Advanced Management of Femoral Neck Fractures: Capsulotomy, Fixation, and Arthroplasty
Key Takeaway
The management of displaced femoral neck fractures requires a nuanced understanding of hip biomechanics, vascular anatomy, and patient-specific physiological demands. This comprehensive guide details the surgical technique for fluoroscopically guided hip capsulotomy to mitigate intracapsular pressure and prevent osteonecrosis. Furthermore, it provides an evidence-based analysis of internal fixation complications and the critical decision-making matrix for selecting between total hip arthroplasty and hemiarthroplasty in the geriatric population.
INTRODUCTION TO FEMORAL NECK FRACTURE MANAGEMENT
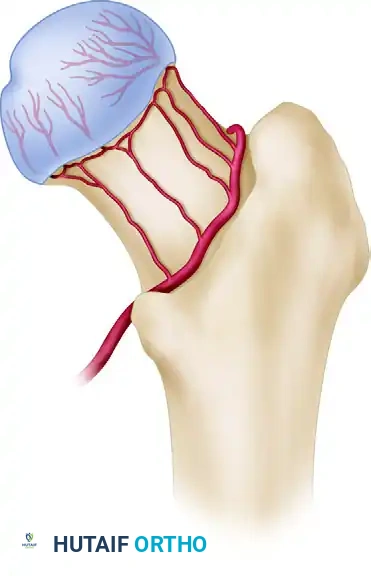
The management of femoral neck fractures remains one of the most rigorously debated topics in orthopedic traumatology. Often referred to as the "unsolved fracture," the femoral neck presents unique biomechanical and biological challenges. The precarious blood supply to the femoral head—primarily derived from the medial circumflex femoral artery (MCFA) and its lateral epiphyseal branches—renders the femoral head highly susceptible to osteonecrosis (avascular necrosis, AVN) following displacement.
Furthermore, the intracapsular nature of these fractures means that fracture hematoma can lead to a significant rise in intracapsular pressure, creating a tamponade effect that further compromises retinacular perfusion. Consequently, joint-preserving procedures such as internal fixation must often be accompanied by a capsulotomy to decompress the joint. Conversely, in the physiologically older population, the unacceptably high rates of fixation failure have driven a paradigm shift toward primary arthroplasty.
This masterclass provides an exhaustive, evidence-based review of fluoroscopically guided capsulotomy, the complications associated with internal fixation, and the contemporary controversies surrounding arthroplasty for displaced femoral neck fractures.
FLUOROSCOPICALLY GUIDED CAPSULOTOMY OF THE HIP
The rationale for performing a capsulotomy after the internal fixation of a femoral neck fracture is rooted in the preservation of the femoral head's vascularity. An intracapsular hematoma can elevate intra-articular pressure above the capillary perfusion pressure of the retinacular vessels, leading to ischemic necrosis of the femoral head.
Christa et al. demonstrated in a landmark cadaveric series that fluoroscopically guided capsulotomy is both safe and highly effective at decreasing intracapsular pressure. Their post-capsulotomy dissections provided critical anatomical safety parameters:
* Femoral Artery: The average distance from the capsulotomy site to the femoral artery was 40.3 mm (absolute minimum distance observed: 36 mm).
* Femoral Nerve: The average distance to the lateralmost branch of the femoral nerve was 19.5 mm (absolute minimum distance observed: 15 mm).
These anatomical metrics confirm that when performed correctly, a closed, fluoroscopically guided capsulotomy carries a minimal risk of iatrogenic neurovascular injury while substantially decreasing intracapsular pressure.
Surgical Technique: Step-by-Step Capsulotomy
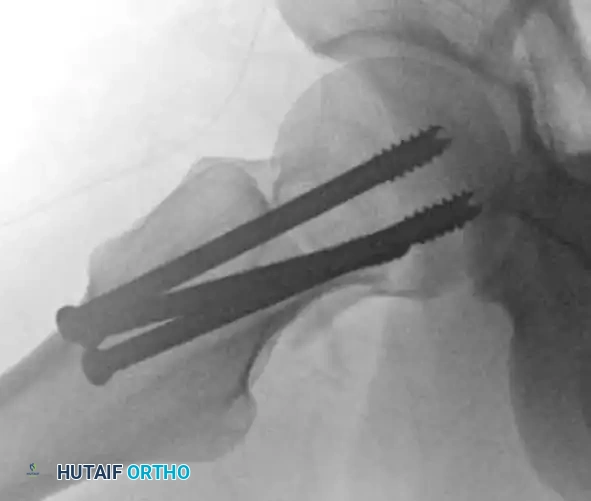
The following technique should be executed immediately following the definitive fixation of the femoral neck fracture (e.g., via cannulated screws, a compression hip screw, or a proximal femoral locking plate).
Surgical Pearl: Instrument Preparation
Before introducing the scalpel into the soft tissues, prepare a No. 10 scalpel blade by wrapping an approximately 2-cm strip of Ioban (antimicrobial incise drape) tightly around the blade/handle junction. This critical step drastically decreases the likelihood of the blade dissociating from the handle and being retained within the deep tissues of the thigh.
- Incision Utilization: Utilize the same lateral approach incision that was created for the insertion of your fixation hardware.
- Instrument Insertion: Introduce the prepared No. 10 scalpel through the lateral incision.
- Trajectory and Advancement: Using a combination of tactile feedback and continuous orthogonal fluoroscopic guidance, advance the scalpel along the anterior cortex of the femoral neck. The sharp edge of the blade must be directed inferiorly to avoid inadvertent superior retinacular vessel injury.
- Capsular Release: Once the tactile sensation of the femoral head is encountered (confirming the blade has traversed the capsule), rotate the scalpel blade 90 degrees.
- Withdrawal: Withdraw the scalpel utilizing a firm, posteriorly directed force. This motion effectively slices through the robust anterior iliofemoral ligament and capsule, completing the capsulotomy and allowing the immediate egress of the fracture hematoma.
COMPLICATIONS OF INTERNAL FIXATION
While anatomical reduction and stable internal fixation remain the gold standard for physiologically young patients (typically defined as < 65 years of age), the complication profile in older cohorts is substantial.
A comprehensive meta-analysis encompassing 106 reports of displaced femoral neck fractures in patients aged 65 years or older revealed alarming failure rates:
* Osteonecrosis (AVN): 16% overall rate.
* Nonunion: 33% overall rate.
* Reoperation Rate: Ranged from 20% to 36% within the first 2 years post-operation.
These reoperation rates are significantly higher than those observed following primary hemiarthroplasty or total hip arthroplasty (THA). Failures are frequently attributed to poor bone quality (osteoporosis), comminution of the calcar, and the inability of the patient to comply with restricted weight-bearing protocols.
Malreduction and Deformity
Failure to achieve an anatomical or slightly valgus reduction inevitably leads to altered biomechanics, increased shear forces across the fracture site, and subsequent hardware failure.
Varus malreduction is particularly detrimental, as it converts compressive forces into shear forces, leading to screw cut-out and nonunion.
Figure: Anteroposterior radiograph demonstrating a severe varus malreduction of a femoral neck fracture following initial cannulated screw fixation.
Similarly, an apex posterior deformity alters the version of the femoral neck, compromising the retinacular blood supply and leading to early mechanical failure.

Figure: Lateral radiograph illustrating an apex posterior deformity, a common pitfall in the reduction of displaced femoral neck fractures.
When malreduction is identified early in a physiologically robust patient, revision open reduction and internal fixation (ORIF) may be attempted, often utilizing more rigid constructs such as proximal femoral locking plates to achieve absolute stability.

Figure: Postoperative radiograph following revision ORIF, demonstrating improved alignment.

Figure: Orthogonal view of the revision ORIF utilizing a fixed-angle device to prevent recurrent varus collapse.
Management of Nonunion
Nonunion of the femoral neck presents a complex reconstructive challenge. Patients typically present with persistent groin pain and a limb length discrepancy.

Figure: Anteroposterior radiograph revealing an established nonunion of the femoral neck with hardware failure and backing out of the cannulated screws.
Advanced imaging, particularly a fine-cut Computed Tomography (CT) scan, is essential to evaluate the extent of bone resorption, the presence of avascular necrosis, and the remaining bone stock available for revision fixation.

Figure: Axial CT scan confirming the lack of bridging trabeculae and the presence of a fibrous nonunion at the femoral neck.
In highly selected, physiologically young patients with a viable femoral head (no evidence of AVN on MRI), joint-preserving salvage procedures can be attempted. Valgus-producing proximal femoral osteotomies, stabilized with a fixed-angle blade plate, reorient the fracture line perpendicular to the joint reaction force, converting shear forces into compressive forces to stimulate union.

Figure: Successful union achieved after revision surgery utilizing a valgus-producing osteotomy and fixation with a 130-degree blade plate.
Surgical Warning: Patient Selection for Salvage
Attempting a valgus-producing osteotomy in a patient over the age of 65 or in a patient with any radiographic evidence of femoral head collapse is contraindicated. In these scenarios, conversion to a Total Hip Arthroplasty is the definitive and most reliable treatment.
ARTHROPLASTY FOR DISPLACED FEMORAL NECK FRACTURES
The decision matrix for proceeding with internal fixation versus arthroplasty hinges primarily on fracture characteristics (displaced vs. nondisplaced) and the physiological age of the patient.
As a strict orthopedic doctrine:
* Young Patients (< 65 years): Require emergent anatomical reduction and stable internal fixation to preserve the native joint.
* Older Patients (> 65 years): Displaced fractures should be treated with primary arthroplasty.
A high-quality meta-analysis incorporating nine randomized controlled trials (RCTs) definitively showed that arthroplasty substantially reduces the risk of revision surgery compared with internal fixation in patients aged 65 years or older. However, surgeons must counsel patients that arthroplasty is a more physiologically demanding procedure, associated with greater intraoperative blood loss, longer operative times, and a slightly higher frequency of deep surgical site infections.
The Rogmark et al. Landmark Trial
The superiority of arthroplasty in the elderly was cemented by the randomized trial conducted by Rogmark et al., which compared internal fixation and arthroplasty for displaced femoral neck fractures in ambulatory patients aged 70 years or older.
- 2-Year Outcomes: Failure (defined as early fracture displacement, nonunion, osteonecrosis with collapse, or deep infection) occurred in a staggering 43% of patients treated with internal fixation, compared to only 6% of those treated with arthroplasty.
- 10-Year Follow-up: A subsequent longitudinal study of the same cohort revealed that these results were stable over time. At no point during the 10-year follow-up did patients with "successful" internal fixation display better outcomes regarding hip pain or mobility than patients with successful arthroplasty.
CONTROVERSIES IN ARTHROPLASTY: THA VS. HEMIARTHROPLASTY
Once the decision has been made to proceed with arthroplasty, the orthopedic surgeon must navigate several controversial variables to optimize patient outcomes. The primary debate centers on the type of arthroplasty: Total Hip Arthroplasty (THA) versus Hemiarthroplasty.
Hemiarthroplasty
Hemiarthroplasty involves replacing only the femoral head, allowing the prosthetic head to articulate directly with the native acetabular cartilage.
* Indications: Typically reserved for older, lower-demand patients, household ambulators, or those with significant cognitive impairment (e.g., advanced dementia) or severe neuromuscular comorbidities.
* Unipolar vs. Bipolar: Bipolar prostheses feature an additional inner articulation, theoretically reducing acetabular wear. However, long-term studies show minimal clinical difference between unipolar and bipolar designs regarding pain or functional outcomes, though bipolar implants are significantly more expensive.
* Advantages: Shorter operative time, less blood loss, and a lower risk of dislocation compared to THA.
* Disadvantages: Risk of progressive acetabular wear (protrusio acetabuli) and persistent groin pain.
Total Hip Arthroplasty (THA)
Historically, THA was rarely performed for acute femoral neck fractures due to concerns over dislocation and surgical magnitude. However, the modern consensus has shifted dramatically. The debate over whether THA is superior to hemiarthroplasty for displaced femoral neck fractures in active, physiologically older patients has intensified, with recent literature heavily favoring THA.
- Indications: Active, community ambulators with a life expectancy greater than 5 years, and patients with pre-existing symptomatic osteoarthritis of the ipsilateral hip.
- Benefits of THA:
- Superior functional outcome scores (e.g., Harris Hip Score).
- Significantly decreased long-term groin pain (as the native acetabulum is resurfaced).
- Improved ambulation and gait mechanics.
- Lower long-term reoperation rates (eliminates the risk of acetabular erosion).
- Disadvantages of THA: The primary drawback is a slightly higher dislocation rate compared to hemiarthroplasty. This risk can be mitigated by utilizing larger femoral heads (e.g., 32mm or 36mm), dual-mobility articulations, and meticulous repair of the posterior capsule if a posterior approach is utilized.
Additional Surgical Considerations
Cemented vs. Uncemented Femoral Stems:
In the osteoporotic bone typical of geriatric femoral neck fracture patients, cemented femoral stems are generally preferred. Uncemented stems in this population carry a higher risk of intraoperative periprosthetic femur fractures (up to 10-14% in some registries) and postoperative subsidence. Cemented stems provide immediate rigid fixation, allowing for unrestricted weight-bearing. Surgeons must, however, be vigilant regarding Bone Cement Implantation Syndrome (BCIS) during pressurization.
Surgical Approach:
The choice of surgical approach (Posterior, Anterolateral, or Direct Anterior) should be based on surgeon familiarity and patient anatomy.
* Posterior Approach: Offers excellent exposure but historically carries a higher dislocation risk. This is mitigated by a robust enhanced soft-tissue repair.
* Anterolateral Approach: Lower dislocation risk but carries a risk of superior gluteal nerve injury and postoperative abductor weakness (Trendelenburg gait).
* Direct Anterior Approach (DAA): Increasingly popular due to its internervous and intermuscular plane, potentially offering faster early rehabilitation and lower dislocation rates, though it carries a steeper learning curve and risk of lateral femoral cutaneous nerve neuropraxia.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
Regardless of whether internal fixation or arthroplasty is performed, the overarching goal in the geriatric population is immediate mobilization to prevent the cascade of complications associated with prolonged bed rest (e.g., deep vein thrombosis, pulmonary embolism, decubitus ulcers, and pneumonia).
- Weight-Bearing Status: Patients treated with arthroplasty (especially cemented constructs) should be allowed weight-bearing as tolerated (WBAT) immediately postoperatively. Patients treated with internal fixation are also generally allowed WBAT, as restricting weight-bearing in the elderly is practically impossible and leads to deconditioning.
- Thromboembolic Prophylaxis: Chemical prophylaxis (e.g., Low Molecular Weight Heparin, Direct Oral Anticoagulants, or Aspirin, depending on risk stratification) combined with mechanical prophylaxis (SCDs) is mandatory for a minimum of 28 to 35 days postoperatively.
- Dislocation Precautions: For patients undergoing THA or hemiarthroplasty via a posterior approach, standard posterior hip precautions (avoiding flexion past 90 degrees, adduction across the midline, and internal rotation) should be maintained for 6 weeks to allow capsular healing.
CONCLUSION
The successful management of femoral neck fractures demands a highly individualized approach. For the young patient, meticulous anatomical reduction, stable internal fixation, and joint decompression via fluoroscopically guided capsulotomy are paramount to preserving the native hip and preventing osteonecrosis. For the physiologically older patient, the literature unequivocally supports arthroplasty over internal fixation. By carefully selecting between hemiarthroplasty and total hip arthroplasty based on the patient's functional demands and life expectancy, orthopedic surgeons can optimize mobility, minimize pain, and significantly reduce the burden of revision surgeries.
📚 Medical References
- femoral neck fractures: a new low posterior approach (the southern exposure), AAOS Instr Course Lect 16:309, 1959.
- Osborne RP: The approach to the hip-joint: a critical review and a suggested new route, Br J Surg 18:49, 1930–1931.
- Schaubel HJ: Modifi cation of the anterior iliofemoral approach to the hip, Int Surg 65:347, 1980.
- Smith-Petersen MN: A new supra-articular subperiosteal approach to the hip joint, Am J Orthop Surg 15:592, 1917.
- Smith-Petersen MN: Approach to and exposure of the hip joint for mold arthroplasty, J Bone Joint Surg 31A:40, 1949.
- Somerville EW: Open reduction in congenital dislocation of the hip, J Bone Joint Surg 35B:363, 1953.
- Testa NN, Mazur KU: Heterotopic ossification after direct lateral approach and transtrochanteric approach to the hip, Orthop Rev 17:965, 1988.
- Watson-Jones R: Fractures of the neck of the femur, Br J Surg 23:787, 1935–1936.
- Acetabulum and Pelvis Carnesale PG: Personal communication, 1977.
- Charnley J, Ferriera A, De SO: Transplantation of the greater trochanter in arthroplasty of the hip, J Bone Joint Surg 46B:191, 1964.
- Krackow KA, Steinmann H, Cohn BT, et al: Clinical experience with the triradiate exposure of the hip for diffi cult
You Might Also Like