Lumbar and Thoracic Intervertebral Disc Disease: Comprehensive Surgical Management
Key Takeaway
Intervertebral disc disease frequently presents in the third and fourth decades of life, characterized by radicular pain and neurological deficits. This guide provides an evidence-based overview of lumbar and thoracic disc herniations, detailing pathomechanics, clinical evaluation, and advanced surgical interventions. Step-by-step protocols for open transthoracic approaches and video-assisted thoracoscopic surgery (VATS) are thoroughly examined to optimize patient outcomes and surgical precision.
Lumbar and Thoracic Intervertebral Disc Disease: Pathomechanics and Clinical Presentation
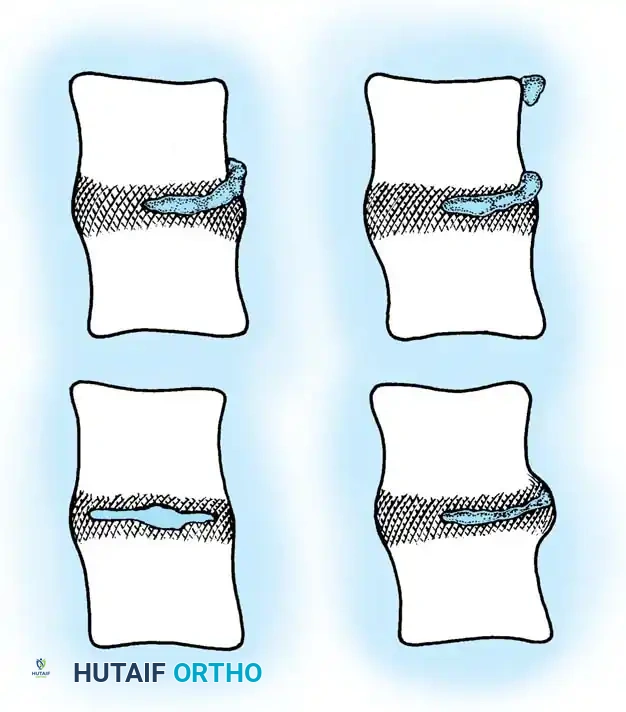
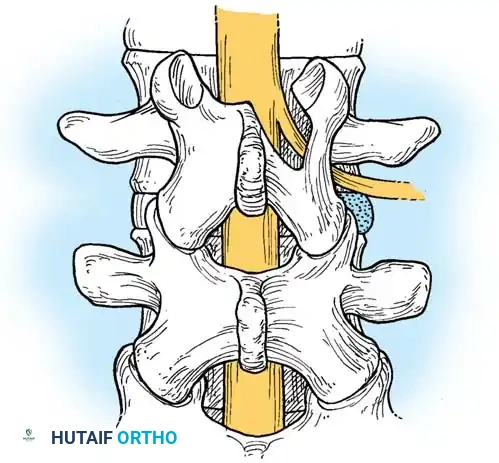
Although axial back pain is a ubiquitous complaint from the second decade of life onward, symptomatic intervertebral disc disease and frank disc herniation are most prominent in otherwise healthy individuals during their third and fourth decades. The pathophysiology of lumbar disc disease is characterized by a continuum of degenerative cascades, often culminating in the mechanical extrusion of the nucleus pulposus through a compromised annulus fibrosus.
Most patients retrospectively correlate the onset of their back and radicular leg pain to a specific traumatic incident or lifting event. However, meticulous clinical history-taking frequently reveals a prodromal phase consisting of intermittent, fleeting episodes of axial back pain spanning months or years prior to the acute radicular crisis. This prodromal pain is typically mechanical in nature—exacerbated by heavy exertion, repetitive bending, twisting, or heavy lifting, and reliably relieved by rest.
The pain classically originates in the lower lumbar spine, radiating to the sacroiliac region and buttocks before extending down the posterior thigh. It is critical to differentiate axial referred pain from true radicular pain. Axial and posterior thigh pain can emanate from multiple spinal generators, including the facet joints, longitudinal ligaments, and vertebral periosteum. In contrast, true radicular pain typically extends distal to the knee, strictly following the dermatomal distribution of the compressed nerve root.

Clinical Evaluation and Provocative Testing
The hallmark history of a symptomatic lumbar disc herniation involves repetitive lower back and buttock pain that is suddenly exacerbated—often by a flexion-rotation maneuver—coinciding with the explosive onset of leg pain. In a classic herniated nucleus pulposus (HNP) with nerve root compression, the severity of the radicular leg pain equals or exceeds the axial back pain.
Clinical Pearl: Whenever leg pain is minimal and back pain is the predominant complaint, the surgeon must exercise extreme caution before diagnosing a symptomatic herniated intervertebral disc requiring surgical decompression. Bizarre pain patterns or pain of uniform, unyielding intensity should raise clinical skepticism regarding a simple discogenic etiology.
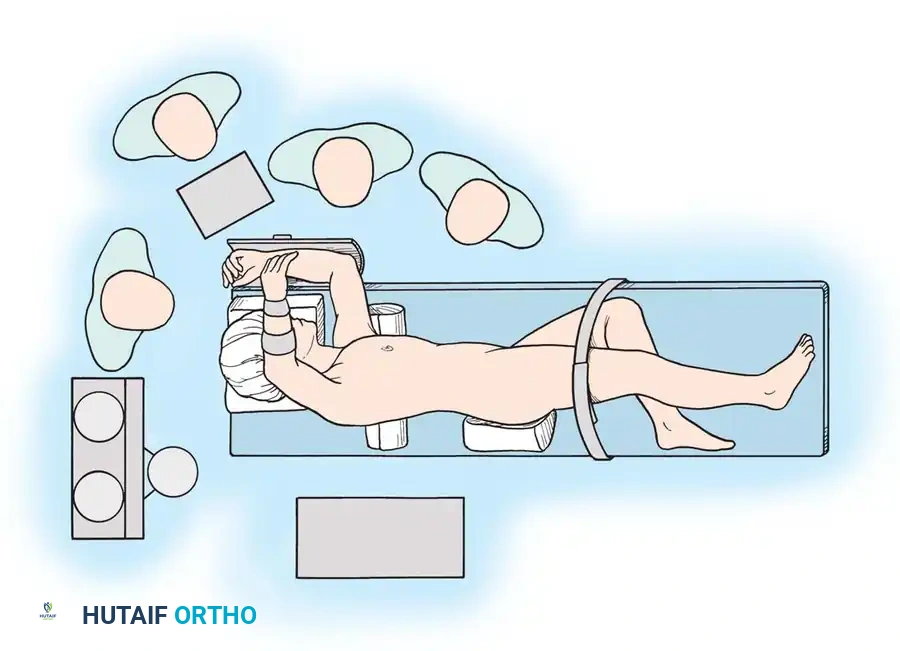
Pain from a herniated disc is highly dynamic. It typically increases with activities that elevate intradiscal pressure, such as sitting, straining, sneezing, or coughing (Valsalva maneuvers). Conversely, it is often alleviated by rest, particularly in the semi-Fowler position (supine with hips and knees flexed), which relaxes the sciatic nerve and decreases intradiscal pressure.
Physical examination findings vary depending on the acuity of the herniation. During an acute episode, patients frequently exhibit marked paraspinal muscle spasm, a loss of normal lumbar lordosis, and a compensatory sciatic list or scoliosis. Point tenderness may be elicited over the involved spinous process, with pain radiating laterally.
Provocative nerve root tension signs are paramount:
* Lasègue Sign (Straight Leg Raise - SLR): Elevation of the symptomatic leg reproduces buttock and leg pain distal to the knee. The absence of a positive SLR should prompt a re-evaluation of the diagnosis, though it may be falsely negative in older patients or upper lumbar herniations.
* Crossed Straight Leg Raise: Contralateral leg pain produced by elevating the asymptomatic leg is highly specific and should be regarded as pathognomonic for a herniated intervertebral disc (usually an axillary herniation).
* Flip Sign: If radicular pain is severe, the patient will lean back and support themselves with their hands (tripod position) when the examiner attempts to extend the knee while the patient is seated.
* Femoral Stretch Test: Highly sensitive for upper lumbar disc herniations (L2-L4). With the patient prone, the knee is acutely flexed while the examiner lifts the thigh, placing traction on the femoral nerve.
Neurological Localization and Root Compression Syndromes
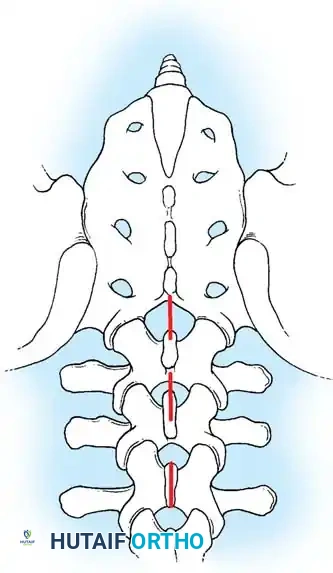
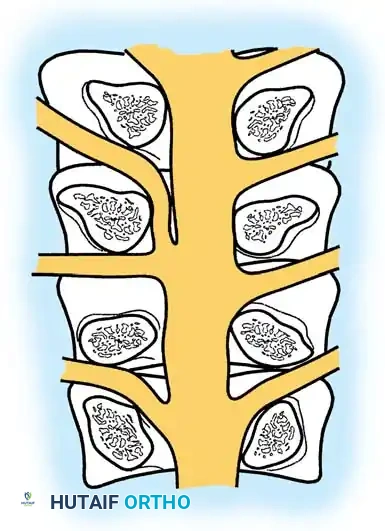
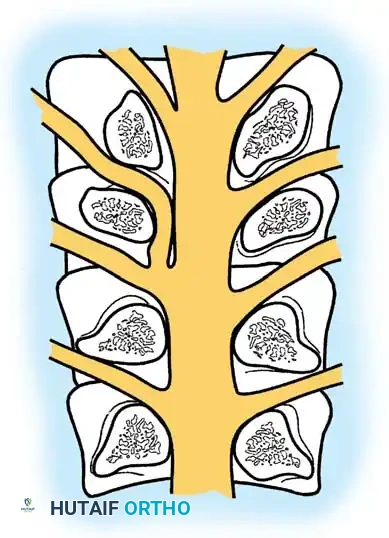
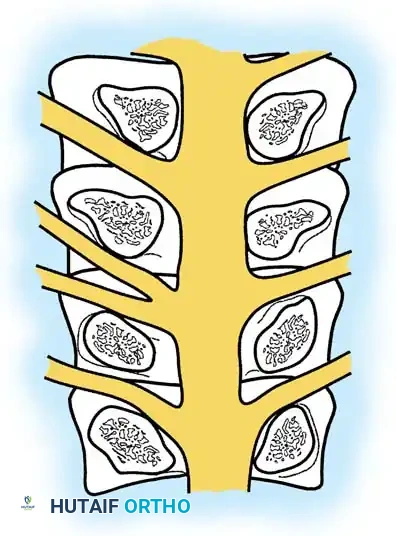
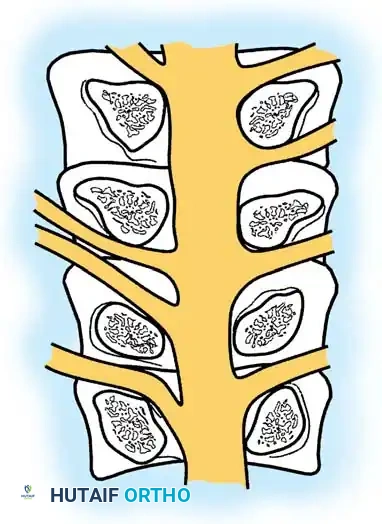
More than 95% of lumbar intervertebral disc ruptures occur at the L4-L5 or L5-S1 levels. Neurological deficits—including weakness, paresthesias, and reflex changes—must strictly map to the involved dermatome and myotome. Generalized or non-anatomical complaints suggest a nonorganic etiology or a more complex pathology (e.g., diabetic amyotrophy, peripheral neuropathy).
Biomechanical studies by Smith et al. demonstrated that spinal roots undergo 0.5 to 5 mm of linear excursion and 2% to 4% strain during motion. With increased strain, the roots migrate lateral to the pedicle, making them highly susceptible to compression from paracentral disc extrusions.

L4 Root Compression (L3-L4 Disc Herniation)
A unilateral disc herniation between L3 and L4 typically compresses the traversing L4 nerve root.
* Sensory Deficit: Pain and numbness over the posterolateral thigh, anterior knee, and anteromedial leg. The autonomous sensory zone is at the level of the medial malleolus.
* Motor Weakness: Weakness in the anterior tibial muscle (inability to heel walk). The quadriceps and hip adductors (innervated by L2, L3, L4) may also exhibit variable weakness and atrophy in chronic cases.
* Reflex Changes: Diminished or absent patellar tendon reflex. The anterior tibial tendon reflex may also be variably affected.
L5 Root Compression (L4-L5 Disc Herniation)
A unilateral herniation at L4-L5 compresses the traversing L5 root.
* Sensory Deficit: Numbness along the anterolateral leg and the dorsum of the foot, extending to the great toe. The autonomous zone is the dorsal first web space and the dorsum of the third toe.
* Motor Weakness: Weakness of the extensor hallucis longus (EHL), extensor digitorum longus and brevis, and gluteus medius.
* Reflex Changes: Typically, no primary reflex is lost, though a diminished posterior tibial reflex may occasionally be elicited.
S1 Root Compression (L5-S1 Disc Herniation)
A unilateral rupture at L5-S1 compresses the traversing S1 root.
* Sensory Deficit: Numbness over the lateral malleolus, lateral aspect of the foot, heel, and the lateral three toes. The autonomous zone is the dorsum of the fifth toe.
* Motor Weakness: Weakness in the peroneus longus and brevis, gastrocnemius-soleus complex (inability to toe walk), and gluteus maximus. Mild weakness may only manifest as asymmetrical fatigue during repetitive single-leg calf raises.
* Reflex Changes: Diminished or absent Achilles tendon reflex.
Surgical Warning: Cauda Equina Syndrome
A massive midline disc extrusion can compress the entire cauda equina, presenting as a surgical emergency. Tay and Chacha (1979) established that the triad of saddle anesthesia, bilateral ankle areflexia, and bladder dysfunction (urinary retention or overflow incontinence) constitutes the most consistent presentation. Immediate aggressive surgical decompression is mandated to prevent permanent sphincter paralysis and paraparesis.
Diagnostic Imaging
Advanced neuroimaging is critical for preoperative planning. Magnetic Resonance Imaging (MRI) remains the gold standard, providing unparalleled visualization of neural elements, disc hydration, and the exact morphology of the herniation.
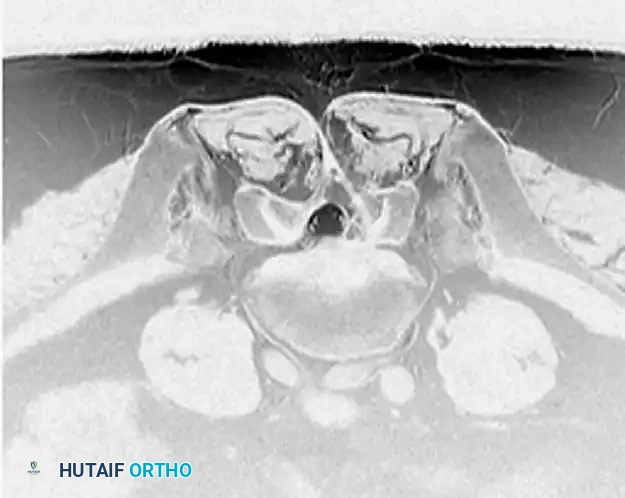
Axial T2-weighted MRI sequences allow the surgeon to differentiate between central, paracentral, foraminal, and extraforaminal (far-lateral) herniations, which directly dictates the surgical approach.

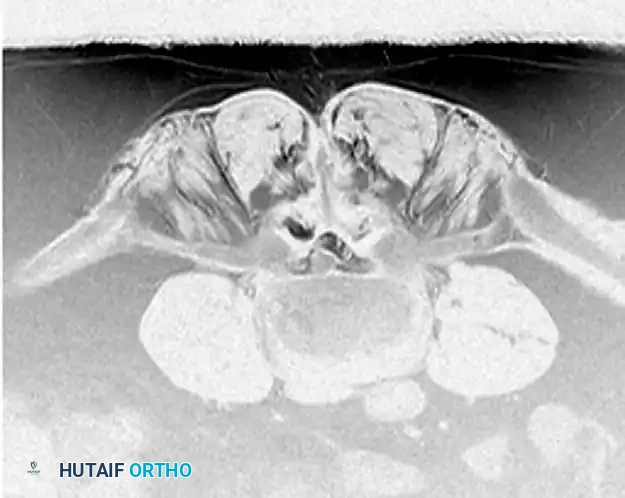
Sagittal sequences are essential for evaluating the craniocaudal extent of extruded disc fragments, assessing Modic changes in the endplates, and ruling out tandem lesions or conus medullaris pathology.
Surgical Management: Thoracic Disc Herniations
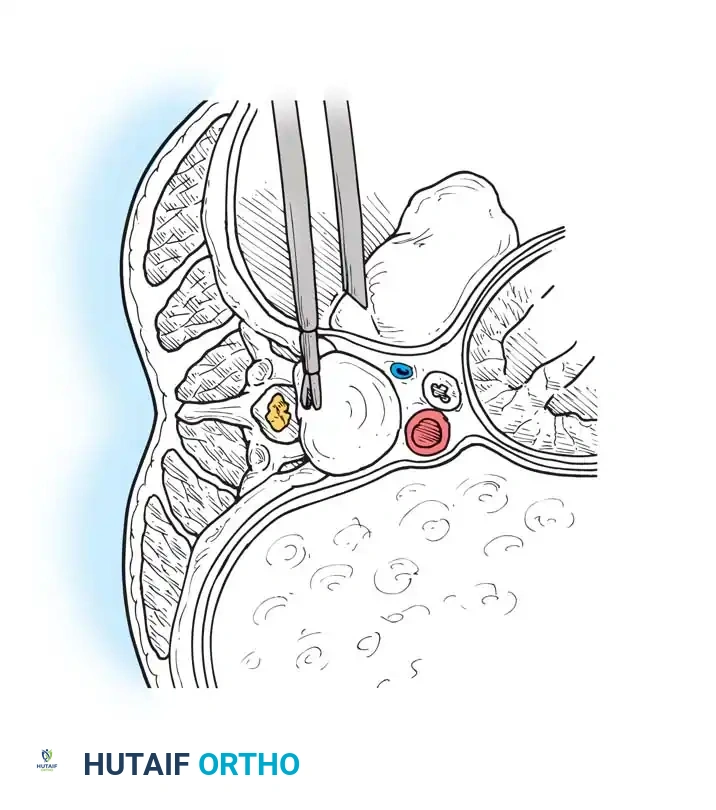
While lumbar disc herniations are frequently managed with posterior microdiscectomy, thoracic disc herniations present a unique surgical challenge. The thoracic spinal canal is narrow, and the spinal cord has tenuous vascularity. Posterior approaches (laminectomy) for central or calcified thoracic discs carry an unacceptably high risk of iatrogenic spinal cord injury and paraplegia. Therefore, anterior or anterolateral approaches are required.
Open Transthoracic Approach (Technique 39-18)
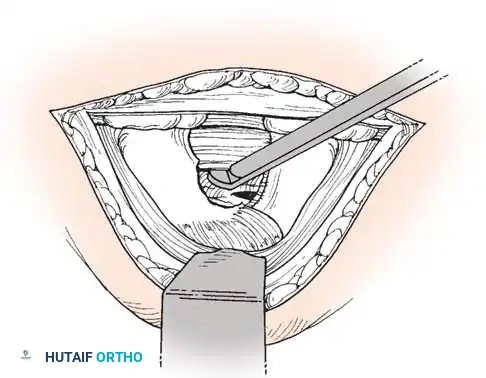
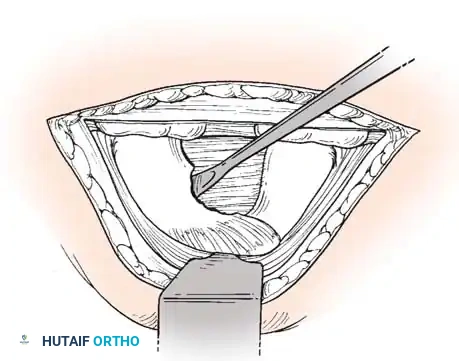
The open transthoracic approach provides direct, orthogonal visualization of the anterior dural sac, allowing for safe removal of central and calcified thoracic disc herniations.
Approach and Exposure:
* For lesions up to T5, a transthoracic approach is utilized by removing the rib two levels above the pathological disc.
* For lesions between T2 and T5, the approach requires excision of the third or fourth rib, combined with elevation of the scapula by sectioning the attachments of the serratus anterior and trapezius.
* Lesions at T1-T2 are best accessed via a low cervical approach with a sternal splitting incision.
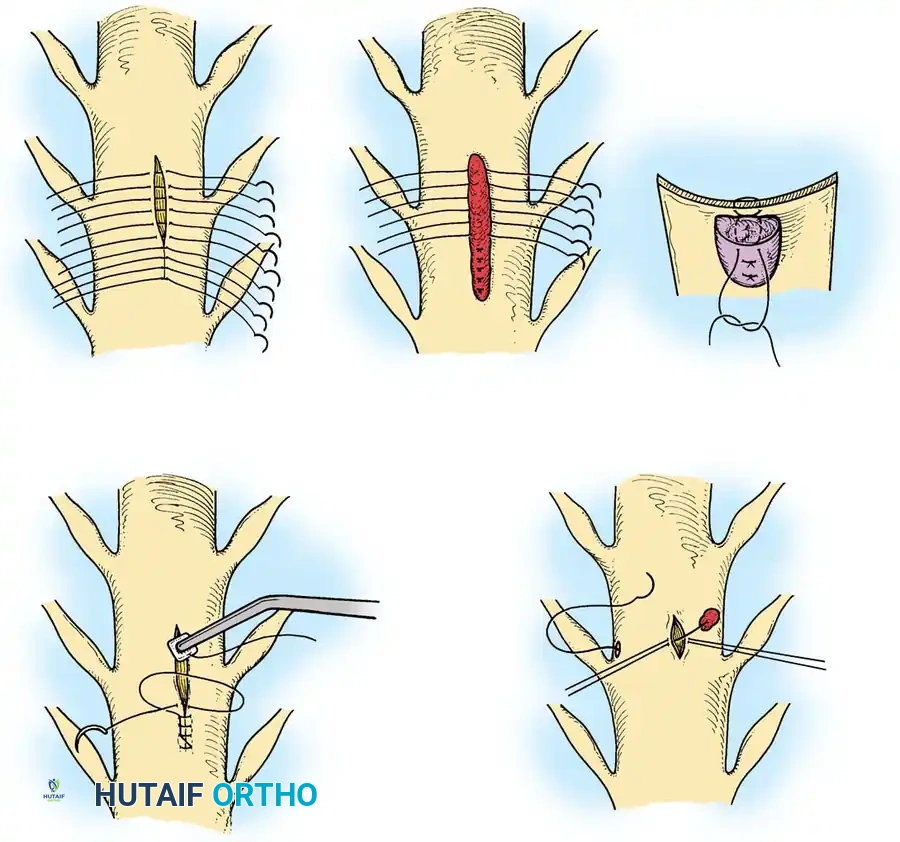
Surgical Steps:
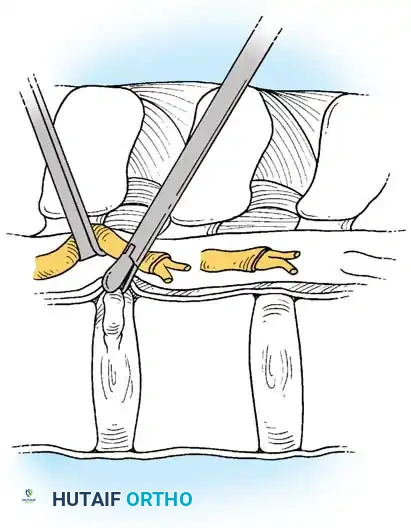
1. Vascular Mobilization: The segmental vessels overlying the target vertebral bodies are carefully ligated and divided to allow mobilization of the great vessels.
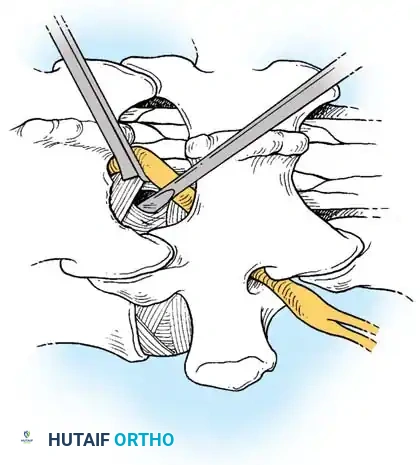
2. Rib Head Resection: The rib head articulating with the target disc space is resected. This is a critical step to allow direct observation of the pedicle and the neural foramen caudal to the disc space.
- Pedicle Removal: The cephalad portion of the pedicle is removed using a high-speed burr and Kerrison rongeurs. This exposes the poster
Associated Surgical & Radiographic Imaging
📚 Medical References
- lumbar disc disease: decompression with stability, Spine 8:86, 1983.
- Herztog RJ: Radiologic imaging in spinal stenosis, Instr Course Lect 50:137, 2001.
- Hiraizumi Y, Transfeldt EE, Fujimaki E, et al: Electrophysiologic evaluation of intermittent sacral nerve dysfunction in lumbar spinal canal stenosis, Spine 18:1355, 1993.
- Hirsh LF, Finneson BE: Intradural sacral nerve root metastasis mimicking herniated disc: case report, J Neurosurg 49:764, 1978.
- Hitselberger WE, Witten RM: Abnormal myelograms in asymptomatic patients, J Neurosurg 28:204, 1968.
- Hurri H, Slatis P, Soini J, et al: Lumbar spinal stenosis: assessment of long-term outcome 12 years after operative and conservative treatment, J Spinal Disord 11:110, 1998.
- Iguchi T, Kurihara A, Nakayama J, et al: Minimum 10-year outcome of decompressive laminectomy for degenerative lumbar spinal stenosis, Spine 25:1754, 2000.
- Inufusa A, An H, Lim T, et al: Anatomic changes of the spinal canal and intervertebral foramen associated with fl exionextension movement, Spine 21:2412, 1996.
- Jackson RP, Cain JE, Jacobs RR, et al: The neuroradiographic diagnosis of lumbar herniated nucleus pulposus (parts I and II), Spine 13:1352.
- Jiang GX, Xu WD, Wang AH: Spinal stenosis with meralgia paraesthetica, J Bone Joint Surg 70B:272, 1988.
- Johansson JE, Barington TW, Amelie M: Combined vascular and neurogenic claudication, Spine 7:150, 1992.
- Johnsson K, Rosén I, Udén A: The natural course of lumbar spinal stenosis, Clin Orthop Relat Res 279:82, 1992.
- Johnsson K, Udén A, Rosén I: The effect of decompression on the natural course of spinal stenosis: a comparison of surgically treated and untreated patients, Spine 16:615, 1991.
- Johnsson K, Willner S, Pettersson H: Analysis of operated cases with lumbar spinal stenosis, Acta Orthop Scand 52:427, 1981.
- Jönsson B, Annertz M, Sjoberg C, et al: A prospective and consecutive study of surgically treated lumbar spinal stenosis, I: clinical features related to radiographic fi ndings, Spine 22:2932, 1997.
- Jönsson B, Annertz M, Sjoberg C, et al: A prospective and consecutive study of surgically treated lumbar spinal stenosis, II: fi ve-year follow-up by an independent observer, Spine 22:2938, 1997.
- Jönsson B, Strömqvist B: Symptoms and signs in degeneration of the lumbar spine: a prospective consecutive study of 300 operated patients, J Bone Joint Surg 75B:381, 1993.
- Jönsson B, Strömqvist B: Decompression for lateral lumbar spinal stenosis: results and impact on sick leave and working conditions, Spine 19:2381, 1994.
- Kanamori M, Matsue H, Hirano N, et al: Trumpet laminectomy for lumbar degenerative spinal stenosis, J Spinal Disord 6:232, 1993.
- Karayannacos PE, Yashon D, Vasko JS: Narrow lumbar spinal canal with “vascular” syndromes, Arch Surg 111:803, 1976.
- Katz JN, Lipson SJ, Change LC, et al: Sevento 10-year outcome of decompressive surgery for degenerative lumbar spinal stenosis, Spine 21:92, 1996.
- Katz JN, Lipson SJ, Lew RA, et al: Lumbar laminectomy alone or with instrumented or noninstrumented arthrodesis in degenerative lumbar spinal stenosis: patient selection, costs, and surgical outcomes, Spine 22:1123, 1997.
- Katz JN, Stucki G, Lipson SJ, et al: Predictors of surgical outcome in degenerative lumbar spinal stenosis, Spine 24:2229, 1999.
- Kauffman C, Garfi n SR: Spinal stenosis: pathophysiology and symptom complex update 1999, Semin Spine Surg 11:209, 1999.
- Kawaguchi Y, Kanamori M, Ishihara, et al: Clinical and radiographic results of expansive lumbar laminoplasty in patients with spinal stenosis, J Bone Joint Surg 86A:1698, 2004.
- Keller RB, Atlas SJ, Soule DN, et al: Relationship between rates and outcomes of operative treatment for lumbar disc herniation and spinal stenosis, J Bone Joint Surg 81A:752, 1999.
- Kimura I, Oh-Hama M, Shingu H: Cervical myelopathy treated by canal-expansive laminaplasty: computed tomographic and myelographic fi ndings, J Bone Joint Surg 66A:914, 1984.
- Kirkaldy-Willis WH: The relationship of structural pathology to the nerve root, Spine 9:49, 1984.
- Kirkaldy-Willis WH, Wedge JH, Yong-Hing K, et al: Pathology and pathogenesis of lumbar spondylosis and stenosis, Spine 4:319, 1978.
- Kirkaldy-Willis WH, Wedge JH, Yong-Hing K, et al: Lumbar spinal nerve lateral entrapment, Clin Orthop Relat Res 169:171, 1982.
- Knaub MA, Won DS, McGuire R, et al: Lumbar spinal stenosis: indications for arthrodesis and spinal instrumentation, Instr Course Lect 54:313, 2005.
- Kornblum MB, Fischgrund JS, Herkowitz HN, et al: Degenerative lumbar spondylolisthesis with spinal stenosis: a prospective long-term study comparing fusion and pseudarthrosis, Spine 29:726, 2004.
- Korovessis P, Papazisis Z, Koureas G, et al: Rigid, semirigid versus dynamic instrumentation for degenerative lumbar spinal stenosis: a correlative radiological and clinical analysis of shortterm results, Spine 29:735, 2004.
- Kostuik JP, Musha Y: Extension to the sacrum of previous adolescent scoliosis fusions in adult life, Clin Orthop Relat Res 364:53, 1999.
- Kuntz KM, Snider RK, Weinstein JN, et al: Cost-effectiveness of fusion with and without instrumentation of patients with degenerative spondylolisthesis and spinal stenosis, Spine 25:1132, 2000.
- Lanes TC, Gauron EF, Spratt KF, et al: Long-term follow-up of patients with chronic back pain treated in a multidisciplinary rehabilitation program, Spine 20:801, 1995.
- Larequi-Lauber T, Vader JP, Burnand B, et al: Appropriateness of indications for surgery of lumbar disc hernia and spinal stenosis, Spine 22:203, 1997.
- Lee BCP, Kazam E, Newman AD: Computed tomography of the spine and spinal cord, Radiology 128:95, 1978.
- Lee J, Hida K, Seki T, et al: An interspinous process distractor (X STOP) for lumbar spinal stenosis in elderly patients: preliminary experiences in 10 consecutive cases, J Spinal Disord Tech 17:72, 2004.
- Lehmann TR, Spratt KF, Tozzi JE, et al: Long-term follow-up of lower lumbar fusion patients, Spine 12:97, 1987.
- Leroux JL, Legeron P, Moulinier L, et al: Stenosis of the lumbar spinal canal in vertebral ankylosing hyperostosis, Spine 17:1213, 1992.
- Liew SM, Simmons ED Jr: Cervical deformity: rationale for selecting the appropriate fusion technique (anterior, posterior, and 360 degree), Orthop Clin North Am 29:779, 1998.
- Lipson SJ: Spinal stenosis defi nitions, Semin Spine Surg 1:135, 1989.
- Liyang D, Yinkan X, Wenming Z, et al: The effect of fl exionextension motion of the lumbar spine on the capacity of the spinal canal: an experimental study, Spine 14:523, 1989.
- Macnab I: Cervical spondylosis, Clin Orthop Relat Res 109:69, 1975.
- Mariconda M, Fava R, Gatto A, et al: Unilateral laminectomy for bilateral decompression of lumbar spinal stenosis: a prospective comparative study with conservatively treated patients, J Spinal Disord Tech 15:39, 2002.
- Mariconda M, Zanforlino G, Celestino GA, et al: Factors infl uencing the outcome of degenerative lumbar spinal stenosis, J Spinal Disord 13:131, 2000.
- Matsui H, Kanamori M, Ishihara H, et al: Expansive lumbar laminoplasty for degenerative spinal stenosis in patients below 70 years of age, Eur Spine J 6:191, 1997.
- Matsui H, Tsuji H, Sekido H et al: Results of expansive laminoplasty for lumbar spinal stenosis in active manual workers, Spine 17:S37, 1992.
- McCullen GM, Bernini PM, Bernstein SH, et al: Clinical and radiographic results of decompression for lumbar spinal stenosis, J Spinal Disord 7:380, 1994.
- McGuire RA: Instrumentation of the stenotic spine with and without deformity, Semin Spine Surg 11:277, 1999.
- McPhee IB, Swanson CE: The surgical management of degenerative lumbar scoliosis: posterior instrumentation alone versus two-stage surgery, Bull Hosp Jt Dis 57:16, 1998.
- Messersmith RN, Cronan J, Esparza AR: Computed tomography-guided percutaneous biopsy: combined approach to the retroperitoneum, Neurosurgery 14:218, 1984.
- Middlebrooks ES, Balderston RA: Decision making and operative treatment: decompression versus decompression and arthrodesis, Semin Spine Surg 11:234, 1999.
- Miyakoshi N, Abe E, Shimada Y, et al: Outcome of one-level posterior lumbar interbody fusion for spondylolisthesis and postoperative intervertebral disc degeneration adjacent to the fusion, Spine 25:1837, 2000.
- Mofi di A, O’Connor D, El-Abed K, et al: Functional outcome study of patients after surgical decompression for lumbar spinal stenosis: effects of concomitant pathology, J Spinal Disord Tech 15:377, 2002.
- Mullin BB, Rea GL, Irsik R, et al: The effect of postlaminectomy spinal instability on the outcome of lumbar spinal stenosis patients, J Spinal Disord 9:107, 1996.
- Nelson MA: Lumbar spinal stenosis, J Bone Joint Surg 55B:506, 1973.
- O’Leary PF, McCance SE: Distraction laminoplasty for decompression of lumbar spinal stenosis, Clin Orthop Relat Res 384:26, 2001.
- Paine KWE: Clinical features of lumbar spinal stenosis, Clin Orthop Relat Res 115:77, 1976.
- Paine KWE: Results of decompression for lumbar spinal stenosis, Clin Orthop Relat Res 115:96, 1976.
- Palumbo MA, Hilibrand AS, Hart RA, et al: Surgical treatment of thoracic spinal stenosis: a 2to 9-year follow-up, Spine 26:558, 2001.
- Phillips FM: The argument for noninstrumented posterolateral fusion for patients with spinal stenosis and degenerative spondylolisthesis, Spine 29:170, 2004.
- Phillips FM, Carlson GD, Bohlman HH, et al: Results of surgery for spinal stenosis adjacent to previous lumbar fusion, J Spinal Disord 13:432, 2000.
- Porter RW, Hibbert C: Calcitonin treatment for neurogenic claudication, Spine 8:585, 1983.
- Porter RW, Hibbert C, Evans C: The natural history of root entrapment syndrome, Spine 9:418, 1984.
- Porter RW, Hibbert C, Wellman P: Backache and the lumbar spinal canal, Spine 5:99, 1980.
- Porter RW, Miller CG: Neurogenic claudication and root claudication treated with calcitonin: a double-blind trial, Spine 13:1061, 1988.
- Posner I, White AA III, Edwards WT, et al: A biomechanical analysis of the clinical stability of the lumbar and lumbosacral spine, Spine 7:374, 1982.
- Postacchini F: Surgical management of lumbar spinal stenosis, Spine 24:1043, 1999.
- Postacchini F, Cinotti G: Bone regrowth after surgical decompression for lumbar spinal stenosis, J Bone Joint Surg 74B:862, 1992.
- Postacchini F, Pezzeri G, Montanaro A, et al: Computerized tomography in lumbar stenosis: a preliminary report, J Bone Joint Surg 62B:78, 1980.
- Ragab AA, Fye MA, Bohlman HH: Surgery of the lumbar spine for spinal stenosis in 118 patients 70 years of age or older, Spine 28:348, 2003.
- Raskin SP: Degenerative changes of the lumbar spine: assessment by computed tomography, Orthopedics 4:186, 1981.
- Resnick DK, Choudhri TF, Dailey AT, et al: Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine, part 9: fusion in patients with stenosis and spondylolisthesis, J Neurosurg Spine 2:679, 2005.
- Resnick DK, Choudhri TF, Dailey AT, et al: Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine, part 10: fusion following decompression in patients with stenosis without spondylolisthesis, J Neurosurg Spine 2:686, 2005.
- Riew KD, Rhee J: Microsurgical techniques in lumbar spinal stenosis, Instr Course Lect 51:247, 2002.
- Rinaldi I, Mullins WJ, Delandy WF, et al: Computerized tomographic demonstration of rotational atlanto-axial fi xation: case report, J Neurosurg 50:115, 1979.
- Rivest C, Katz JN, Ferrante FM, et al: Effects of epidural steroid injection on pain due to lumbar spinal stenosis or herniated disks: a prospective study, Arthritis Care Res 11:291, 1998.
- Rydevik B, Brown MD, Lundborg G: Pathoanatomy and pathophysiology of nerve root compression, Spine 9:7, 1984.
- Saifuddin A: The imaging of lumbar spinal stenosis, Clin Radiol 55:581, 2000.
- Saint-Louis LA: Lumbar spinal stenosis assessment with computed tomography, magnetic resonance imaging, and myelography, Clin Orthop Relat Res 384:122, 2001.
- San Martino A, D’Andria FM, San Martino C: The surgical treatment of nerve root compression caused by scoliosis of the lumbar spine, Spine 8:261, 1983.
- Schillberg B, Nystrom B: Quality of life before and after microsurgical decompression in lumbar spinal stenosis, J Spinal Disord 13:237, 2000.
- Schmid G, Better S, Gottmann D, et al: CT-guided epidural/ perineural injections in painful disorders of the lumbar spine: shortand extended-term results, Cardiovasc Interv Radiol 22:493, 1999.
- Schnebel B, Kingston S, Watkins R, et al: Comparison of MRI to contrast CT in the diagnosis of spinal stenosis, Spine 14:332, 1989.
- Schönström NSR, Bolender N, Spengler DM: The pathomorphology of spinal stenosis as seen on CT scans of the lumbar spine, Spine 10:806, 1985.
- Sengupta DK, Herkowitz HN: Lumbar spinal stenosis: treatment strategies and indications for surgery, Orthop Clin North Am 34:281, 2003.
- Shakil MS, Vaccaro AR, Albert TJ, et al: Effi cacy of conservative treatment of lumbar spinal stenosis, Semin Spine Surg 11:229, 1999.
- Sheehan JM, Helm GA, Kallmes DFR, et al: Partial pediculectomy in the treatment of lumbar spinal stenosis: technical note, Neurosurgery 41:308, 1997.
- Shenkin HA, Hash CJ: Spondylolisthesis after multiple bilateral laminectomies and facetectomies for lumbar spondylosis, J Neurosurg 50:45, 1979.
- Simmons ED: Surgical treatment of patients with lumbar spinal stenosis with associated scoliosis, Clin Orthop Relat Res 384:45, 2001.
- Simmons ED Jr, Simmons EH: Spinal stenosis with scoliosis, Spine 17(suppl):117, 1992.
- Simotas AC: Nonoperative treatment for lumbar spinal stenosis, Clin Orthop Relat Res 384:153, 2001.
- Simotas AC, Dorey FJ, Hansraj KK, et al: Nonoperative treatment for lumbar spinal stenosis: clinical and outcome results and a 3-year survivorship analysis, Spine 15:197, 2000.
- Speciale AC, Pietrobon R, Urban CW, et al: Observer variability in assessing lumbar spinal stenosis severity on magnetic resonance imaging and its relation to cross-sectional spinal canal area, Spine 27:1082, 2002.
- Spengler DM: Current concepts review: degenerative stenosis of the lumbar spine, J Bone Joint Surg 69A:305, 1987.
- Spivak JM: Degenerative lumbar spinal stenosis, J Bone Joint Surg 80A:1053, 1998.
- Stambough JL: Principles of decompression for lumbar spinal stenosis, Semin Spine Surg 11:244, 1999.
- Stambough JL, Templin CR: Indirect decompression and reduction in the stenotic spine: is there a role for fusion? Semin Spine Surg 11:262, 1999.
- Stitz MY, Sommer HM: Accuracy of blind versus fl uoroscopically guided caudal epidural injection, Spine 24:1371, 1999.
- Styblo K, Bossers GT, Slot GH: Osteotomy for kyphosis in
You Might Also Like

