Comprehensive Surgical Management of Upper Extremity Injection, Extravasation, and Wringer Injuries

Key Takeaway
High-pressure injection, extravasation, and wringer injuries represent severe orthopedic emergencies that often present with deceptively benign superficial wounds. Immediate recognition, aggressive surgical debridement, and meticulous soft-tissue management are paramount. This guide details the pathophysiology, step-by-step surgical approaches, and postoperative protocols required to mitigate catastrophic outcomes such as compartment syndrome, extensive tissue necrosis, and subsequent amputation in complex upper extremity trauma.
INTRODUCTION TO COMPLEX SOFT TISSUE TRAUMA OF THE HAND
The upper extremity is uniquely vulnerable to a spectrum of severe soft tissue injuries, particularly those sustained in industrial and iatrogenic settings. Among the most deceptive and limb-threatening of these are high-pressure injection injuries, chemical extravasation events, and wringer (roller crush) injuries. While the initial clinical presentation of these injuries may appear benign—often presenting as a mere pinpoint puncture or superficial abrasion—the underlying pathophysiology involves catastrophic kinetic energy transfer, chemical cytotoxicity, and delayed ischemic necrosis.
For the practicing orthopedic surgeon, hand fellow, and resident, mastering the evidence-based protocols for these injuries is critical. Delayed or inadequate surgical intervention frequently results in compartment syndrome, irreversible tissue necrosis, and the need for digital or ray amputations. This comprehensive guide delineates the biomechanics, clinical evaluation, step-by-step surgical management, and postoperative rehabilitation protocols for these complex upper extremity emergencies.
HIGH-PRESSURE INJECTION INJURIES
High-pressure injection injuries are true surgical emergencies. They typically occur when industrial equipment (such as paint sprayers, grease guns, or hydraulic lines) accidentally discharges into the hand. The pressure generated by these devices can exceed 10,000 psi, easily breaching the dermal barrier and forcefully dissecting along the path of least resistance—usually the neurovascular bundles and flexor tendon sheaths.
Pathophysiology and Biomechanics
The severity of a high-pressure injection injury is dictated by three primary factors:
1. Kinetic Energy and Mechanical Trauma: The sheer force of the injection causes immediate mechanical disruption of tissues. The fluid rapidly expands within the closed fascial spaces of the digits and palm, leading to an acute rise in interstitial pressure.
2. Chemical Toxicity: The injected material (e.g., oil-based paint, grease, solvents) acts as a severe chemical irritant. Solvents dissolve lipid cell membranes, leading to rapid liquefactive necrosis, while paints trigger a massive, acute inflammatory response.
3. Secondary Ischemia: The combination of volume expansion and profound inflammatory edema rapidly precipitates compartment syndrome. The digital arteries, which are end-vessels, are highly susceptible to compression and subsequent thrombosis.
Surgical Warning: The initial puncture wound is notoriously misleading. A pinpoint entry wound at the index finger pulp can mask the presence of toxic material that has tracked proximally into the deep palmar space or even the carpal tunnel. Never underestimate a high-pressure injection injury based on superficial appearance.
Clinical Evaluation
Patients typically present with a history of equipment malfunction or accidental discharge. The entry wound is often minuscule.
Figure A: Site of high-pressure injection of an unknown substance. The patient complained of severe, disproportionate pain and numbness of the digit and palm, despite the deceptively small puncture wound.
In severe cases, the immense pressure can cause bursting of the skin at distant sites. A classic presentation involves the bursting of the skin at the thumb web space, with the thenar muscles protruding through the traumatic opening.
Key Clinical Findings:
* Pain out of proportion: The hallmark of impending compartment syndrome.
* Pallor and altered capillary refill: Indicative of digital artery compression.
* Sensory deficits: Numbness or paresthesia in the distribution of the digital nerves due to direct compression or chemical neuropraxia.
* Swelling and induration: The digit is often held in a flexed posture, and passive extension elicits excruciating pain.
Surgical Approach and Debridement
Hospitalization and immediate surgical intervention are universally required. The goal of surgery is complete decompression of the involved compartments and meticulous removal of all foreign material and necrotic tissue.
Step-by-Step Surgical Technique:
1. Anesthesia and Positioning: General anesthesia or a regional brachial plexus block is preferred. Avoid local infiltration (e.g., digital blocks), as this further increases compartment pressures. The patient is positioned supine with a radiolucent hand table. A pneumatic tourniquet is applied but should be inflated only after exsanguination by elevation (avoid Esmarch bandages to prevent proximal milking of the injected material).
2. Incision and Exposure: Wide exposure is mandatory. A modified Brunner (zigzag) incision or mid-axial incision is utilized to open the entire involved digit. The incision must be extended proximally into the palm or forearm as far as the material has tracked.
3. Decompression: The flexor tendon sheath must be opened. If the material has entered the palm, the carpal tunnel and Guyon's canal may require release.
4. Debridement: All foreign material must be meticulously excised. This often requires magnification (loupes or operating microscope).

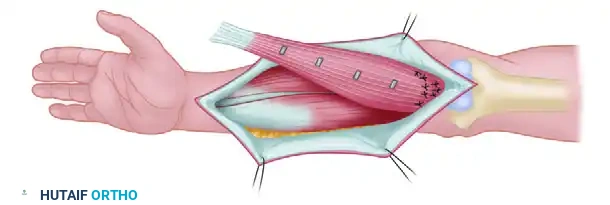
Figure B: Extensive debridement performed through a modified Brunner incision. Note the wide exposure required to adequately visualize and remove the injected substance along the flexor tendon sheath.
- Irrigation: Copious irrigation with normal saline is performed. The limb is cleaned with soap and water, and any open wounds are aggressively debrided.
- Wound Management: The wounds are never closed primarily. They are left open for delayed primary closure, secondary intention, or subsequent skin grafting.
Complications and Compartment Syndrome
Despite aggressive early debridement, the intense inflammatory response can still lead to delayed compartment syndrome and tissue death.
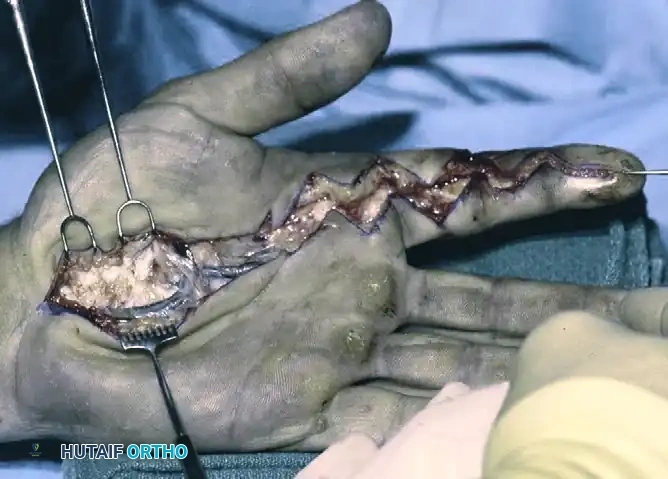
Figure C: Two days after the initial surgery, progressive compartment syndrome necessitated extensive dorsal and volar fasciotomies. Repeated debridements of devitalized tissue were required, ultimately culminating in the amputation of the left index finger due to irreversible necrosis.
Clinical Pearl: Serial examinations are critical. If necessary, any devitalized tissue identified during subsequent dressing changes must be excised promptly. Amputation is often required for organic solvents or oil-based paints that cause intractable necrosis.
Postoperative Protocol and Outcomes
Postoperatively, a pressure dressing that includes the entire hand is applied immediately, with meticulous care taken to distribute the pressure evenly.
* Dressing Application: First, the area is covered by finely woven, nonadherent gauze, followed by flat gauze pads. Next, large masses of cotton and an elastic bandage are rolled on evenly to provide uniform compression without creating a tourniquet effect.
* Elevation: The extremity is strictly elevated and kept so throughout the acute treatment phase to minimize edema.
* Wound Checks: At 24 hours, the dressing is removed. The wound is inspected for blisters, hematomas, and necrosis, and the dressing is reapplied. This process is repeated every 24 hours until the injury becomes stabilized.
With rigorous adherence to early debridement and structured rehabilitation, functional recovery can be achieved, though stiffness and sensory deficits are common.
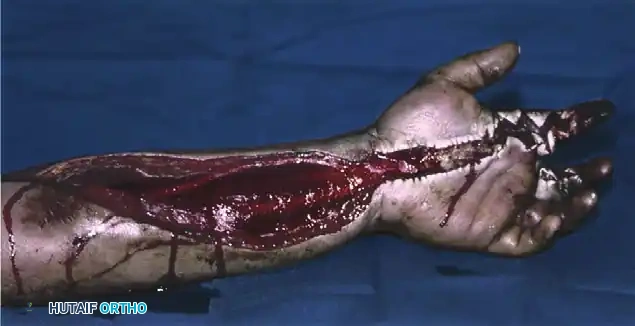
Figure D: Volar view demonstrating hand function at 7 months after the initial injury and subsequent index finger amputation.

Figure E: Fist view at 7 months post-injury, showing acceptable functional recovery of the remaining digits following aggressive early surgical management and rehabilitation.
EXTRAVASATION AND CHEMICAL INJECTION INJURIES
Extravasation injuries occur when intravenously administered medications or radiographic contrast materials inadvertently leak into the surrounding subcutaneous tissues. The severity ranges from mild local inflammation to full-thickness skin necrosis and deep tissue destruction.
Pathophysiology of Extravasation
Agents are generally classified into vesicants (causing blistering and tissue necrosis) and non-vesicants.
* Radiographic Contrast: Although extravasation of radiographic contrast materials probably occurs more often than literature reports suggest, severe skin necrosis as a complication has been reported in approximately 0.5% of radiographic contrast studies. Large extravasations can result in skin necrosis, producing painful ulcers that are notoriously slow to heal.
* Phenytoin: Extravasation of phenytoin (Dilantin) is highly alkaline and can cause severe soft tissue damage, often referred to as "Purple Glove Syndrome."
* Chemotherapeutic Agents: Drugs like doxorubicin are potent vesicants that bind to tissue DNA, causing a prolonged, progressive cycle of tissue necrosis.
Medical Management and Antidotes
Historically, various pharmacological antidotes have been proposed to mitigate tissue damage. Reported antidotes include:
* Hydrocortisone
* Hyaluronidase (to break down hyaluronic acid and disperse the extravasated fluid)
* Propranolol and Isoproterenol
* Sodium bicarbonate
* Topical dimethyl sulfoxide (DMSO)
* Vitamin E and heat packs
However, for the treatment of upper extremity injuries from medications, modern clinical consensus suggests that the best results are obtained with the immediate discontinuation of the intravenous line, elevation of the part, avoidance of antidotes, late debridement and coverage, and incorporation of a rehabilitation program early in the recovery.
For specific scenarios, such as treating phenytoin extravasation in the hand, conservative management consisting of elevation and splinting with a compression dressing has proven effective, provided there is an absence of cellulitis, abscess formation, skin loss, or compartment pressure elevation.
Surgical Techniques for Extravasation
When surgical intervention is warranted, clinical studies heavily support early debridement, drainage, irrigation, repeat debridement, and delayed closure as the methods that consistently yield the best results. Loth and Jones reported that early surgical debridement, wound lavage, and delayed closure produced “excellent” functional and cosmetic outcomes for contrast extravasation.
Advanced Surgical Adjuncts:
* Fluorescence-Guided Debridement: Ultraviolet light has been found to be highly useful in locating and removing fluorescent doxorubicin-containing tissue. Furthermore, after removing the extravasated fluid, intravenous fluorescein can be injected to determine the exact demarcation between viable and nonviable tissue, guiding precise surgical debridement.
* Liposuction and Saline Flush: A minimally invasive technique has gained traction for acute extravasation. Healing without soft tissue injury has been reported in 86% to 96% of patients with the use of liposuction and a saline flush to mechanically remove the extravasated material while preserving the overlying skin.
* Animal Models: A comparison of various antidotes with early surgical treatment in rat models found that early surgical debridement was the most effective modality in decreasing the size of vesicant ulcers and speeding the healing of those ulcers.
WRINGER AND ROLLER CRUSH INJURIES
The term wringer injury was first used by MacCollum in 1938 to designate a specific crushing injury of the upper extremity caused by its passage between the rollers of the wringer on an electric washing machine. While vintage washing machines are obsolete, similar injuries continue to occur frequently in industrial workers caught in conveyor belts, printing presses, and industrial rollers.
Biomechanics of Wringer Injuries
Wringer injuries are complex because they combine three distinct destructive forces:
1. Compression: Direct crushing of the skin, subcutaneous fat, and muscle.
2. Shear: As the limb is pulled through the rollers, the skin and subcutaneous tissues are violently sheared away from the underlying deep fascia, creating massive potential spaces (Morel-Lavallée lesions) that rapidly fill with hematoma and serous fluid.
3. Friction Burns: If the injury is severe, the skin and deep tissues are burned by the spinning rollers. This often occurs at one specific level where the extremity is physically blocked from entering farther between the rollers. Common anatomical block points include the base of the thumb, the antecubital fossa, or the axilla.
Surgical Warning: Some of the most severe skin avulsions in wringer injuries are actually iatrogenic to the patient—caused by the patient’s vigorous, panicked attempts to forcefully free the limb while the rollers are still in motion.
Clinical Evaluation and the "Delayed Swelling" Phenomenon
Early examination of a wringer injury is notoriously treacherous. Initial presentation may reveal only superficial abrasions, minor tears of the skin, or occasionally a fracture.
This first examination often is misleading, however, because severe swelling caused by deep hemorrhage and reactive edema may occur hours later. The sheer forces strip the perforating vessels, leading to delayed full-thickness skin necrosis that may not become clinically apparent for 48 to 72 hours.
Management Protocol
The management of wringer injuries relies heavily on aggressive compression, strict elevation, and vigilant monitoring for compartment syndrome.
- Initial Resuscitation and Cleaning: The limb is thoroughly cleaned with soap and water. Any open wounds or frank avulsions are debrided of gross contamination and either closed loosely or left open for delayed closure or skin grafting.
- The Pressure Dressing: A meticulously applied pressure dressing is the cornerstone of conservative management. It must include the entire hand and arm, with extreme care taken to distribute the pressure evenly to prevent venous congestion.
- Layer 1: The area is covered by finely woven, nonadherent gauze.
- Layer 2: Flat gauze pads are applied over the nonadherent layer.
- Layer 3: Large masses of cotton are applied to provide bulky, soft padding.
- Layer 4: An elastic bandage is rolled on evenly from distal to proximal.
- Elevation and Monitoring: The extremity is elevated above the level of the heart and is kept so throughout treatment.
- Serial Examinations: At 24 hours, the dressing is removed. The wound is meticulously inspected for the development of blisters, expanding hematomas, and early signs of skin necrosis. The dressing is then reapplied. This process is repeated every 24 hours until the soft tissue envelope becomes stabilized.
- Surgical Intervention: If necessary, any devitalized tissue identified during serial exams is excised, hematomas are evacuated to prevent secondary infection, and the wound is closed appropriately via skin grafting or local flap coverage once the wound bed is healthy.
CONCLUSION
Injection, extravasation, and wringer injuries of the upper extremity demand a high index of suspicion and a low threshold for surgical intervention. The deceptively benign initial presentation of high-pressure injection injuries masks a limb-threatening emergency that requires immediate, wide surgical decompression and meticulous debridement. Similarly, extravasation and wringer injuries require vigilant observation for delayed necrosis and compartment syndrome. By adhering to strict protocols of early surgical debridement, appropriate use of advanced adjuncts like fluorescein demarcation, and rigorous postoperative compression and elevation, the orthopedic surgeon can salvage limb function and prevent the devastating sequelae of these complex soft tissue traumas.
You Might Also Like