Valgus Osteotomy for Developmental Coxa Vara: An Intraoperative Masterclass
Key Takeaway
This masterclass details valgus osteotomy for developmental coxa vara, a proximal femoral deformity. We cover critical preoperative planning, precise patient positioning, and a step-by-step intraoperative guide for K-wire, Wagner, and blade plate fixation techniques. Comprehensive surgical anatomy, neurovascular considerations, and extensive pearls and pitfalls are discussed to ensure optimal outcomes and manage potential complications effectively.
Introduction and Epidemiology
Developmental coxa vara, historically referred to as cervical or infantile coxa vara, represents a rare but clinically significant deformity of the proximal femur. It is fundamentally characterized by a progressive decrease in the neck-shaft angle (NSA) to less than 110 degrees. Unlike the congenital form of coxa vara, which is present at birth and frequently associated with significant limb-length discrepancy (LLD) and other embryonic limb bud abnormalities (such as proximal focal femoral deficiency), developmental coxa vara manifests in early childhood, typically becoming clinically apparent after the onset of ambulation.
Epidemiologically, developmental coxa vara is an exceedingly rare musculoskeletal entity, with an estimated worldwide incidence of 1 in 25,000 live births. It occurs with equal frequency in males and females, and bilateral involvement is observed in approximately one-third to one-half of documented cases. Crucially, this specific form of coxa vara is isolated; it is not systematically connected to an increased association with other musculoskeletal abnormalities or systemic syndromic conditions, differentiating it from acquired forms secondary to metabolic bone diseases (e.g., rickets), fibrous dysplasia, trauma, or neoplastic processes.

The exact etiology of developmental coxa vara remains elusive, though the prevailing pathophysiological model was proposed by Pylkkanen. This theory postulates that the varus deformity originates from a primary ossification defect localized to the medial aspect of the femoral neck. This localized defect results in a more vertical orientation of the proximal femoral physis. Consequently, dystrophic bone forms along the medial femoral neck. During normal weight-bearing, physiologic shearing stresses fatigue this dystrophic bone, creating a vicious cycle of microfracture, altered growth, and progressive varus deformity. Histological analyses of biopsies taken from the proximal femoral physis in these patients reveal an enlarged growth plate containing disorganized islands of cartilage with relatively reduced cellular numbers. These histopathologic findings bear a striking resemblance to those observed in the proximal tibia of patients with infantile Blount’s disease, as well as the proximal femoral physis in patients with metaphyseal chondrodysplasia (Schmid type). Notably, there is no histological evidence of osteonecrosis in the primary pathogenesis of developmental coxa vara.
Surgical Anatomy and Biomechanics
A profound understanding of proximal femoral growth and hip biomechanics is requisite for the surgical management of developmental coxa vara. Growth of the proximal femur is driven by three distinct but interrelated centers: the proximal femoral physeal plate, the femoral neck isthmus, and the greater trochanteric apophysis. The synchronized growth at these specific sites dictates the ultimate size, shape, and spatial orientation of the proximal femur, explicitly determining the femoral neck length and the NSA.

In normal skeletal development, the capital femoral epiphyseal ossification center becomes radiographically visible between 3 and 6 months of age, followed by the trochanteric secondary center of ossification at approximately 4 years of age. The NSA undergoes a predictable physiologic progression, starting at approximately 150 degrees in the neonate and gradually remodeling to a more varus position, stabilizing near 120 to 130 degrees at skeletal maturity.
In developmental coxa vara, the primary ossification defect alters this trajectory. Any disruption to the proximal physis, combined with the continued uninhibited growth of the greater trochanteric apophysis, exacerbates the varus deformity.

Biomechanically, the hip joint operates as a first-class lever. The vertical orientation of the physis in developmental coxa vara fundamentally alters the force vectors across the hip joint. Normal compressive forces are pathologically converted into high-magnitude shear forces across the physis and the medial femoral neck. This shear stress not only inhibits normal endochondral ossification but also places the femoral neck at significant risk for stress fracture and subsequent nonunion.
Furthermore, as the NSA decreases, the greater trochanter relatively overgrows and migrates proximally. This decreases the articulotrochanteric distance (ATD)—the vertical distance between the tip of the greater trochanter and the superior articular surface of the femoral head. A shortened or negative ATD critically reduces the resting length and mechanical advantage of the hip abductor musculature (gluteus medius and minimus), manifesting clinically as a profound Trendelenburg gait and early abductor fatigue.

Indications and Contraindications
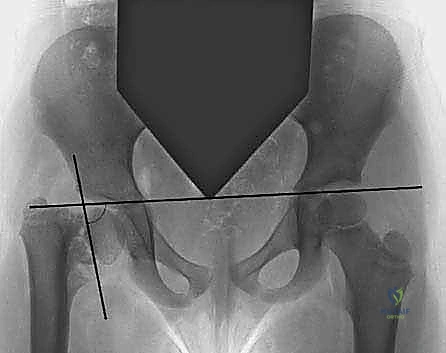
The natural history of developmental coxa vara dictates the indications for surgical intervention. The most critical prognostic indicator is the Hilgenreiner-epiphyseal angle (HEA), as extensively described by Weinstein et al. The HEA is measured on an anteroposterior (AP) radiograph of the pelvis as the angle subtended by Hilgenreiner’s line (a horizontal line connecting the bilateral triradiate cartilages) and a line drawn parallel to the proximal femoral physis.
Patients presenting with an HEA greater than 60 degrees demonstrate invariable progression of the varus deformity. Without surgical correction, the progressive varus and associated femoral retroversion lead to severe cam-type femoroacetabular impingement, premature degenerative osteoarthritis, and debilitating pain. Furthermore, the extreme mechanical strain can culminate in a femoral neck stress fracture. Therefore, an HEA > 60 degrees is an absolute indication for surgical intervention, typically via a proximal femoral valgus osteotomy.
Conversely, patients with an HEA between 45 and 60 degrees occupy a prognostic "gray zone." These patients require rigorous serial radiographic monitoring, as their deformity may either progress, stabilize, or occasionally improve. Surgery is indicated in this cohort only if documented progression of the varus deformity or worsening clinical symptoms (e.g., progressive Trendelenburg gait) occur. An HEA of less than 45 degrees typically resolves spontaneously with growth and is managed non-operatively.

| Clinical Scenario | Hilgenreiner-Epiphyseal Angle | Management Strategy | Rationale |
|---|---|---|---|
| Severe / Progressive | > 60 degrees | Operative: Valgus Osteotomy | Invariable progression; high risk of stress fracture, impingement, and early osteoarthritis. |
| Indeterminate | 45 to 60 degrees | Observation: Serial Radiographs | Unpredictable natural history. Intervene only if documented progression or worsening gait mechanics. |
| Mild / Resolving | < 45 degrees | Non-Operative: Observation | High likelihood of spontaneous resolution with continued skeletal growth. |
| Symptomatic Impingement | Any HEA with severe retroversion | Operative: Valgus-Derotation Osteotomy | Address cam-impingement and restore abductor mechanics to prevent joint degeneration. |
Contraindications to surgical intervention include active local or systemic infection, severe medical comorbidities precluding safe anesthesia, and an HEA < 45 degrees without evidence of progression.
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is the cornerstone of a successful proximal femoral valgus osteotomy. The primary biomechanical objective of the procedure is to horizontalize the proximal femoral physis, thereby converting pathologic shear forces back into physiologic compressive forces, which stimulates normal ossification and healing of the medial neck defect.
Standard radiographic evaluation must include a standing AP pelvis and a frog-leg lateral view of the affected hip. The surgeon must meticulously calculate the preoperative HEA, the NSA, the ATD, and the degree of femoral retroversion.

The target postoperative HEA should be less than 38 degrees, with many authors advocating for a goal of 30 to 35 degrees to ensure a robust mechanical environment that prevents recurrence. The required angle of correction (the wedge to be resected or the angle of the opening wedge) is calculated by subtracting the desired postoperative HEA from the preoperative HEA. Concurrently, the NSA should be restored to at least 130 degrees.
Templating is performed using digital software or traditional acetate overlays. The surgeon must select the appropriate fixation construct based on the child's age, size, and bone quality. Common options include pediatric fixed-angle blade plates (e.g., 100-degree, 110-degree, or 130-degree plates), locking proximal femoral osteotomy plates, or, in older children, a dynamic hip screw (DHS) system.

If the ATD is severely negative, the preoperative plan must also include a strategy for the greater trochanter. In younger children (typically under 8 years of age), a prophylactic greater trochanteric epiphysiodesis may be sufficient to arrest trochanteric overgrowth while the femoral neck continues to grow. In older children with a fixed, severely negative ATD, a formal distal and lateral advancement of the greater trochanter may be required to restore the abductor lever arm.
Patient Positioning and Operating Room Setup
The patient is placed supine on a radiolucent flat table. Some surgeons prefer a pediatric fracture table to allow for precise control of traction and rotation; however, a flat radiolucent table with a bump under the ipsilateral hemipelvis provides excellent flexibility and allows for a free drape of the operative extremity, facilitating dynamic intraoperative assessment of hip range of motion and impingement.

High-quality intraoperative fluoroscopy is mandatory. The C-arm should be positioned to easily obtain both AP and cross-table lateral views of the proximal femur and hip joint without compromising the sterile field. The entire hemipelvis and lower extremity must be prepped and draped free to allow for manipulation during the reduction and fixation phases.
Detailed Surgical Approach and Technique
The surgical approach to the proximal femur for a valgus osteotomy is typically achieved via a standard lateral or Watson-Jones approach.
Superficial and Deep Dissection
A longitudinal incision is made centered over the greater trochanter, extending distally along the lateral shaft of the femur. The fascia lata is incised in line with the skin incision. For the deep dissection, the vastus lateralis is identified. A standard subvastus or transvastus approach is utilized. The vastus lateralis is elevated off the lateral intermuscular septum and retracted anteriorly, exposing the proximal femoral shaft and the base of the greater trochanter. Perforating vessels from the profunda femoris are meticulously identified and coagulated to prevent postoperative hematoma.

Guide Wire Placement and Proximal Fixation Preparation
Once the proximal femur is exposed, a guide wire is placed into the femoral neck and head under strict fluoroscopic guidance. The starting point is typically at the lateral cortex, just distal to the greater trochanteric physis. The wire is advanced parallel to the femoral neck and perfectly centered within the femoral head on both the AP and lateral projections.
If a fixed-angle blade plate is utilized, the seating chisel is introduced over the guide wire or parallel to it, depending on the specific instrumentation system. The angle of chisel insertion relative to the femoral shaft axis must equal the desired correction angle. It is critical that the chisel or proximal locking screws do not violate the capital femoral physis to avoid premature physeal closure, unless the physis is already closing or intentionally bypassed in an older adolescent.

Osteotomy Execution
Several osteotomy techniques exist, including the Pauwels Y-shaped osteotomy, the Langenskiöld dome osteotomy, and the standard lateral closing-wedge osteotomy. The lateral closing-wedge osteotomy is the most commonly employed due to its relative simplicity and excellent bony apposition.

- Marking the Osteotomy: The predetermined wedge is marked on the lateral cortex using electrocautery or a sterile marker. The proximal cut is typically made transverse to the femoral shaft, just proximal to the lesser trochanter. The distal cut is angled to create the laterally based wedge, corresponding to the planned angle of correction.
- Performing the Cuts: Using an oscillating saw under continuous saline irrigation to prevent thermal necrosis, the proximal cut is completed. The distal cut is then performed, completing the wedge resection.
- Derotation: If femoral retroversion is present (common in developmental coxa vara), the distal fragment is internally rotated relative to the proximal fragment before final fixation to restore normal femoral anteversion.

Reduction and Final Fixation
The proximal fragment is manipulated into a valgus position, closing the lateral wedge gap. The pre-selected plate (blade plate or locking plate) is applied to the lateral cortex of the distal fragment.

Compression across the osteotomy site is achieved using an articulated tension device or dynamic compression principles through the plate holes. The distal screws are then inserted, obtaining bicortical purchase. Fluoroscopy is used to confirm the final HEA (targeting < 38 degrees), the NSA, and the hardware position.

Addressing the Greater Trochanter
Following the valgus correction, the relative position of the greater trochanter must be reassessed. If the ATD remains negative, a greater trochanteric epiphysiodesis is performed by drilling across the trochanteric physis. In severe cases, a formal osteotomy of the greater trochanter is performed, and the trochanter is advanced distally and laterally, secured with tension band wiring or heavy non-absorbable sutures, to optimize the abductor lever arm.
The wound is irrigated copiously, and the vastus lateralis fascia, fascia lata, subcutaneous tissues, and skin are closed in a layered fashion.
Complications and Management
While valgus osteotomy is highly effective in altering the natural history of developmental coxa vara, it is a technically demanding procedure associated with several potential complications. Meticulous preoperative planning and precise intraoperative execution are paramount to minimizing these risks.

| Complication | Incidence / Risk Factors | Prevention and Management Strategies |
|---|---|---|
| Recurrence of Varus | Most common complication. Risk is high if post-op HEA > 38 degrees or if fixation fails. | Prevention: Ensure absolute correction of HEA to < 38 degrees (ideally 30-35). Use rigid internal fixation. Management: Repeat valgus osteotomy once recurrence is documented and symptomatic. |
| Premature Physeal Closure | Occurs if hardware violates the capital physis or secondary to vascular insult during neck dissection. | Prevention: Precise fluoroscopic guidance. Avoid intra-articular penetration. Do not cross the physis with wires or screws unless intentionally performing epiphysiodesis. Management: Monitor for LLD. Contralateral epiphysiodesis or ipsilateral lengthening may be required near skeletal maturity. |
| Limb Length Discrepancy | Can occur due to initial deformity, overgrowth post-osteotomy, or premature physeal arrest. | Prevention: Careful monitoring of growth percentiles postoperatively. Management: Shoe lifts for minor discrepancies (< 2 cm). Surgical equalization (epiphysiodesis or lengthening) for discrepancies > 2 cm at maturity. |
| Nonunion / Delayed Union | Rare in the pediatric population due to robust osteogenic potential, but possible with inadequate fixation. | Prevention: Ensure rigid compression across the osteotomy site. Preserve soft tissue attachments. Management: Revision internal fixation with autologous bone grafting. |
| Infection | < 1-2%. Risk factors include prolonged operative time and poor soft tissue handling. | Prevention: Perioperative prophylactic antibiotics, meticulous hemostasis, and sterile technique. Management: Aggressive surgical debridement, implant retention if stable, and culture-directed intravenous antibiotics. |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is heavily dependent on the rigidity of the internal fixation achieved and the age of the patient.
Historically, patients were routinely placed in a 1.5 hip spica cast for 6 to 8 weeks to protect the osteotomy. However, with the advent of modern rigid pediatric locking plates and fixed-angle blade plates, routine spica casting is largely obsolete, provided secure fixation is confirmed intraoperatively.
Phase I: Immediate Postoperative (Weeks 0-6)
* Weight Bearing: The patient is typically restricted to toe-touch weight bearing (TTWB) or non-weight bearing (NWB) on the operative extremity using crutches or a walker.
* Motion: Early active and active-assisted range of motion (ROM) of the hip, knee, and ankle is encouraged to prevent stiffness and promote cartilage nutrition.
* Monitoring: AP and lateral radiographs are obtained at 2 weeks and 6 weeks postoperatively to assess the maintenance of correction and the progression of bony union at the osteotomy site.
Phase II: Consolidation and Strengthening (Weeks 6-12)
* Weight Bearing: Once radiographic evidence of bridging callus and clinical stability are observed (typically around 6 to 8 weeks), the patient is gradually transitioned to partial weight bearing, advancing to full weight bearing as tolerated.
* Physical Therapy: A formal physical therapy program is initiated. The primary focus is on restoring the strength of the hip abductor musculature (gluteus medius and minimus) to eliminate the residual Trendelenburg gait. Aquatic therapy can be highly beneficial during this transition phase.
Phase III: Long-Term Surveillance (Months to Years)
* Follow-up: Patients must be followed longitudinally until skeletal maturity. Annual radiographs (standing AP pelvis) are required to monitor the HEA, NSA, and ATD.
* Hardware Removal: Routine hardware removal is generally not indicated unless the implant causes local soft tissue irritation, prominent bursa formation, or if it spans a growth plate that requires un-tethering. If removal is elected, it is typically performed 12 to 18 months postoperatively, after complete remodeling of the osteotomy site.
Summary of Key Literature and Guidelines
The academic foundation for the surgical management of developmental coxa vara relies heavily on a few landmark studies that have defined the biomechanics, natural history, and surgical indications.
- Weinstein et al. (Natural History and Indications): This seminal work established the Hilgenreiner-epiphyseal angle (HEA) as the paramount prognostic indicator. The guideline that an HEA > 60 degrees mandates surgery, while an HEA < 45 degrees can be observed, remains the gold standard in pediatric orthopedic decision-making.
- Pylkkanen (Pathogenesis): Pylkkanen’s extensive review provided the prevailing theory of the primary ossification defect in the medial femoral neck, explaining the conversion of compressive to shear forces and the resulting dystrophic bone fatigue.
- Desai and MacEwen (Long-Term Outcomes): Their research highlighted the critical need to overcorrect the deformity. They demonstrated that achieving a postoperative HEA of less than 38 degrees is the most significant factor in preventing the recurrence of varus deformity.
- Carroll et al. (Trochanteric Management): This literature emphasizes the importance of the articulotrochanteric distance (ATD). Their work guides the concurrent management of the greater trochanter (via epiphysiodesis or transfer) during valgus osteotomy to optimize abductor mechanics and resolve the Trendelenburg gait.
In summary, valgus osteotomy for developmental coxa vara is a highly effective, biomechanically sound intervention. By meticulously adhering to the principles of restoring the NSA, horizontalizing the physis to an HEA of less than 38 degrees, and optimizing the abductor lever arm, the orthopedic surgeon can reliably restore hip health, prevent premature osteoarthritis, and alter the natural history of this challenging pediatric deformity.
Clinical & Radiographic Imaging
You Might Also Like