Thoracic Disc Disease: Surgical Approaches & Management
Key Takeaway
Thoracic disc disease is a rare but potentially debilitating condition. While most cases resolve with conservative management, progressive myelopathy or intractable radiculopathy necessitates surgical intervention. Due to the narrow thoracic canal and kyphotic alignment, simple posterior laminectomy is strictly contraindicated. Safe surgical management requires specialized posterolateral approaches, such as costotransversectomy, or anterior transthoracic decompression to adequately visualize and resect the pathology without manipulating the vulnerable spinal cord.
THORACIC DISC DISEASE: EPIDEMIOLOGY AND PATHOPHYSIOLOGY
The thoracic spine is the least common location for clinically significant intervertebral disc pathology. Symptomatic thoracic disc herniations remain exceedingly rare, with an estimated incidence of one in 1 million individuals per year, representing merely 0.25% to 0.75% of the total incidence of all symptomatic disc herniations. The most common age of onset spans the fourth and sixth decades of life.
Despite the rarity of symptomatic presentations, the incidence of asymptomatic thoracic disc herniations is remarkably high. In a landmark study, Wood et al. reviewed magnetic resonance imaging (MRI) studies in 90 asymptomatic patients and discovered thoracic disc abnormalities in 73% of the cohort. Of these, 37% had frank herniations, and 29% demonstrated radiographic evidence of spinal cord compression without clinical myelopathy. At a mean follow-up of 26 months with repeat MRI, none of these patients had become symptomatic. Furthermore, Wood et al. observed a paradoxical natural history: small herniations often increased in size over time, whereas larger herniations frequently regressed.
Biomechanics and Surgical Anatomy
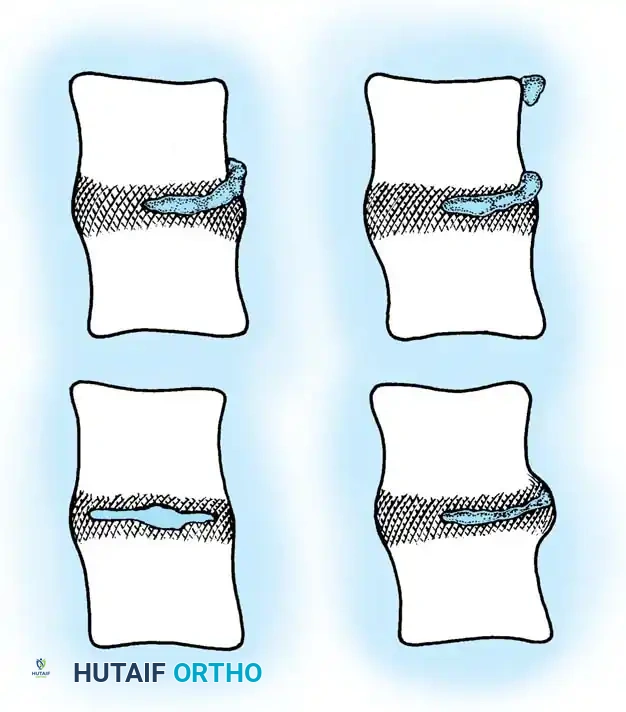
Understanding the unique biomechanics and anatomy of the thoracic spine is critical for surgical decision-making. The thoracic spine features a natural kyphosis, which inherently drapes the spinal cord anteriorly against the posterior longitudinal ligament (PLL) and the posterior aspect of the intervertebral discs. Consequently, any anterior space-occupying lesion (such as a herniated disc or osteophyte) directly compresses the ventral cord.
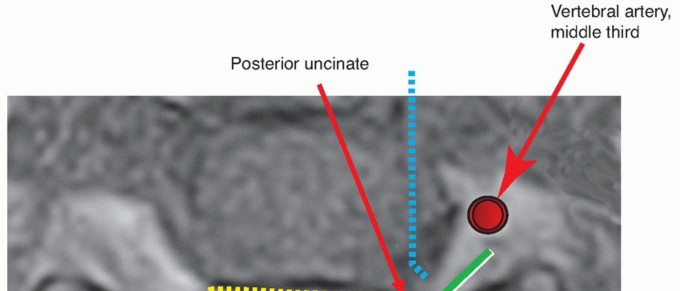
Furthermore, the thoracic spinal canal is narrowest between T4 and T9, leaving minimal reserve for the spinal cord. The vascular supply to the thoracic cord is also precarious; the midthoracic region represents a vascular watershed zone. The Artery of Adamkiewicz, which provides the primary arterial supply to the lower anterior spinal cord, typically arises between T9 and L2 (most commonly on the left side). Surgical approaches must meticulously respect this vascular anatomy to prevent catastrophic postoperative paraplegia secondary to cord ischemia.
CLINICAL PRESENTATION AND EVALUATION
The natural history of symptomatic thoracic disc disease mirrors that of other spinal regions; symptoms and functional deficits typically improve with conservative treatment and time. However, the clinical course can be highly variable, necessitating a high index of suspicion to establish the correct diagnosis.
Differential Diagnosis
The differential diagnosis for thoracic disc herniation is extensive and includes non-spinal etiologies across multiple organ systems:
* Cardiopulmonary: Myocardial infarction, angina pectoris, pericarditis, pulmonary embolism.
* Gastrointestinal: Cholecystitis, peptic ulcer disease, pancreatitis.
* Musculoskeletal: Intercostal neuralgia, costochondritis, rib fractures.
* Spinal: Infectious (discitis/osteomyelitis), neoplastic (primary or metastatic tumors), degenerative, and metabolic disorders.
Patient Populations
Two distinct patient populations emerge in the literature:
1. Acute/Traumatic (Younger Cohort): A smaller group of younger patients presenting with a relatively short history of symptoms, often precipitated by trauma. They typically exhibit an acute soft disc herniation causing acute spinal cord compression or radiculopathy. Outcomes are generally highly favorable with either operative or nonoperative treatment.
2. Chronic/Degenerative (Older Cohort): A larger group of patients with a prolonged history (often >6 to 12 months) of symptoms resulting from chronic spinal cord or nerve root compression. The underlying pathophysiology is disc degeneration, frequently accompanied by dense calcification of the herniated disc fragment.
Signs and Symptoms
Pain is the most ubiquitous presenting feature. Two distinct pain patterns are clinically apparent:
1. Axial Pain: Localized to the thoracic spine.
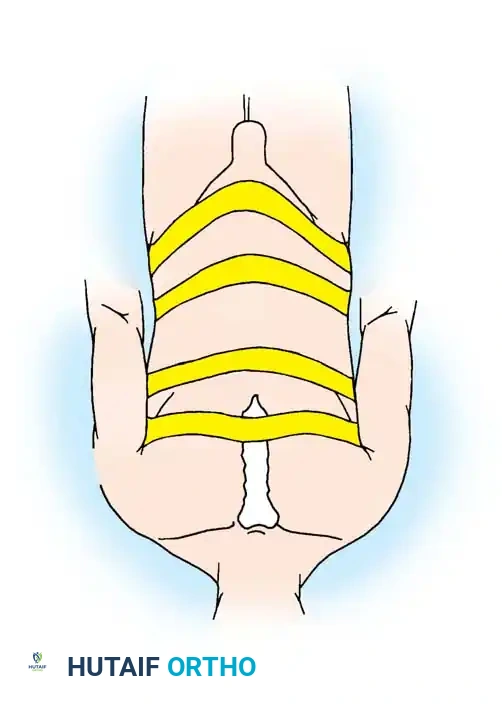
2. Radicular Pain: A bandlike, burning, or shooting pain radiating along the course of the intercostal nerve.
The T10 dermatomal level is the most commonly reported distribution, regardless of the actual level of involvement. This manifests as a band extending around the lower lateral thorax and caudally to the level of the umbilicus. This radicular pattern is more prevalent with upper thoracic and lateral disc herniations. Associated sensory changes, including paresthesias and dysesthesias in a dermatomal distribution, are frequent.
High thoracic discs (T2 to T5) can mimic cervical disc disease, presenting with upper extremity pain, paresthesias, radiculopathy, and occasionally Horner syndrome (due to disruption of the sympathetic chain).
Myelopathy is a severe manifestation. Patients may complain of generalized weakness, typically involving both lower extremities in the form of mild paraparesis. Objective signs of myelopathy include sustained clonus, a positive Babinski sign, hyperreflexia, and a wide-based, spastic gait. Bowel and bladder dysfunction are late findings, occurring in only 15% to 20% of patients.
💡 Clinical Pearl: The Neurological Examination
The neurological evaluation of patients with suspected thoracic disc herniations must be meticulous due to the paucity of localizing findings. Assess abdominal reflexes, the cremasteric reflex, dermatomal sensory levels, rectus abdominis contraction symmetry (Beevor's sign), lower extremity reflexes, motor strength, and long tract signs.
CONFIRMATORY IMAGING
- Magnetic Resonance Imaging (MRI): MRI is the gold standard and the most useful imaging modality for demonstrating thoracic disc herniations. It effectively delineates intradural pathology, disc fragments, and spinal cord signal changes (indicating inflammation, edema, or myelomalacia). However, MRI may underestimate the true size of a thoracic disc herniation if the fragment is heavily calcified, as calcifications exhibit low signal intensity on both T1 and T2 sequences.
- Computed Tomography (CT) Myelography: Highly useful for evaluating bony anatomy and accurately assessing the calcified portion of a herniated thoracic disc. It is often utilized when MRI is contraindicated or when surgical planning requires precise mapping of a calcified mass.
- Plain Radiographs: Helpful for evaluating traumatic injuries, identifying osseous morphological variations, and localizing the correct level on intraoperative fluoroscopy.
TREATMENT ALGORITHM AND RESULTS
Nonoperative Management
Conservative treatment is highly effective for the majority of patients. Brown reported that 63% of patients improved using a combination of nonoperative modalities. While a universal regimen cannot be prescribed, the core principles include:
* Short-term rest or activity modification.
* Pharmacologic pain relief (NSAIDs, gabapentinoids, muscle relaxants).
* Progressive, directed physical therapy and core stabilization.
These measures should generally be exhausted for at least 6 to 12 weeks before considering surgical intervention, provided the patient remains neurologically stable.
Indications for Surgery
Operative treatment is indicated in rare patients presenting with:
1. Acute disc herniation with progressive myelopathic findings.
2. Progressive neurological deficits (motor weakness).
3. Intractable, debilitating radicular or axial pain that fails comprehensive conservative management.
Evolution of Surgical Outcomes
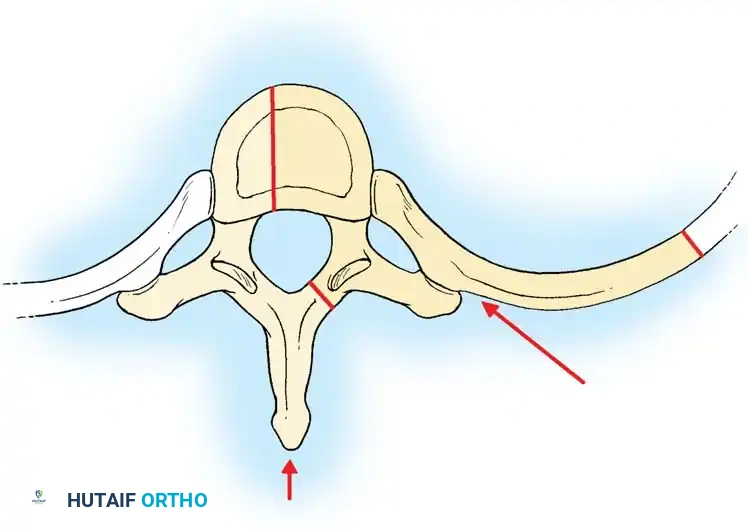
Historically, the initial procedure recommended for thoracic disc herniations was a posterior thoracic laminectomy. Because at least half of these lesions are central, attempting to excise a ventral mass via a posterior approach required dangerous retraction of the thoracic spinal cord. The results were disastrous; most series reported fewer than half of the patients improving, with a significant percentage suffering catastrophic neurological worsening (paraplegia) postoperatively.
🚨 Surgical Warning: The Laminectomy Contraindication
Simple posterior laminectomy has no role in the surgical treatment of thoracic disc herniations. It is strictly contraindicated due to the unacceptably high risk of spinal cord injury.
Modern literature confirms that lateral rachiotomy (modified costotransversectomy) or anterior transthoracic approaches yield vastly superior results with minimal risk of neurological worsening. Bohlman and Zdeblick reported on anterior thoracic disc excision in 19 patients: 16 achieved excellent or good results, pain was relieved or decreased in 18, and zero patients experienced neurological worsening. Video-assisted thoracic surgery (VATS) has also emerged as a viable minimally invasive alternative; Regan, Ben-Yishay, and Mack reported a series of 29 thoracoscopic disc excisions with 76% satisfactory results.
OPERATIVE TREATMENT: SURGICAL APPROACHES
The optimal surgical approach depends entirely on the specific characteristics of the disc herniation (central vs. lateral, soft vs. calcified) and the surgeon's expertise.
(Above: Standard Laminectomy - Contraindicated for thoracic disc herniation)
Posterolateral Approaches
Posterolateral approaches avoid the morbidity of a thoracotomy while providing safe access to the lateral aspect of the ventral spinal canal.
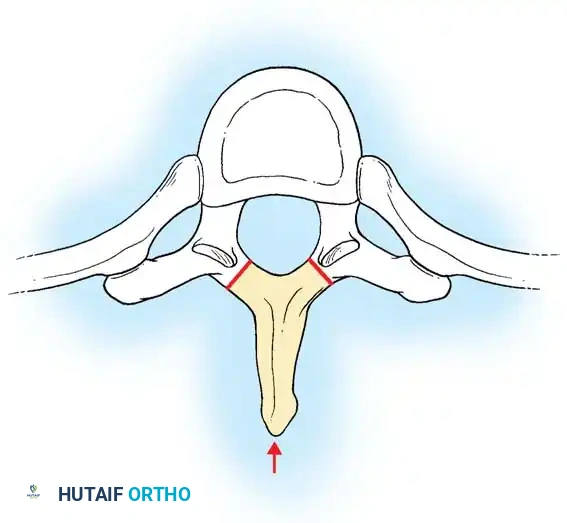
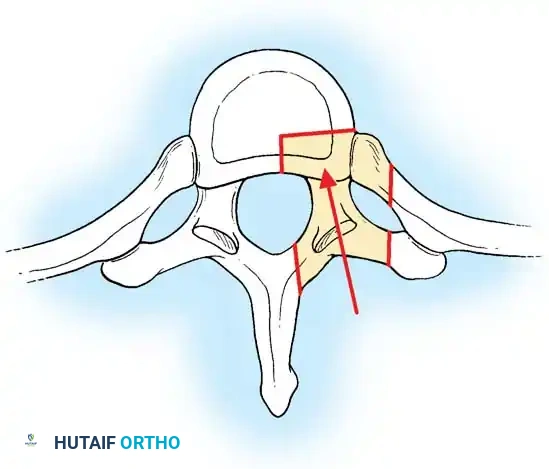
1. Transpedicular Approach
Useful for soft, lateral herniations. It involves removing the facet joint and pedicle to access the lateral disc space without manipulating the cord.
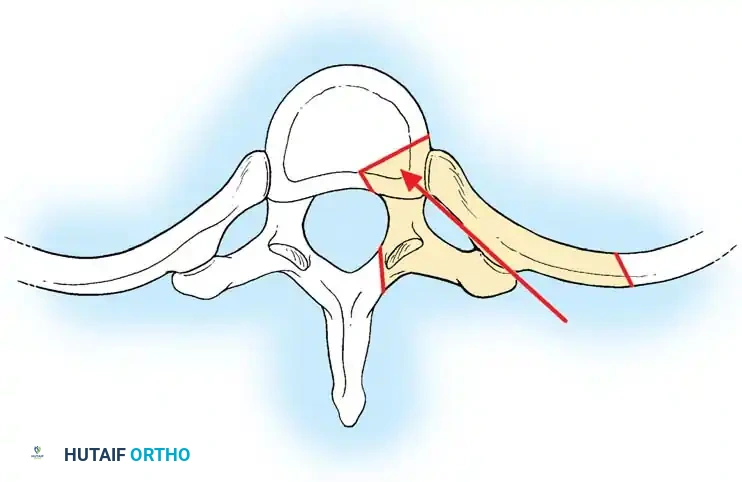
2. Costotransversectomy
Costotransversectomy is best suited for thoracic disc herniations that are predominantly lateral, or herniations suspected to be extruded or sequestered.
🔪 Surgical Technique: Costotransversectomy
- Anesthesia & Positioning: The operation is performed under general anesthesia. A double-lumen endotracheal tube (or Carlen tube) is highly recommended to allow selective lung deflation on the operative side, minimizing pleural injury. Place the patient prone on a Jackson table with chest rolls to free the abdomen.
- Incision: Make a long midline incision or a paramedian curved incision (convex to the midline) centered over the side of involvement.
- Exposure: Dissect the paraspinal musculature laterally to expose the posterior elements, facet joints, transverse processes, and the medial aspect of the ribs.
- Rib Resection: Remove a section of the rib, approximately 5 to 7.5 cm long, at the level of involvement. Surgical Pitfall: Meticulously dissect the periosteum to avoid damaging the underlying intercostal nerve and artery.
- Disc Exposure: Carry the resection medially into the lateral side of the disc space. The transverse process and the head of the rib articulating with the disc space are removed.
- Decompression: Additional exposure can be achieved by a partial hemilaminectomy and excision of the pedicle and facet joint. Remove the lateral disc fragment using down-pushing curettes and pituitary rongeurs.
- Fusion Considerations: Fusion is generally unnecessary unless more than one facet joint or pedicle is completely resected, which may destabilize the segment.
- Closure: Close the wound in deep anatomical layers to prevent dead space and hematoma formation.
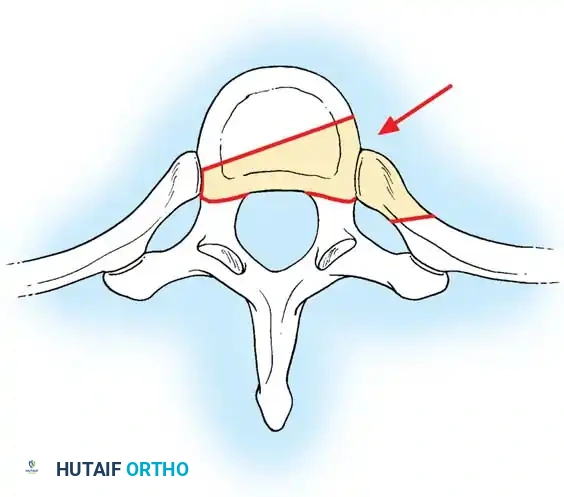
3. Lateral Extracavitary Approach
Provides a more ventral trajectory than the costotransversectomy by resecting a larger portion of the rib and mobilizing the paraspinal muscles medially.
Anterior Approaches
Anterior approaches (via thoracotomy, transsternal, or VATS) are the gold standard for central, broad-based, or heavily calcified thoracic disc herniations. They provide direct, orthogonal visualization of the ventral dural sac.
Anterior Transthoracic Approach for Disc Excision
Because patients with degenerative thoracic discs are often older, preoperative pulmonary function testing is essential. In patients with severe pulmonary compromise, an anterior approach may be medically detrimental, making a posterolateral approach safer. However, for midline calcified protrusions, the transthoracic approach ensures complete, safe disc removal.
🔪 Surgical Technique: Anterior Transthoracic Approach
- Anesthesia: General anesthesia utilizing a double-lumen endotracheal tube for selective lung deflation on the side of the approach.
- Positioning: Place the patient in a true lateral decubitus position. A left-sided approach is generally preferred (especially for central herniations) as it avoids the friable liver and the thin-walled inferior vena cava, dealing instead with the more robust aorta.
- Incision: Make a skin incision along the line of the rib corresponding to the second thoracic vertebra above the involved intervertebral disc. For approaches to the upper five thoracic segments, the approach is typically through the third rib bed. Confirm the level with intraoperative fluoroscopy before incision.
- Rib Resection: Cut the rib subperiosteally at its posterior and anterior ends. Insert a rib retractor. Save the resected rib for use as an interbody structural graft later in the procedure. The approach can be extrapleural or transpleural, depending on surgeon familiarity.
- Vascular Mobilization: Dissect the great vessels (aorta) free from the anterior spine. Ligate the segmental vessels near the great vessels, not near the neural foramen, to preserve collateral flow. Critical Rule: Do not disturb more than three segmental vessels to avoid ischemic complications to the spinal cord (Artery of Adamkiewicz).
- Diaphragmatic Takedown (Thoracolumbar Junction): In the thoracolumbar region (T11-L1), strip the crus of the diaphragm from the 11th and 12th ribs.
- Discectomy: Section the anterior longitudinal ligament (ALL) to allow spreading of the intervertebral disc space. Remove the anterior two-thirds of the disc using standard curettes and rongeurs.
- Microscopic Decompression: Use an operating microscope or high-powered loupe magnification for the posterior third of the disc near the PLL and dura. If the herniation is calcified, use a high-speed burr to thin the disc and osteophytes down to a thin cortical shell. Surgical Pearl: Even if a drill is used, the removal of the posterior-most tissue directly compressing the ventral dura must be done with hand instruments (blunt Penfield dissectors, micro-curettes) to prevent dural tears or cord injury.
- Managing the PLL and Epidural Space:
- Excise the posterior longitudinal ligament only in selected cases. It is unlikely that a hidden ruptured disc fragment is present without prior disruption of this ligament.
- Removal of the PLL is the most difficult part of the procedure and is often complicated by brisk epidural venous bleeding. If the ligament is left intact, the procedure is simpler and shorter.
- If epidural bleeding occurs, use bipolar coagulation. Warning: To avoid compressive material contacting the spinal cord, do not pack the canal with expansile hemostatic agents (e.g., Gelfoam or Surgicel) if they cannot be fully retrieved.
- Grafting and Fusion: After complete decompression, strip the cartilaginous endplates to bleeding subchondral bone. Make a slot on the margin of the superior endplate to accept the graft. Insert the autologous rib graft, iliac crest, or a structural allograft/cage into the disc space.
- Closure: For standard thoracotomies, place a chest tube, reapproximate the ribs, and close the muscle layers. (Note: If approaching a high T1-T2 disc via a low anterior cervical/supraclavicular approach, close the platysma with interrupted 3-0 absorbable stitches, and approximate the skin with subcuticular sutures). Inject local anesthetic subcutaneously to minimize postoperative incisional pain.
Postoperative Protocol
Postoperative care is heavily dictated by the surgical approach. For anterior transthoracic procedures:
* Chest Tube Management: The patient is monitored in an intensive or step-down unit. Chest tubes are placed to water seal and suction. Daily chest radiographs are obtained to monitor lung expansion and rule out hemothorax/pneumothorax.
* Mobilization: The patient is rapidly mobilized out of bed as tolerated by the chest tubes. Early ambulation prevents pulmonary complications and deep vein thrombosis.
* Discharge: Discharge is typically possible 24 to 48 hours after the chest tubes have been removed, provided the patient is ambulating well, pain is controlled, and bowel/bladder function is normal.
* Bracing: Depending on the extent of bony resection and the stability of the interbody fusion, a rigid thoracic orthosis (TLSO) may be prescribed for 6 to 12 weeks to promote arthrodesis.
You Might Also Like