Ulnar Tunnel Syndrome & Stenosing Tenosynovitis Surgery
Key Takeaway
Ulnar tunnel syndrome and stenosing tenosynovitis represent common yet anatomically complex compressive neuropathies and tendinopathies of the hand and wrist. Successful surgical management requires a profound understanding of local biomechanics, anatomical variations—such as aberrant tendons in de Quervain disease—and precise surgical execution. This guide details the pathophysiology, diagnostic criteria, and step-by-step operative techniques for ulnar nerve decompression, first dorsal compartment release, and trigger digit management.
ULNAR TUNNEL SYNDROME (GUYON'S CANAL)
Ulnar tunnel syndrome is a compressive neuropathy of the ulnar nerve occurring within a tight, triangular fibro-osseous tunnel at the level of the carpus, commonly referred to as Guyon's canal. While it shares pathophysiological similarities with median nerve compression in the carpal tunnel, ulnar tunnel syndrome is significantly less common. This is primarily because the anatomical space occupied by the ulnar nerve at the wrist is more yielding, and the ulnar nerve is more frequently constricted proximally at the cubital tunnel of the elbow.
Applied Anatomy and Biomechanics
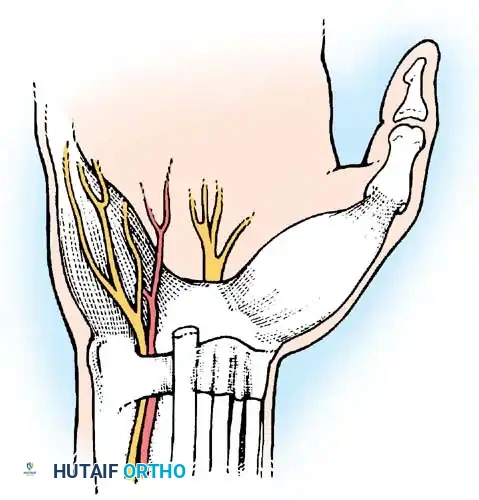
The ulnar tunnel is approximately 1.5 cm in length. A precise understanding of its boundaries is critical for safe surgical decompression:
* Anterior (Roof): Superficial transverse carpal ligament and the palmaris brevis muscle.
* Posterior (Floor): Deep transverse carpal ligament and the hypothenar aponeurosis.
* Medial (Ulnar Border): Pisiform bone and the pisohamate ligament.
* Lateral (Radial Border): Hook of the hamate.
Fig. 73-8 Anatomical relationships of structures within the ulnar tunnel.
Clinically, Guyon's canal is divided into three distinct zones, which dictate the presentation of motor and sensory symptoms:
* Zone 1: Proximal to the bifurcation of the ulnar nerve. Compression here yields mixed motor and sensory deficits.
* Zone 2: Encompasses the deep motor branch after bifurcation. Compression results in isolated motor weakness of the intrinsic hand muscles (excluding the hypothenar muscles, which are supplied proximally).
* Zone 3: Encompasses the superficial sensory branch. Compression yields isolated sensory deficits to the volar ulnar aspect of the hand and the ulnar one and a half digits.
Etiology and Pathophysiology
Unlike carpal tunnel syndrome, which is often idiopathic, ulnar tunnel syndrome is frequently driven by a distinct space-occupying lesion or identifiable trauma.
* Mass Lesions: Ganglion cysts (most common non-traumatic cause) and lipomas.
* Vascular Pathologies: True or false aneurysms of the ulnar artery (often associated with Hypothenar Hammer Syndrome), or thrombosis of the ulnar artery.
* Trauma: Fractures of the hook of the hamate with associated hemorrhage and edema.
* Anatomical Variations: Aberrant muscles, such as an accessory abductor digiti minimi.
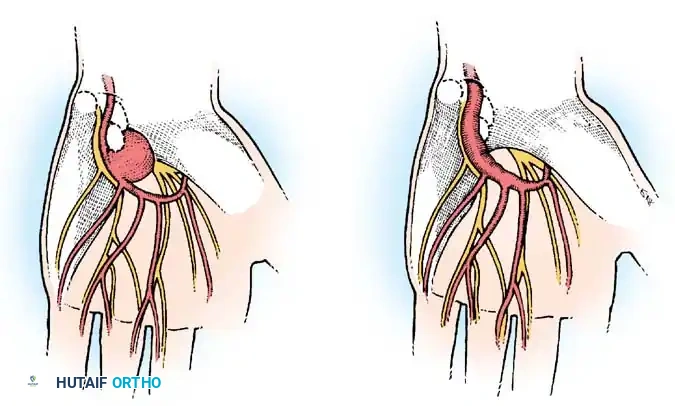
Fig. 73-9 Two types of traumatic aneurysms of the ulnar artery in the hand. A, Saccular “false” aneurysm. B, “True” fusiform aneurysm.
Clinical Pearl: In patients presenting with rheumatoid arthritis, it is not uncommon for carpal tunnel and ulnar tunnel syndromes to develop concomitantly in the same hand due to severe tenosynovial proliferation. Always evaluate both nerve distributions.
Differential Diagnosis
A meticulous clinical examination is required to differentiate ulnar tunnel syndrome from proximal pathologies. The differential diagnosis must include:
* Cervical radiculopathy (C8-T1 herniation)
* Thoracic outlet syndrome (TOS)
* Cubital tunnel syndrome
* Peripheral neuropathy (diabetic, alcoholic, or idiopathic)
Surgical Management: Ulnar Nerve Decompression
Treatment consists of surgical exploration of the ulnar nerve at the wrist and the meticulous removal of any compressive etiology.
Surgical Steps:
1. Positioning and Anesthesia: The patient is positioned supine with the arm on a hand table. The procedure can be performed under regional anesthesia or Wide Awake Local Anesthesia No Tourniquet (WALANT). If a tourniquet is used, exsanguinate the limb prior to inflation.
2. Incision: A curvilinear incision is made over the volar-ulnar aspect of the wrist, extending from the proximal wrist crease, passing just ulnar to the palmaris longus, and curving distally toward the hypothenar eminence.
3. Superficial Dissection: The superficial palmar fascia and the palmaris brevis muscle are divided. Care must be taken to identify and protect the ulnar artery, which lies radial to the nerve.
4. Decompression: The superficial transverse carpal ligament is incised. The ulnar nerve is identified and traced distally to its bifurcation.
5. Deep Branch Exploration: If Zone 2 compression is suspected, the deep motor branch must be traced as it dives between the abductor digiti minimi and the flexor digiti minimi brevis, passing through the pisohamate hiatus. The fibrous arch of the hypothenar muscles is released.
6. Vascular Management: Should the ulnar artery be occluded for several millimeters, Raynaud syndrome may be produced in the ulnar three digits because the sympathetic nerve fibers to these digits pass along the ulnar artery. Segmental resection of the occluded section and replacement with a vein graft is the preferred procedure when feasible.
Postoperative Protocol:
Symptoms are usually relieved promptly, though weakened or atrophic intrinsic muscles may require 3 to 12 months to recover. Early active range of motion (ROM) of the digits is encouraged to prevent perineural adhesions.
STENOSING TENOSYNOVITIS
Stenosing tenosynovitis occurs more frequently in the hand and wrist than anywhere else in the human body. The condition arises from a volumetric mismatch between a tendon and its surrounding fibrous sheath.
The stenosis typically occurs at anatomical transition points where the direction of a tendon changes. At these junctures, a fibrous sheath acts as a pulley, maximizing friction. While the tenosynovium normally lubricates the sheath, repetitive friction—often seen in occupational hazards (e.g., carpenters, assembly line workers)—provokes a hypertrophic inflammatory reaction.
Surgical Warning: Before initiating corticosteroid injections, the clinician must definitively rule out atypical causes of tenosynovitis, such as gout, crystalline arthropathy, or atypical mycobacterial infections, which could be catastrophically exacerbated by localized immunosuppression.
Anatomical visualization of the flexor tendon sheath and pulley system, highlighting areas prone to stenosing tenosynovitis.
DE QUERVAIN DISEASE
When the extensor pollicis brevis (EPB) and the abductor pollicis longus (APL) tendons in the first dorsal compartment are affected, the condition is termed de Quervain disease, named after the Swiss physician who first described it in 1895.
Demographics and Clinical Presentation
De Quervain disease typically affects adults between 30 and 50 years of age, with a striking female-to-male predominance of 6:1 to 10:1. It is frequently associated with overuse, postpartum periods (due to lifting infants), or rheumatoid arthritis.
Patients present with insidious or acute pain and tenderness localized to the radial styloid. A palpable thickening of the fibrous sheath is often present.
The Finkelstein Test:
Often considered pathognomonic, the Finkelstein test is performed by having the patient grasp their thumb within their palm, followed by the examiner quickly ulnar-deviating the hand. Excruciating pain over the radial styloid constitutes a positive test. However, this must be differentiated from:
* Trapeziometacarpal (CMC) arthritis
* Scaphotrapeziotrapezoid (STT) arthritis
* Superficial radial nerve entrapment (Wartenberg's syndrome)
* Intersection syndrome (tenosynovitis at the crossing of the first and second dorsal compartments)
Pathoanatomy and Anatomical Variations
Surgical success in de Quervain disease hinges entirely on recognizing anatomical variations within the first dorsal compartment.
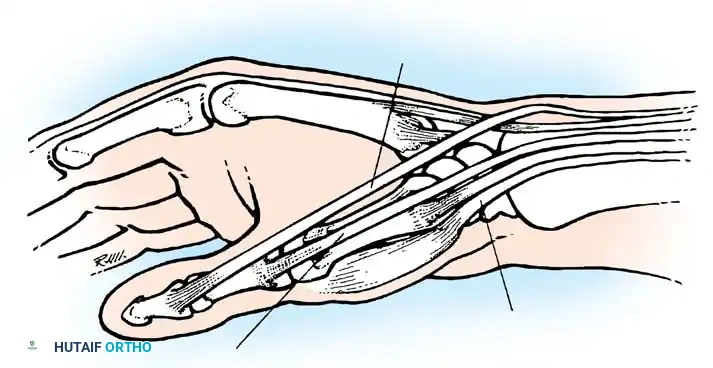
Fig. 73-10 Often, the abductor pollicis longus inserts on the trapezium and the base of the first metacarpal through two or more tendons. During surgery, aberrant tendons are frequently encountered.
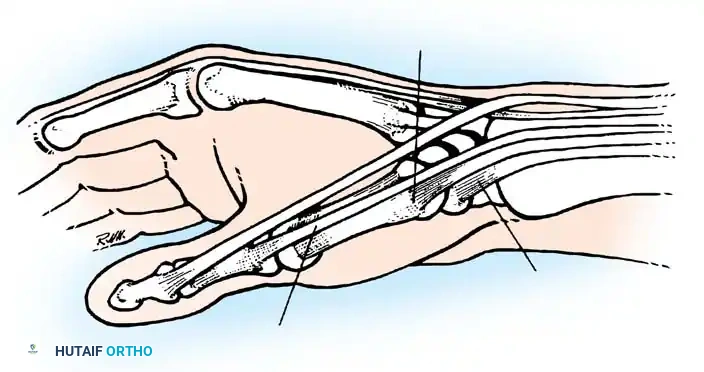
Fig. 73-11 In rare cases, the abductor pollicis longus inserts on the fascia of the abductor pollicis brevis and the base of the first metacarpal.
- Septation: A longitudinal septum subdivides the first compartment in 44% to 73% of wrists. Failure to recognize and release the separate sub-compartment housing the EPB is the leading cause of surgical failure.
- Aberrant Tendons: More than half of patients possess duplicated or "aberrant" APL tendons, which may insert proximally into the trapezium, the abductor pollicis brevis muscle, or the opponens pollicis.
Nonoperative Management
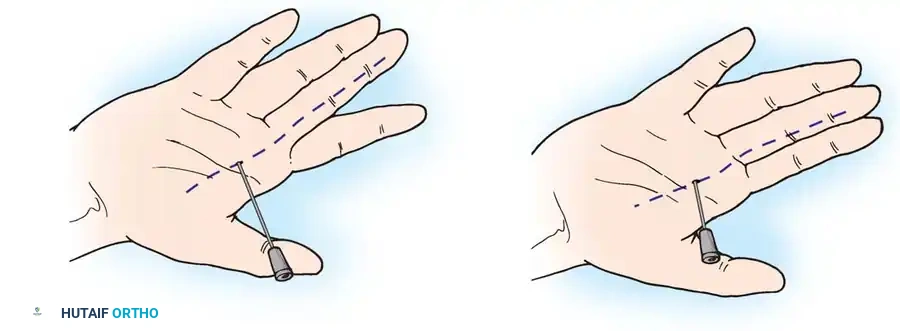
Conservative treatment is highly effective if initiated within the first 6 weeks of symptom onset. It consists of thumb spica splinting and corticosteroid injection into the tendon sheath. Studies indicate that up to 71.4% of patients achieve complete pain relief after a single injection, with an additional subset responding to a second injection.
Technique for corticosteroid injection into the affected tendon sheath. The patient must be warned of a temporary increase in pain for 24 hours post-injection.
Surgical Technique: First Dorsal Compartment Release (Technique 73-4)
When conservative measures fail, surgical release is indicated.
- Preparation: Use a local anesthetic (WALANT is highly effective here) and a tourniquet if desired. Infiltrate the skin over the first dorsal compartment.
- Incision: Make a transverse-to-oblique skin incision parallel to the skin creases over the area of maximal tenderness.
> Surgical Warning: Avoid longitudinal incisions. They cross the flexion creases perpendicularly, leading to hypertrophic scarring and a higher risk of adherence to the underlying superficial branch of the radial nerve (SBRN). - Superficial Dissection: Carry sharp dissection only through the dermis. Use blunt dissection (e.g., with tenotomy scissors) in the subcutaneous fat to identify and meticulously protect the sensory branches of the SBRN, which usually lie deep to the superficial veins.
- Compartment Release: Identify the tendons proximal to the stenosing dorsal ligament. Open the first dorsal compartment on its dorsoulnar aspect.
- Verification: With the thumb abducted and the wrist flexed, lift the APL and EPB tendons from their groove. If they do not glide freely, aggressively search for a separate EPB compartment or aberrant APL slips.
- Closure: Close the skin only. Apply a small pressure dressing.
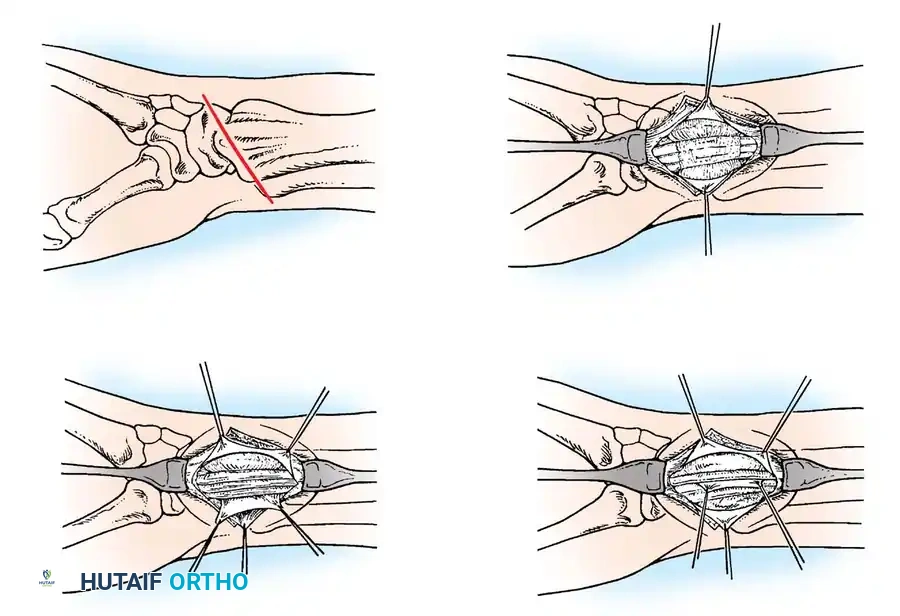
Fig. 73-12 Surgical treatment of de Quervain disease. A, Transverse skin incision. B, Dorsal carpal ligament exposed. C, First dorsal compartment opened on its ulnar side. D, Identification of separate compartments for the EPB and APL tendons.
Complications and Salvage Procedures
Failure to obtain complete relief may result from:
1. Iatrogenic neuroma of the SBRN.
2. Failure to release a septated EPB compartment.
3. Volar subluxation of the tendons (caused by excessive volar release of the retinaculum).
Management of Tendon Subluxation:
If the tendons subluxate volarward over the radial styloid during wrist flexion, reconstruction of the retinaculum is required.
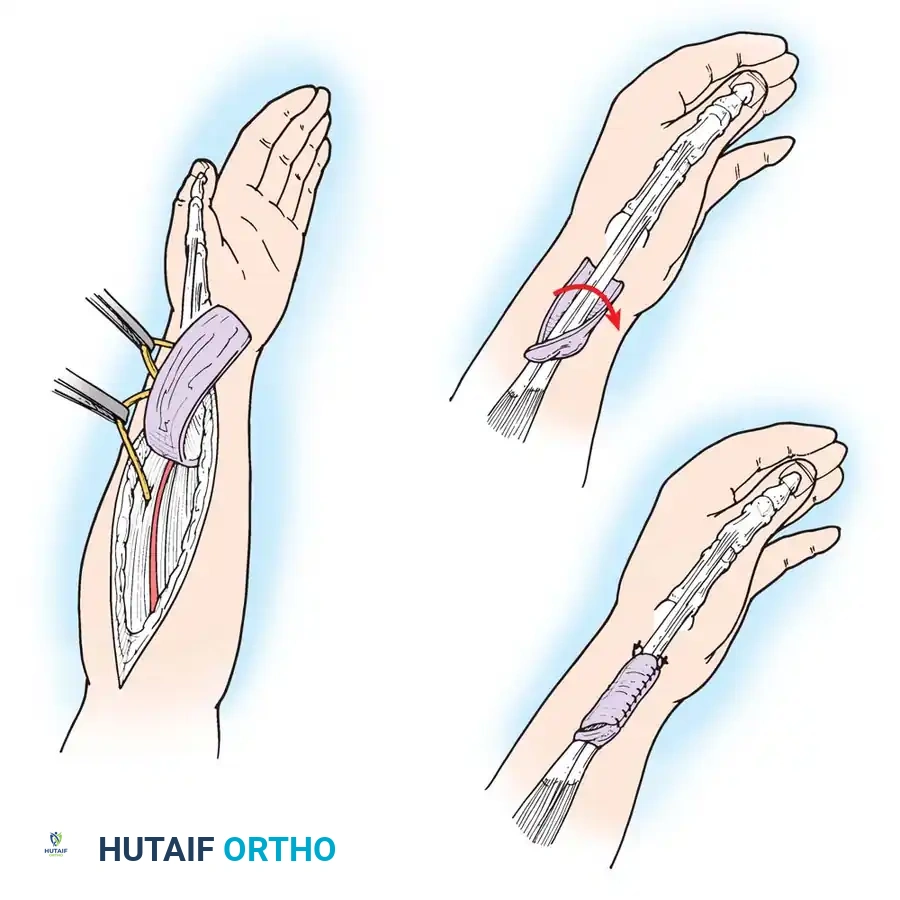
* Ramesh and Britton Technique: Utilizes a slip of the extensor retinaculum to create a U-shaped sling.
* Littler Technique: The septum dividing the compartment is excised, and the retinacular sheath is loosely reapproximated over the APL to prevent subluxation while allowing the EPB to remain free.
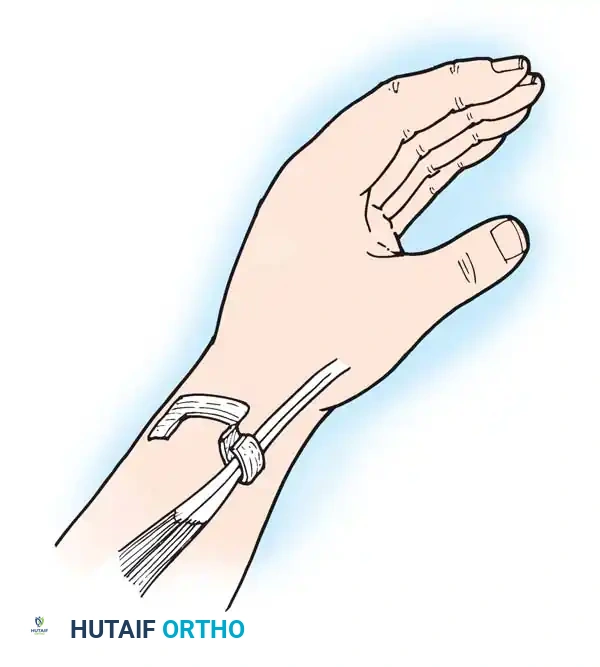
Fig. 73-13 Part of the extensor retinaculum is used to create a U-shaped sling to retain the tendons of the extensor pollicis brevis and abductor pollicis longus.
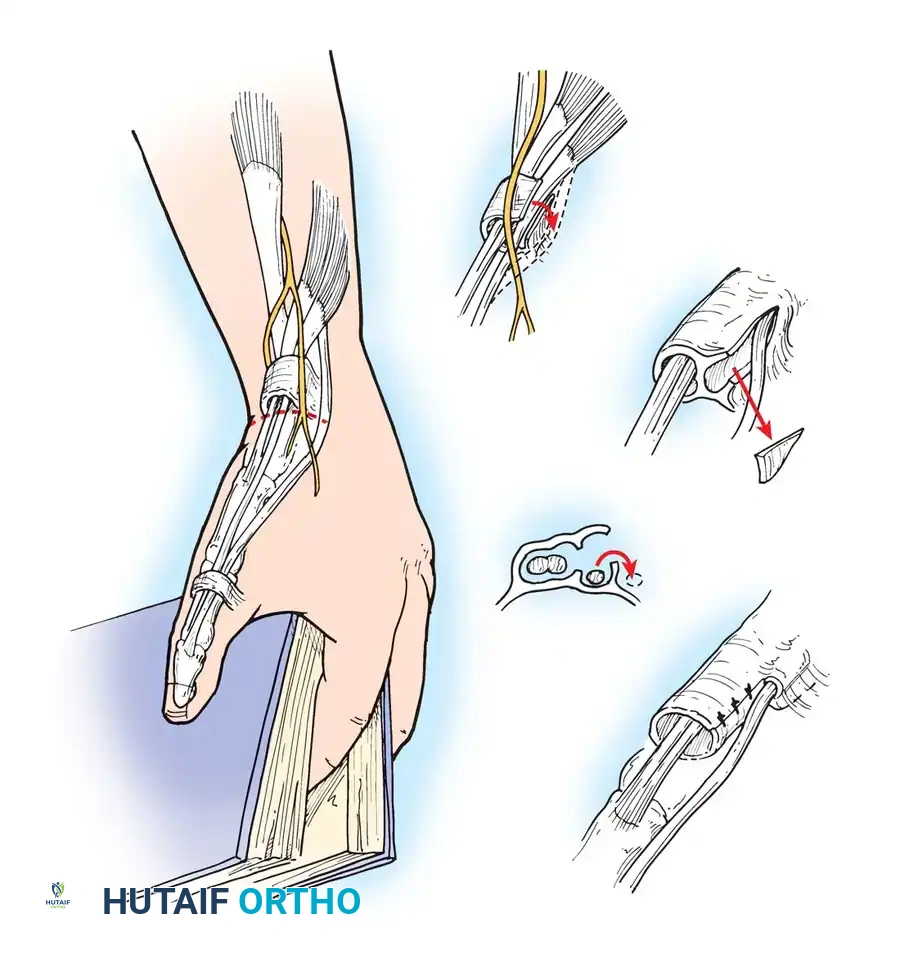
Fig. 73-14 Technique of Littler et al. for reconstruction of the first extensor compartment. The superficial radial nerve is protected, and the retinacular sheath is incised along the dorsoulnar margin.
TRIGGER FINGER AND THUMB (FLEXOR TENOSYNOVITIS)
Trigger digit in adults is a distinct entity from congenital trigger thumb. It presents as an inability to smoothly extend a flexed digit, resulting in a painful "snapping" or "triggering" phenomenon. It is most commonly seen in patients over 45 years of age, with a higher prevalence in diabetic and rheumatoid populations. The long and ring fingers are most frequently involved.
Pathophysiology and Clinical Findings
The primary site of pathology is the first annular (A1) pulley of the flexor tendon sheath, located at the level of the metacarpophalangeal (MCP) joint. Tenosynovial proliferation leads to a localized thickening or a fusiform nodule within the flexor tendon.
During digital flexion, this nodule is pulled proximally through the A1 pulley. Upon attempted extension, the nodule catches at the proximal edge of the pulley, requiring increased force to pull it through, which results in the characteristic snap.
Demonstration of the flexor tendon nodule catching at the proximal edge of the A1 pulley during dynamic digital motion.
On examination, a tender nodule is often palpable in the distal palmar crease (for fingers) or the MCP flexion crease (for the thumb). The nodule moves synchronously with the flexor tendon.
Surgical Management
When conservative management (splinting, NSAIDs, and corticosteroid injections) fails, surgical release of the A1 pulley is highly curative.
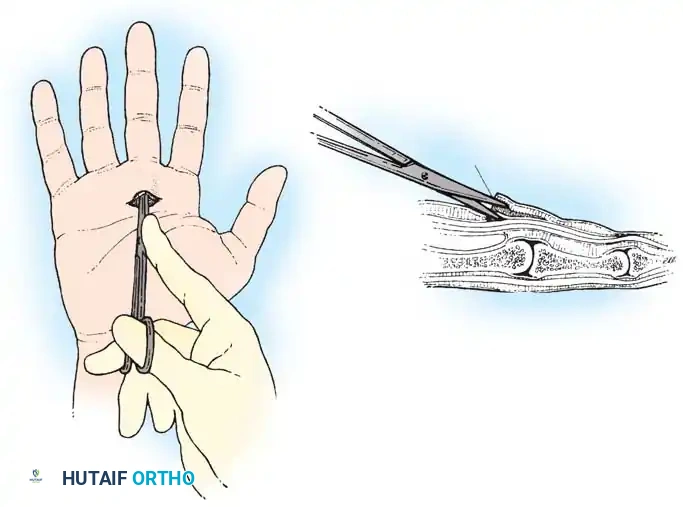
Surgical release of the A1 pulley. Blunt dissection is utilized to protect the adjacent neurovascular bundles before the pulley is longitudinally incised.
Operative Technique:
1. Incision: A transverse or oblique incision is made in the palm over the affected A1 pulley. For the thumb, the incision is made at the MCP flexion crease.
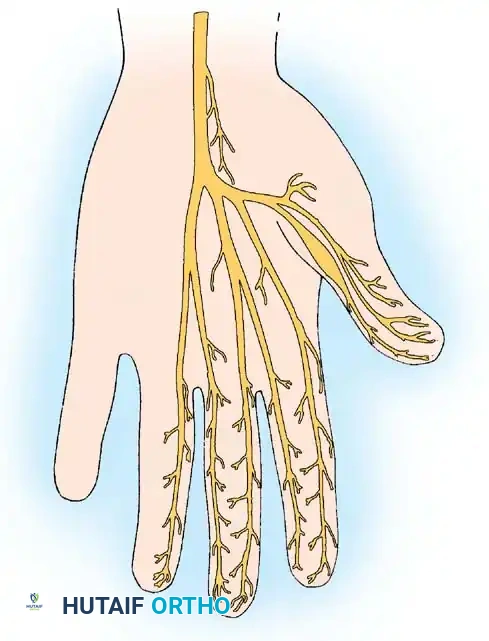
2. Dissection: Subcutaneous tissues are bluntly spread to protect the digital neurovascular bundles. Special care must be taken in the thumb, as the radial digital nerve crosses obliquely over the flexor sheath just proximal to the A1 pulley.
3. Pulley Release: The A1 pulley is identified and longitudinally incised under direct vision.
4. Dynamic Assessment: The patient (if under WALANT) is asked to actively flex and extend the digit to confirm complete resolution of the triggering.
5. Closure: The skin is closed, and early active motion is initiated immediately postoperatively to prevent tendon adhesions.
Surgical Pitfall: In rheumatoid patients, a nodule distal to the A1 pulley may cause triggering at the A2 pulley or the decussation of the FDS. Releasing the A1 pulley alone in these patients may not resolve the symptoms, and a flexor tenosynovectomy may be required. Furthermore, persistent triggering after A1 release can occasionally be caused by the tendon catching on the transverse fibers of the palmar aponeurosis.
You Might Also Like
