performed to augment a pollicized index finger, suture one slip to the radial lateral band and the other to the central slip at the proximal interphalangeal (PIP) joint of the newly pollicized digit.
6. Closure and Immobilization
Deflate the tourniquet and achieve meticulous hemostasis. Close the incisions in a routine fashion using absorbable sutures. Apply a bulky, well-padded dressing and a custom fiberglass splint, holding the thumb in maximal opposition and palmar abduction.
Postoperative Care and Rehabilitation
- 0 to 3 Weeks: The hand is strictly immobilized in the bulky dressing and splint to protect the tendon transfer and capsulorrhaphy.
- 3 to 6 Weeks: The bulky dressing is removed. The thumb is taped or placed in a custom thermoplastic splint holding it in opposition for an additional 3 weeks. During this phase, the child is actively encouraged to use the hand for light, play-based activities.
- 6 Weeks Postoperative: All dressings and rigid splints are discontinued.
Clinical Pearl: Unlike adult tendon transfers, formal motor retraining and biofeedback are usually unnecessary in the pediatric population. The innate cortical plasticity of children allows them to spontaneously integrate the transferred ADM into their pinch and grasp patterns.
CLEFT HAND: CENTRAL DEFICIENCIES
Central deficiencies of the hand represent a complex spectrum of malformations characterized by the longitudinal failure of formation of the second, third, or fourth rays. This condition challenges the reconstructive surgeon due to the profound functional and psychological impact on the developing child.
Nomenclature and Epidemiology
Historically, these deformities have been burdened with pejorative terms such as ectrodactyly, crab claw, or lobster claw. In modern academic orthopedics, the preferred terminology is Cleft Hand or Central Longitudinal Deficiency.
Severe suppression of the radial four rays, leaving only a one-digit (fifth-ray) hand, falls into this spectrum. However, further suppression resulting in a completely digitless hand is classified separately as a transverse deficiency (symbrachydactyly). Cleft hand is exceedingly rare, with an estimated incidence of approximately 1 per 90,000 live births.
Pathoanatomy and Classification
Central deficiencies are broadly classified into two distinct pathoanatomic patterns: Typical and Atypical. The distinction is critical, as they represent entirely different embryological failures and genetic backgrounds.
1. The Typical Pattern (True Cleft Hand)
- Morphology: Presents as a central V-shaped cleft with variable degrees of deficiency of the long (third) ray.
- Associated Anomalies: Syndactyly between the ulnar digits (ring and small) and radial digits (thumb and index) is highly common. Transverse bones (cross-bones) may be present at the base of the cleft, progressively widening the deformity as the child grows.
- Laterality: Typically bilateral.
- Systemic Involvement: Frequently associated with similar V-shaped cleft deformities of the feet.
- Genetics: Demonstrates an autosomal dominant mode of inheritance with variable expressivity and incomplete penetrance. It is frequently linked to mutations in the SHFM (Split Hand/Foot Malformation) gene loci.
2. The Atypical Pattern (Symbrachydactyly Variant)
- Morphology: Initially described by Lange, this presents as a severe, wide U-shaped deficiency involving the index, long, and ring rays. Often, only a thumb and a little finger remain attached to the hand.
- Laterality: Usually unilateral.
- Systemic Involvement: Occurs without associated foot deformities.
- Genetics: Occurs sporadically without a predictable inheritance pattern.
- Academic Consensus: According to Ogino and modern embryological studies, the atypical pattern should not be classified as a true cleft hand, but rather as a severe form of symbrachydactyly. Flatt strongly supported this distinction, suggesting that the term cleft hand be reserved exclusively for typical patterns, while lobster claw (though historically used) described the fully developed atypical pattern.
Flatt’s Classification of Cleft Hand
Flatt proposed a comprehensive classification system for true cleft hand malformations based on the extent of ray involvement:
* Group 0: All bones are present (often presenting as a simple central syndactyly with an underlying osseous cleft).
* Group 1: One ray involved (typically the long finger).
* Group 2: Two rays involved.
* Group 3: Three rays involved.
These groups are further subdivided into three subgroups based on the specific degree of phalangeal and metacarpal involvement, guiding the surgical reconstructive algorithm.
Embryology and Pathogenesis
The exact etiology of central deficiencies remains a subject of intense academic debate. Most cases of the atypical form occur sporadically due to vascular disruptions or mesodermal defects during the 4th to 6th weeks of gestation.
For the typical pattern, Maisels proposed the Centripetal Suppression Theory. According to this model, the deformity represents a spectrum of central ray suppression. Milder deformities present as a simple soft-tissue cleft without significant osseous tissue loss. As the suppression becomes more severe, there is progressive centripetal loss of the central rays, leading to the classic deep V-cleft and eventual merging of the adjacent digits (syndactyly).
Principles of Surgical Reconstruction
The management of cleft hand is highly individualized. Surgery is typically performed between 6 and 18 months of age to harness neuroplasticity and prevent the progressive widening of the cleft by transverse bones.
Primary Surgical Goals:
1. Closure of the Cleft: Restoring the aesthetic appearance of the hand by closing the central defect.
2. Release of Syndactyly: Separating the border digits to restore independent motion, particularly the first web space to allow for thumb opposition and grasp.
3. Excision of Deforming Forces: Removal of transverse bones or tethering fibrous bands that force the border digits into divergence.
4. Reconstruction of the Deep Transverse Metacarpal Ligament: Essential to prevent the metacarpals from splaying postoperatively.
Techniques such as the Snow-Littler procedure (which utilizes a palmar flap to reconstruct the first web space while transposing the index ray ulnarward) or the Miura-Komedal procedure are mainstays in the surgical armamentarium. In cases where the thumb lacks opposition following cleft closure, an ADM opponensplasty (as detailed above) may be utilized as an adjunct procedure to optimize final hand kinematics.
You Might Also Like

